OBJECTIVE: To evaluate the influence of a secondary task on foot pedal reaction time, movement time and total response time in patients with transtibial amputation.
DESIGN: Controlled trial without randomization.
SUBJECTS: Ten patients with transtibial amputation and 13 age-matched controls.
METHODS: Foot pedal reaction time and movement time were measured for both legs under simple and dual-task conditions.
RESULTS: While mean simple reaction time was similar for both groups (258 (standard deviation (SD) 53) vs 239 (SD 34) ms), a group by reaction time condition interaction (p < 0.05) identified a disproportionately greater mean dual-task effect among patients with transtibial amputation (432 (SD 109) vs 317 (SD 63) ms), apparently affecting the prosthetic and intact legs equally (426 (SD 110) vs 438 (SD 107) ms). Among patients with transtibial amputation faster movement time was achieved with the intact leg (185 (SD 61) vs 232 (SD 58) ms, p < 0.0001). Compared with controls, patients with transtibial amputation demonstrated impaired mean movement time (142 (SD 37) vs 208 (SD 64) ms, p < 0.001) and total response time (420 (SD 80) vs 552 (SD 151) ms, p < 0.001) regardless of reaction time condition.
CONCLUSION: This study appears to have identified a functional manifestation of central reorganization following transtibial amputation, affecting the prosthetic and intact lower limbs equally.
Key words: amputation; automobile driving; reaction time; neuronal plasticity.
J Rehabil Med 2011; 00: 00–00
Correspondence address: Tim Pauley, West Park Healthcare Centre, 82 Buttonwood Ave. Toronto, ON, Canada, M6M 2J5, Canada. E-mail: Tim.pauley@westpark.org
Submitted March 10, 2011; accepted July 21, 2011
INTRODUCTION
The ability to execute foot movements quickly and accurately is integral to successful foot placement during loss of balance or when operating a motor vehicle. While foot pedal reaction time (RT) of patients with lower-limb amputation has been examined previously, the investigation was limited to identifying which foot pedal operation techniques elicit the fastest braking responses among patients with unilateral, right transtibial amputation (TTA) (1). While this study showed faster RT of the left intact leg relative to the right amputated leg, the experimental protocol provided an ideal environment free from the types of distracting stimuli that characterize the real-world operation of a motor vehicle. It is highly unlikely that individuals consciously focus their attention on the activities of the lower limbs while driving. Rather, attention is shared between the activities of the body and its immediate environment while driving (e.g. navigational cues, vehicle traffic patterns, speed, etc.). Indeed, it has been demonstrated previously that RT is significantly impaired in the presence of a secondary cognitive task (2) and that this dual-task effect is also present in driving RT tests (3, 4).
Consideration of the dual-task implications of a cognitive task for the safe operation of a motor vehicle is particularly relevant for patients who have undergone limb amputation, as previous research suggests that the consequences of limb amputation is not solely a peripheral phenomenon, but probably involves central reorganization. For example, among patients with amputation it has been demonstrated that phantom sensation can be eliminated by lesions of the post-central gyrus or parietal cortex (5–7) and that the receptive field of the lost digits can relocate to the face (8, 9). The functional implications of central involvement following lower limb amputation have been demonstrated previously in studies of dual-task interference. Compared with able-bodied controls, patients with amputation have demonstrated greater dual-task effects during quiet stance (10), while weight shifting during bipedal stance (11), while stepping in place (12) and during obstacle avoidance task while walking on a treadmill (13). The majority of these previous investigations have focused on the effects of a concurrent task on static or dynamic postural control. One study, however, focused on RT as an outcome while subjects were asked to either stand quietly or perform a stepping-in-place task (12). Both controls and patients with amputation demonstrated significantly impaired auditory RT (subjects asked to say “pa” in response to an auditory stimulus) during the stepping task compared with the standing task (p < 0.01 for all). Though the authors did not confirm the result statistically, patients with TTA (mean 271.0 (SD 32.6) ms) and transfemoral amputation (mean 273.3 (SD 73.4) ms) appeared to demonstrate larger dual-task effects than controls (mean 237.4 (SD 29.2) ms) during the stepping task, which the authors argue is less automatized than quiet stance and therefore demanding of greater attention. Though apparently maladaptive, it has been argued that dual-task effects, which are manifest bilaterally among patients with unilateral amputation, may demonstrate an adaptive response of the central nervous system (CNS) to re-establish synchronized activity in both lower limbs (13).
While other lines of inquiry have demonstrated an apparently greater susceptibility of patients with amputation to secondary interference when completing a functional task, foot pedal RT in the presence of a secondary task has not been examined previously. Such an approach differs from Nakamura et al. (12), in that a robust motor response, as opposed to a verbal response, is required to move the leg from the brake to the accelerator of a motor vehicle. The purpose of this study is to evaluate the influence of a secondary cognitive task on foot pedal reaction (RT), movement time (MT) and total response time (TRT) among patients with traumatic, unilateral, TTA and age-matched controls.
Hypotheses
The following hypotheses were tested: (i) Compared with controls, TTAs will demonstrate a greater dual-task effect (i.e. delayed RT) in foot pedal RT. (ii) The prosthetic leg of TTAs will consistently demonstrate impaired MT relative to control subjects and the intact leg. (iii)The prosthetic legs of TTAs will consistently demonstrate impaired TRT relative to control subjects and the intact leg.
METHODS
Design
A controlled trial design without randomization was used.
Subjects
Five right and 5 left TTAs (mean age 41.2, SD 6.3 years) were recruited from West Park Healthcare Centre, a tertiary rehabilitation centre, and from the Prosthetics and Orthotics program at Sunnybrook Health Sciences Centre, in Toronto, ON, Canada. Potential subjects were identified in consultation with the treating physiatrist at West Park Healthcare Centre and the prosthetic coordinator at Sunnybrook Health Sciences Centre. TTA subjects were determined appropriate for study inclusion if they had sustained a localized traumatic right or left TTA, their age was between 18 and 55 years, and they were at least 12 months post-initial prosthetic fitting (to ensure adequate familiarity with the prosthesis). TTA subjects were excluded from recruitment if multiple traumas were sustained at the time of the event that led to amputation, thus accidents that may have involved a head injury (e.g. motor vehicle accident) precluded study participation. Mean Houghton score was 8.1 (SD 1.3), suggesting these were highly functional individuals in terms of prosthetic usage (14). Thirteen control subjects (mean age 38.8, SD 2.9 years) were recruited from each centre and through word of mouth. Control subjects had to be free from physical disability and between 18 and 55 years of age. Experimental and control subjects were screened for history of neurological, musculoskeletal, visual or vestibular disorders; dizziness; and use of drugs/medications that may impair cognitive function. All experimental and control subjects were right-leg dominant. Subject demographics and clinical data are presented in Table I.
|
Table I. Demographic and clinical data of study participants (n=23)
|
|
Characteristics
|
Amputees (n = 10)
|
Controls (n = 13)
|
|
Gender, n (%)
|
|
|
|
Male
|
8 (80)
|
9 (69)
|
|
Age, years, mean (SD)
|
41.2 (6.3)
|
38.8 (2.9)
|
|
BMI
|
26.3 (3.2)
|
22.8 (3.6)
|
|
Side of amputation, n (%)
|
|
|
|
Right
|
5 (50)
|
N/A
|
|
Time since amputation years, mean (SD)
|
10.2 (8.2)
|
N/A
|
|
Cause of amputation, n (%)
|
|
|
|
Crush injury
|
8 (80)
|
N/A
|
|
Mechanical equipment injury
|
2 (20)
|
N/A
|
|
Houghton score, mean (SD)
|
8.1 (1.3)
|
N/A
|
|
BMI: body mass index; N/A: not applicable.
|
Apparatus
The apparatus utilized in this study included a MOART Reaction Time/Movement Time system and 3 foot switches (Lafayette Instruments Company, Lafayette, USA). The foot pedals measure 65 mm wide, 90 mm long and 20 mm thick. The switches were mounted in parallel atop a wooden platform with the tops of the switches 60 mm above the floor, such that subjects were able to rest their heels comfortably on the floor while depressing the start pedal. Measured from centre to centre, the pedals were spaced at a distance of 135 mm from one another. Pedal travel (from bottom to top position) was 6 mm. Seat height was adjusted to ensure that the thighs were parallel to the ground, while the distance from the seat to the pedals was adjusted to achieve a 90º angle at the knee.
Procedures
Foot pedal RT and MT were measured for the prosthetic and intact legs of experimental subjects and left and right legs of controls. Each group completed one block of 20 trials under simple RT conditions and 1 block of 20 trials while simultaneously performing a cognitively demanding secondary task (dual-task condition) consisting of counting backward by serial 3s from 100, 99, or 98. Each block consisted of 10 trials with the right foot and 10 trials with the left foot. To eliminate a training effect, ordering of left vs right foot was randomized from trial to trial. All subjects completed the simple RT trials first, followed by the dual-task trials. In addition, 5 catch trials (i.e. no stimulus) were randomly distributed throughout each block of 20 test trials, to further reduce anticipation of the arrival of the stimulus. Subjects were provided with 4 practice trials for each foot and for each condition. For the dual-task condition, subjects were given the opportunity to practice the counting task prior to commencing the test trials. Subjects were provided a 5-min break between simple and dual-task blocks of trials.
Subjects were asked to depress the start pedal fully at the beginning of each trial. For the right foot condition, the right foot was placed on the right-most switch. For the left foot condition, the left foot was placed on the left-most switch. An auditory stimulus signaled the subject to release the start switch, move the foot medially and depress the middle switch. There was a 3–10 s delay from the start of the trial to the arrival of the auditory stimulus. The length of the delay was randomized from trial to trial to eliminate anticipation. Measurement of RT commenced with the onset of an auditory stimulus and terminated when the subject’s foot lifted off the start pedal. Measurement of MT commenced when the subject began to release the start pedal and terminated when the subject’s foot had fully depressed the middle pedal. Total response time was the sum of RT and MT. Outcome measures included RT, MT and TRT.
This study was approved by the research ethics boards at West Park Healthcare Centre and Sunnybrook Health Sciences Centre.
Analysis
Descriptive statistics were used to summarize the data. Data were rank-transformed prior to inferential statistical analysis, to avoid violating the underlying assumptions of the analysis of variance (ANOVA). Repeated measures ANOVA (RM ANOVA) were conducted to compare RT, MT and TRT for 2 levels of the between-subjects factor “group” (controls vs TTAs) and 2 levels of the within-subject factor “RT condition” (simple RT vs dual-task RT). Three additional RM ANOVAs were conducted within TTAs to compare RT, MT and TRT for 2 levels of the within-subjects factor “leg” (prosthetic leg vs intact leg) and 2 levels of the within-subject factor “RT condition” (simple RT vs dual-task RT). SAS for Windows, Version 9.1 was used to conduct the analyses.
RESULTS
Mean RT, MT and TRT for simple and dual-task conditions for both groups has been provided in Table II. Sixteen trials were excluded due to inappropriate foot pedal operation (e.g. subject hit their foot against the side of the brake pedal), thus 904/920 trials were included in the analysis.
|
Table II. Reaction (RT), movement and total response times for simple and dual-task conditions
|
|
|
Simple RT, Mean (SD)
|
Dual-task RT
Mean (SD)
|
|
Reaction time
|
|
|
|
Controls
|
239 (34)
|
317 (63)
|
|
Intact leg
|
260 (54)
|
438 (107)
|
|
Prosthetic leg
|
255 (51)
|
426 (110)
|
|
Movement time
|
|
|
|
Controls
|
141 (40)
|
142 (34)
|
|
Intact leg
|
180 (59)
|
191 (63)
|
|
Prosthetic leg
|
236 (62)
|
227 (53)
|
|
Total response time
|
|
|
|
Controls
|
381 (59)
|
460 (79)
|
|
Intact leg
|
440 (94)
|
629 (146)
|
|
Prosthetic leg
|
491 (56)
|
653 (142)
|
Comparison of patients with amputation vs controls
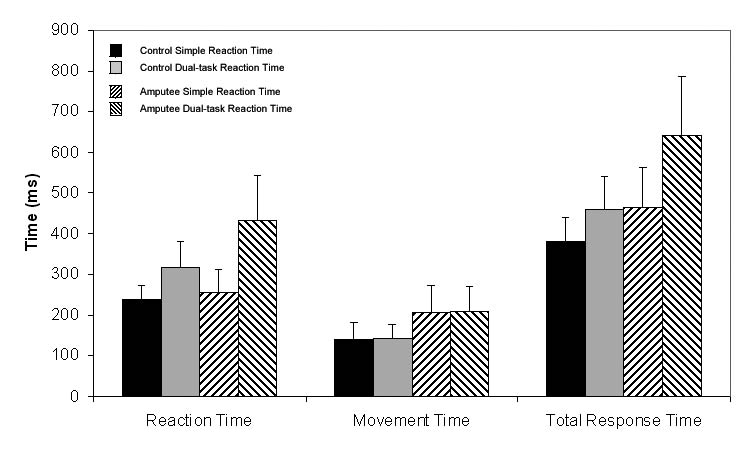
RT, MT and TRT results for TTAs and controls for each “RT condition” are presented in Fig. 1. A significant “group” main effect indicated that TTAs demonstrated consistently impaired mean RT (343 (SD 122) vs 278 (SD 64) ms, p < 0.001), mean MT (208 (SD 64) vs 142 (SD 37) ms, p < 0.001) and mean TRT (552 (SD 151) vs 420 (SD 80) ms, p < 0.001) relative to controls. Likewise, a significant “RT condition” main effect indicated that the presence of a dual-task impaired both mean RT (366 (SD 103) vs 247 (SD 44) ms, p < 0.0001) and mean TRT (537 (SD 143) vs 417 (SD 89) ms, p < 0.0001), but not mean MT (171 (SD 58) vs 170 (SD 62) ms, p = 0.41). However, the RM ANOVA main effects for “group” and “RT condition” obscured the relatively greater dual-task interference demonstrated by TTAs, as evidenced by the significant “group” by “RT condition” interaction (p < 0.05). While the inclusion of a dual-task had the effect of impairing mean RT for both controls (317 (SD 63) vs 239 (SD 34) ms) and TTAs (432 (SD 109) vs 258 (SD 53) ms), the additional time required to begin the movement by TTAs in the dual-task condition was 123% greater than controls (174 vs 78 ms). It is notable that RT of the 2 groups were very similar in the simple RT condition, with TTAs demonstrating an 8% delay in mean RT relative to controls (258 vs 239 ms) compared with a 36% delay in the dual-task mean RT condition (432 vs 317 ms).
Fig. 1. Reaction, movement and total response times for simple and dual-task reaction time conditions for patients with transtibial amputation and controls. Error bars indicate standard deviation.
Comparison of intact and prosthetic legs of patients with amputation
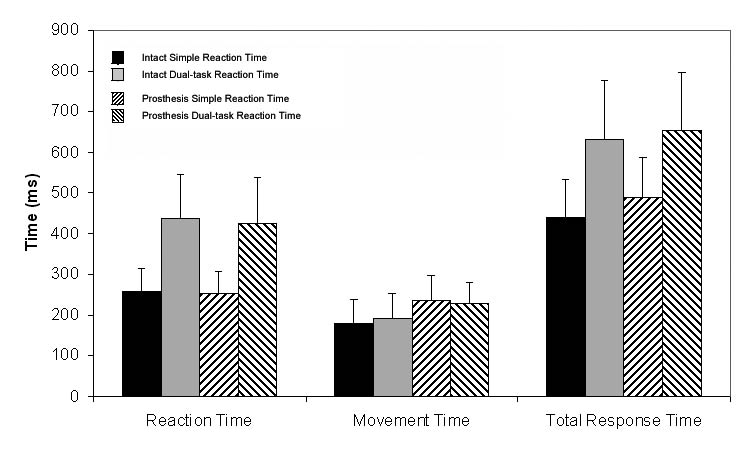
RT, MT and TRT results for the intact and prosthetic legs of TTAs for each “RT condition” are presented in Fig. 2. Separating the intact and prosthetic legs of TTAs allowed a comparison of the relative contribution of each leg to overall RT, MT and TRT. The absence of a significant main effect for “leg” (intact vs prosthetic) is particularly notable. In spite of a clear unilateral physical impairment, there was no between-leg difference when comparing mean RT of the prosthetic and intact legs (339 (SD 121) vs 348 (SD 122) ms, p = 0.19), though the effect of amputation-related impairment were clearly demonstrated in terms of MT, which was significantly impaired on the prosthetic side compared with the intact leg (232 (SD 58) vs 185 (SD 61) ms, p < 0.0001). As expected, RT was significantly impaired in the presence of a dual-task (432 (SD 109) vs 258 (SD 53) ms, p < 0.0001), although the presence of a dual-task did not translate to a delay in MT (209 (SD 61) vs 207 (SD 66) ms, p = 0.82).
Regarding TRT, there was a significant main effect for “leg” demonstrating impaired TRT of the prosthetic leg compared with the intact leg (571 (SD 145) vs 533 (SD 155) ms, p < 0.005), resulting largely from the delayed MT of the prosthetic leg. Likewise, there was a significant main effect for “RT condition” demonstrating impaired TRT under the dual-task condition compared with the simple RT condition (641 (SD 144) vs 465 (SD 98) ms, p < 0.0001), resulting largely from the delayed RT associated with the dual-task.
Fig. 2. Reaction, movement and total response times for simple and dual-task reaction time conditions for intact and prosthetic legs of patients with transtibial amputation. Error bars indicate standard deviation.
There was a trend toward a significant “leg” by “RT condition” interaction (p = 0.06) for TRT. In the simple RT condition the prosthetic leg demonstrated a 12% delay in RT relative to the intact leg (491 (SD 96) vs 440 (SD 94) ms), although this was reduced to only 4% in the presence of a dual task (653 SD 142) vs 629 (SD 146) ms).
DISCUSSION
Reaction time
The outcome of this study resulted in acceptance of the hypothesis that TTAs would demonstrate a greater dual-task effect than controls. Though controls demonstrated faster overall RT relative to TTAs, the significant “group” by “RT condition” interaction suggests that the between-groups difference is largely a result of the influence of a competing cognitive task, which disproportionately affects RT of TTAs. In the simple RT condition, controls achieved RTs that were 19 ms faster than TTAs, though this difference increased by 6 times, to 115 ms, in the dual-task RT condition.
Of much greater interest was the finding that the prosthetic and intact legs of TTAs demonstrated a similar amount of slowing under the dual-task condition. As these were patients with unilateral amputation who reported no difficulties or injuries to the intact leg, there is no readily apparent reason why the intact leg should be affected by the increased cognitive demand of the dual-task to the same degree as the prosthetic legs.
By convention, RT corresponds to the elapsed time between the presentation of a sensory stimulus and the onset of the overt physical response and depends on the amount of time required to identify the stimulus, select and execute the appropriate motor program, all of which happens at the cognitive control level of the CNS (15). That we found little difference between controls and TTAs on the simple RT task suggests similar central processing characteristics between the two groups. However, the relatively greater impairment of RT among TTAs under the dual-task condition, equally affecting the intact and prosthetic legs, suggests the possibility of central adaptation following amputation. Central involvement accompanying amputation is suggested by studies of phantom limb pain, which has been eliminated following vascular (5, 7) and surgical lesions to post-central gyrus or parietal cortex (6), but not secondary to local anesthesia of the stump or epidural anesthesia (16, 17).
Central reorganization following amputation
Both animal (18, 19) and human models have demonstrated considerable plasticity of the corticospinal system (20–23). Among TTAs, the implications of corticospinal reorganization have yet to be described fully, but may suggest reorganization of a large number of descending motor fibers, which would normally innervate muscles distal to the site of amputation, to innervation of the residual muscle tissues proximal to the amputation. This is supported by the findings of Hall et al. (21), who used electromagnetic stimulation (EMS) of the motor cortex to excite cortico-spinal projections to the intact and amputated arms of 2 patients with congenital amputation, 2 patients with traumatic amputation (4 and 16 years since amputation), and 4 neurologically normal controls. EMG response thresholds were lower on the amputated side compared with the intact leg at all sites (60–90%). In addition, response probability was higher in all muscles of the amputated side, suggesting that muscles on the amputated side were accessible to stimulation of a much larger cortical area than those on the intact side. This was observed only in the 3 individuals for whom a considerable length of time had passed since the time of amputation, but not in the one person whose amputation was 4 years prior to the study, suggesting a delayed time course for onset of cortical reorganization. Taken together, this evidence suggests that corticospinal reorganization occurs in such a manner that the remaining muscles receive a much larger number of descending connections from the motor cortex than the intact side. This is further supported by Kew et al. (24), who, using transcranial magnetic stimulation to determine amplitude of motor evoked potentials (MEP), found MEPs that were, on average, 514% larger in muscles ipsilateral to the amputation relative to responses from homologous muscles of the intact limb. Moreover, abnormal increases in regional cerebral blood flow to the primary motor and somatosensory cortex were detected contralateral to the amputation, regardless of whether the subject moved the intact or amputated limbs. The authors ascribe these findings to increased neuronal excitability.
The larger relative influence from the motor cortex controlling the amputated side may in part explain the relatively larger increase in RT among TTAs during the dual-task condition. While classic theories of central processing and attentional demand assume that attention has a fixed capacity for processing information and that a processing bottleneck occurred at the stimulus identification stage (25, 26), more recent theories allow for multiple channels of attention, suggesting that the bottleneck occurs during the response selection stage (27). Given the larger number of descending connections on the amputated side (22, 24), and the correspondingly greater degree of coordination required in programming the motor response, it is reasonable to surmise that execution of the response may be delayed by the competing cognitive load of the counting task more so than during the simple RT condition.
Limb balance restoration via “central recalibration”
One of the more compelling findings of the current study was the contralateral slowing of RT in the dual-task condition, even though the intact limb was neither damaged at the time of amputation nor otherwise physically impaired for any TTAs. Adaptation of sensory thresholds of the homologous areas of the contralateral limb following unilateral injury has been noted following burns (28, 29), arthroplasty (30), carpal tunnel syndrome (31) and digit amputation (32, 33). Only 2 studies have investigated contralateral adaptation following lower limb amputation (34, 35). Following traumatic, unilateral TTA, Kavounoudias et al. (35) found that sensory thresholds of the intact leg were significantly higher for passive movement detection about the knee and plantar touch-pressure sensitivity relative to healthy controls. Within patients with amputation, no between-leg differences were detected for passive movement detection (i.e. equal impairment was demonstrated by the intact and amputated leg). The authors suggest the presence of an adaptive mechanism designed to balance out the perceptive capacities of the amputated and intact legs. Though apparently maladaptive, this “balance of perception” is thought to provide perceptual calibration on each side of the body proximal to the amputation, eliminating perceptual discrepancy between the limbs. This study was not designed, however, to determine whether this central recalibration functions solely on the sensory input side, or on the motor programming side as well.
The currently available evidence regarding central reorganization and central recalibration following amputation clearly suggest that a peripheral insult can profoundly alter afferent feedback from the affected limbs. However, in view of the results of the current study, it is unclear how altered afferent feedback translates to impaired efferent activity, particularly as the stimulus to begin the movement was received not at the periphery, but as an auditory cue, therefore the appropriate response would be expected to be executable independent of afferent feedback. In addition to the auditory cue utilized in the current study, it would have been instructive to include a non-auditory tactile stimulus at a point on the residual limb immediately proximal to the amputation, as well as the homologous structure of the intact limb, to compare the current results to those obtained in a manner dependent on afferent input.
Movement time
As hypothesized, TTAs demonstrated impaired MT of the prosthetic leg relative to the intact leg as well as when compared with controls. This was not unexpected, as patients with amputation tend to adopt an asymmetric stance whereby the majority of body weight is carried over the intact leg, leading to muscle atrophy on the amputated side secondary to disuse (36, 37).
Surprisingly, the intact leg of TTAs also demonstrated slower MT relative to controls for both RT conditions. TTAs were asked if they had experienced any injuries to the intact leg at the time of amputation or since. All reported no such injuries. The most plausible explanation is that impaired MT of the intact leg is probably related to de-training. This is a reasonable suspicion, as many patients with amputation had experienced their amputations as a result of workplace injury and had not returned to work for several years afterwards.
Total response time
As hypothesized, TTAs consistently demonstrated impaired TRT relative to control subjects, though the within-group comparison of the prosthetic and intact legs of TTAs appears to suggest that impaired TRT was specific to the prosthetic leg. Thus, the second part of the hypothesis (i.e. that the prosthetic legs would demonstrate impaired TRT relative to the intact leg) was supported. It was particularly noteworthy that dual-task TRT of controls was not significantly different from simple TRT achieved by TTAs (460 vs 465 ms). This suggests that only when focused solely on the task at hand, are TTAs able to achieve a level of TRT performance comparable to controls concurrently engaged in a cognitively demanding task. On average, relative to the simple RT condition, the dual-task condition caused the TRT of controls subjects to slow by 79 ms, while TRT slowed by 162 ms (205%) and 189 ms (239%) for the prosthetic and intact legs of TTAs, respectively.
The most obvious implications of this study apply to driving a motor vehicle. Where control subjects were able to activate the second pedal in 460 ms, activation of the second pedal by the prosthetic and intact legs of TTAs required 653 and 629 ms, respectively. Assuming a driving scenario where an individual is traveling at 100 km/h and identifies a stimulus requiring a braking response, controls would begin their response after traveling approximately 12.8 m, while TTAs using the prosthetic or intact leg would travel 18.1 and 17.5 m, respectively, for an additional 5.3 and 4.7 m, respectively (approximately equivalent to the vehicle length of a 2011 Toyota Camry). Though seemingly short distances, an additional travel distance of as little as 4.7 m can make the difference between stopping safely and colliding with a stationary vehicle in front. It should be noted that, while the horizontal displacement of the pedals utilized in this study were similar to a regular passenger motor vehicle, pedal travel (i.e. the distance the face of the pedal closest to the subject moves from the neutral position to fully depressed) was only 6 mm compared with several centimeters in a typical passenger vehicle. That is, while the horizontal displacement of the foot in this study was similar to a motor vehicle, the vertical component was much smaller. Therefore, the braking distances provided probably reflect an underestimate of the time required to complete the MT response, though it is nonetheless instructive to provide a real-world example highlighting the apparent disadvantage of TTAs in comparison with controls. Readers should be reminded, however, that RT is but a singular component of driving. The safe operation of a motor vehicle is equally dependent on attention, experience and perceptual and physical fitness, which contribute to the ability to identify and interpret myriad sensory cues, select and execute the appropriate response within the complex and dynamic environment of constantly evolving traffic patterns (38).
Due to the dearth of scientific evidence, the Canadian Medical Association’s Driver’s Guide (7th edition) provides only cursory guidance specific to patients with lower limb amputation (39). These guidelines simply inform clinicians that “People who have an amputation below the knee of one or both legs are usually able to drive any class of motor vehicle safely provided they have full strength and movement in their back, hips and knee joints and a properly fitted prosthesis or prostheses.” Little attention is given, however, to clinical evaluation of the basic skills required to safely operate a motor vehicle. Whereas a clinician may typically recommend installation of a left-sided accelerator or adoption of a left-foot cross-over pedal operation technique for a patient with right TTA, the results of this study suggest that normal function of the intact limb (i.e. comparable to able-bodied controls) cannot be assumed by the clinician. The results of this study would also suggest that left-sided TTAs who resume driving with their intact right leg may, over time, also perform at a level that is slower than able-bodied drivers.
In conclusion, this study appears to have identified a measurable functional manifestation of central reorganization following TTA. Studies describing “central recalibration” as the mechanism by which sensory impairment of the intact leg occurs secondary to contralateral amputation, as well as evidence of reorganization of the motor cortex secondary to changes in the somatosensory cortex, seem to provide an explanation for our finding that the intact leg of TTAs demonstrated impaired RT equal to that of the prosthetic leg. Further examination of central reorganization following amputation is required to establish the time course of adaptation as well as the relative degree of dual-task interference resulting from secondary tasks of varying complexity.
Study limitations
First, no neurophysiological data were collected throughout the course of data collection, so we were not able to investigate neuromuscular activity with respect to movement onset. Rather, the intent of this study was primarily to evaluate functional differences between TTAs and controls in terms of RT. However, we believe that the current study provides a functional demonstration of the role of amputation-induced central reorganization in affecting motor control of the prosthetic and intact legs. Secondly, though all subjects completed the simple RT trials prior to the dual-task trials, there was no apparent evidence of an order-related fatigue effect, as MT was nearly identical for both blocks of trials (171 vs 170 ms). Indeed, among TTAs, MT improved marginally (9 ms) on the prosthetic side. Finally, while the admission profile for all experimental subjects indicated no comorbidities that would be expected to adversely affect the results of this study, no formal cognitive screening tests were conducted at the time of data collection.
ACKNOWLEDGEMENT
This project was funded by a research grant provided by the Workplace Safety and Insurance Board (Ontario).
REFERENCES