OBJECTIVE: To examine the reproducibility, responsiveness and concurrent validity of the six-minute walk test (6MWT) when tested outdoors in patients’ own neighbourhoods using a global positioning system (GPS) or a measuring wheel.
METHODS: A total of 27 chronic stroke patients, discharged to their own homes, were tested twice, within 5 consecutive days. The 6MWT was conducted using a GPS and an measuring wheel simultaneously to determine walking distance. Reproducibility was determined as test-retest reliability and agreement, using the intraclass correlation coefficient, standard error of measurement and Bland & Altman plots. Responsiveness was expressed as the smallest real difference and visualized in Bland & Altman plots. Pearson’s correlation coefficient (r) was used to study concurrent validity between the GPS and measuring wheel.
RESULTS: Intraclass correlation coefficiens were 0.96 for the GPS and 0.98 for the measuring wheel, and standard error of measurement scores were 11.9 m for the measuring wheel and 18.1 m for the GPS, resulting in smallest real differences of 33.0 m and 50.2 m, respectively. Concurrent validity was strong (r = 0.99).
CONCLUSION: These results indicate that the outdoor 6MWT using a GPS or measuring wheel is reproducible, responsive and concurrently valid. This suggests that therapists working in the community can use the outdoor 6MWT as a reliable, responsive and valid test.
Key words: stroke; gait; environment; exercise test.
J Rehabil Med 2011; 00: 00–00
Correspondence address: I. G. L. van de Port, Rehabilitation Center, De Hoogstraat, Center of Excellence, Rembrandtkade 10, 3583 TM Utrecht, The Netherlands. E-mail: i.v.d.port@dehoogstraat.nl
Submitted March 28, 2011; accepted July 21, 2011
INTRODUCTION
Although several prospective cohort studies have shown that approximately 85% of patients who have had a stroke regain gait by 6 months post-stroke (1, 2), approximately 20% of all stroke survivors show significant deterioration in mobility status between 1 and 3 years after stroke (3). Patients’ walking competency after stroke is often assessed with the six-minute walk test (6MWT), which has been recommended (4) as a reliable (5, 6), responsive (7) and valid measure (6). The 6MWT is a uni-dimensional measure that assesses walking endurance when used with a standardized protocol (8). Research has shown that timed walk tests conducted over short distances, such as the 10-m test, tend to overestimate performance on the 6MWT and should complement, but not replace, the 6MWT (9).
Conducting the 6MWT requires appropriate indoor testing facilities, such as a gym or a large corridor in a clinical setting. This means that patients who are treated by physical or occupational therapists at home have to be transported to a gym or outpatient clinic for the appropriate test facilities. To the patient, the transport is not only burdensome, but also expensive. The challenge for the healthcare system is to apply rehabilitation services preferably in the patient’s own environment, and thus to reduce the costs and burden of travel for patients with stroke. As a consequence, the 6MWT needs to be conducted in a valid and reproducible manner in the patient’s own neighbourhood.
Thus far, only a few studies have included stroke survivors performing the 6MWT in various indoor and outdoor environments, such as a suburban street (10, 11), shopping mall (10, 11) and a walkway in a quiet garden (12). However, none of these studies assessed the use of the 6MWT in patients’ own neighbourhood using a global positioning system (GPS) as a potentially innovative tool to determine outdoor walking distance.
The first aim of the present study was to investigate the reproducibility and responsiveness of the 6MWT when tested outdoors in the patients’ own neighbourhoods by using a GPS or a measuring wheel (MW). The second aim was to investigate the concurrent validity of conducting the 6MWT in the stroke survivors’ own neighbourhoods using a GPS compared with an MW.
METHODS
Participants
All participants for the present study were recruited from the FIT-Stroke trial, which is a randomized controlled trial conducted in 9 rehabilitation centres in the Netherlands (13). The FIT-Stroke protocol has been approved by the medical ethics committees of the University Medical Centre Utrecht and all the participating rehabilitation centres, and is registered in the Dutch Trial Register (NTR1534). Eligible patients met the following inclusion criteria: (i) verified stroke according to the World Health Organization (WHO) (2001) definition; (ii) ability to walk a minimum of 10 m without physical assistance from a therapist (i.e. patient may require verbal supervision or stand-by help from a person, and may use an aid or orthotics, but should be classified as Functional Ambulation Category ≥ 3); (iii) discharged home from an inpatient rehabilitation centre; (iv) informed consent and willingness to perform two 6MWTs outdoors at the final assessment of the FIT-Stroke trial (i.e. 24 weeks after randomization). Participants were excluded if they: (i) had severe cognitive deficits as evaluated by the Mini-Mental State Examination (< 24 points); (ii) were unable to communicate (i.e. < 4 points on the Utrechts Communicatie Onderzoek; UCO (14)) or (3) lived more than 30 km from the rehabilitation centre.
Study design
Each recruited participant was invited to perform two 6MWTs in their own neighbourhood. These tests were conducted with an interval of maximally 5 days. Four trained assessors performed the 6MWTs according to a standardized protocol, using Google Earth (GE) to find a appropriate walking course in the patients’ own neighbourhood, and using GPS and a MW to determine the walking distance attained in 6 min.
Testing six-minute walk test in patients’ own neighbourhoods
All assessors were instructed in advance as to how to find a safe and appropriate walking course in the patients’ neighbourhoods using Google Earth. Each assessor was instructed to select an appropriate course, such as a flat pavement, preferably with a length of 30 m, without the need to cross streets. In addition, assessors were only allowed to conduct the 6MWT when the weather was dry. The same course had to be used for the second 6MWT and patients were instructed to use the same shoes during both measurements.
After visually checking the walking course for appropriateness, each assessor used a handheld GPS as well as a hand-driven MW to establish the distance covered during the 6MWTs. The GPS used was a Garmin GPSMAP 60Cx expressing horizontal accuracy by twice the distance root mean squared (2DRMS). The 2DRMS (95%) is 100 metres. The assessors simultaneously pushed a MW (Nedo 703 112) while conducting the 6MWT. The MW had a rubber tyre and a digital counter with a known accuracy of 99.8% (1 cm error) when tested over a distance of 50 m. A stopwatch was used to measure the time taken during the 6MWT.
The 6MWTs in the patients’ own neighbourhoods were conducted following the standardized indoor 6MWT protocol by Guyatt et al. (6). This protocol is known to be a reliable and valid method to measure walking endurance in patients with a compromised walking ability (15, 16), including patients with hemiplegic gait (17–19). During the 6MWTs, all patients received standardized instructions to walk as far as possible at their comfortable pace for 6 min. Running was not allowed. After each minute, the assessor delivered one of a predetermined set of encouraging phrases, such as “You’re doing well” or “Keep up the good work”. At the end of the test the assessor called “Stop”, and the distance walked was recorded. For safety reasons, the assessor walked with the patient to provide the necessary physical assistance if any was needed. To avoid pacing, the assessor walked behind the participant while measuring the distance covered with the GPS and MW.
Reproducibility
Test-retest reliability. Test-retest reliability was defined as the degree to which the measurement error corresponds to the variability between the participants who did the 6MWTs (20). The test-retest reliability of the 6MWT was examined using the intraclass correlation coefficiens (ICC), a two-way random effects model with absolute agreement. This ICCagreement assumes that observers and patients form a random sample of a population and is calculated by the following formula:
ICCagreement = ((BMS-EMS)/k) / ((BMS-EMS/k) + (OMS-EMS/n) + EMS)
where BMS (between-subjects mean square) is the variability between participants, EMS (error mean square) the residual mean square, OMS (observation mean square) the variability between assessors, k the number of assessors and n the number of participants (20). The variables BMS, EMS and OMS were derived from an analysis of variance (ANOVA) table. ICC values less than 0.4 were classified as poor reliability, between 0.4 and 0.75 as fair reliability and greater than 0.75 as excellent reliability (21).
Agreement. Agreement concerns the absolute measurement error, i.e. the degree of correspondence between the distances walked during the first and second 6MWTs (22). The standard error of measurement for agreement (SEMagreement) represented this measurement error as absolute values. SEMagreement was calculated as follows:
SEMagreement=√((OMS-EMS/n) + EMS)
Systematic differences between the two 6MWT distances measured by GPS or MW were investigated with Bland & Altman analysis (23, 24), by plotting the mean difference found between the two consecutive assessments against the standard deviation (SD) of the calculated difference (23), while the limits of agreement were calculated as the mean difference ± 1.96 times the SD of the differences.
Responsiveness
Bland & Altman plots were used to visualize systematic variations around the zero line (25). If Bland & Altman analyses indicate no large systematic differences with regard to the limits of agreement, the smallest real difference (SRD) indicates a real (clinical) improvement or deterioration for a single individual on the basis of the limits of agreement, which were based on the standard error of measurement (SEM) for agreement (26):
SRD = 1.96 * √2 * SEM
Concurrent validity
The concurrent validity of the GPS and MW for measuring the 6MWT was determined by calculating a correlation coefficient. If visual inspection of the outcomes of the 6MWTs revealed a normal distribution, we used Pearson’s correlation coefficient, otherwise a Spearman’s rho. In accordance with Cohen’s classification, a strong association was defined if the coefficient exceeded 0.70, whereas a coefficient between 0.30 and 0.70 was classified as moderate to substantial and a coefficient below 0.30 as a weak association (27).
All data were analysed using SPSS (version 16.0), while all statistical tests were applied two-tailed with a critical p-value of < 0.05.
RESULTS
The main characteristics of the 27 individuals (21 men, 6 women) included in the study are presented in Table I. The age of the participants ranged from 35 to 76 years, while the mean interval between the stroke and the first assessment of the 6MWT was 266 days (SD 38.0 days). Measurements with GPS yielded mean distances for the first and second 6MWTs of 408 m (SD 132 m) and 417 m (SD 139 metres), respectively. Measurements with the MW yielded mean distances of 413 m (SD = 127 m) and 422 m (SD 132 m) for the first and second assessments, respectively (Table II).
| Table I. Participant characteristics (n=27) |
| Variable | |
| Female gender, n (%) | 6 (22) |
| Age, years, mean (SD) | 60.7 (10.9) |
| Height, cm, mean (SD) | 177 (9) |
| Weight, kg, mean (SD) | 81 (16) |
| First stroke, n (%) | 23 (85) |
| Previous stroke, n (%) | 4 (15) |
| Days from stroke to 1st assessment, mean (SD) | 266 (38.0) |
| Days between 1st and 2nd assessments, mean (SD) | 1.5 (1.3) |
| Type of stroke, ischaemic/haemorrhagic strokes, n | 24/3 |
| Hemisphere of stroke, LACI/PACI/TACI/POCI, n | 10/11/0/3 |
| Hemiparetic side, left/right/bilateral, n | 12/13/2 |
| UCO score, 4/5, n | 3/24 |
| FAC score, 3/4/5, n | 1/3/23 |
| LCT score, left/right/none, n | 1/3/23 |
| Walking device, cane/quad cane/walker, n | 6/1/0 |
| AFO/orthotic shoe, n | 6/1 |
| LACI: lacunar infarcts; PACI: partial anterior circulation infarcts; TACI: total anterior circulation infarcts; POCI: posterior circulation infarcts; UCO: Utrechts Communicatie Onderzoek; FAC: functional ambulation categories; LCT: letter cancellation task, having 2 omissions or more on 1 side compared with the other side; AFO: ankle-foot orthotics; SD: standard deviation. |
| Table II. 6MWT outcome (n = 27) |
| Variable | Mean (SD) | Range |
| GPS 1st measurement, m | 408 (132) | 133–700 |
| GPS 2nd measurement, m | 417 (139) | 127–695 |
| MW 1st measurement, m | 413 (127) | 129–664 |
| MW 2nd measurement, m | 422 (132) | 125–668 |
| 6MWT: six-minute walk test; GPS: global positioning system; MW: measuring wheel; SD: standard deviation. |
Reproducibility
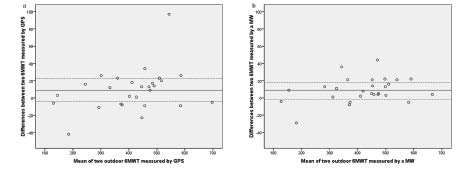
Table III shows the test-retest reliability, agreement and responsiveness of the 6MWTs using GPS or MW. Assessment of the test-retest reliability between the first and second 6MWTs yielded ICCagreement scores of 0.96 and 0.98, respectively. The SEMagreement for GPS was found to be 18.1 metres, compared with 11.9 metres for MW. The Bland & Altman plots (Fig. 1) showed mean differences between the 6MWTs to be above zero (d = 9 m), with limits of agreement ranging from –4.7 to 22.7 metres when using GPS (Fig. 1a), and from –0.8 to 18.8 m when using the MW (Fig. 1b). The SRD was 50.2 m for GPS and 33.0 m for the MW.
| Table III. Test-retest reliability, agreement and responsiveness (n = 27) |
| Variable | ICC (95% CI) | SEM | SRD | p |
| GPS 6MWT 1st vs GPS 6MWT 2nd | 0.96 (0.96–0.98) | 18.1 | 50.2 | 0.06 |
| MW 6MWT 1st vs MW 6MWT 2nd | 0.98 (0.98–1.00) | 11.9 | 33.0 | 0.00 |
| GPS: global positioning system; MW: measuring wheel; 6MWT: six-minute walk test; ICC: intraclass correlation coefficient for agreement; CI: confidence interval; SEM: standard error of measurement; SRD: smallest real difference. |
Fig. 1. (a) 1st six-minute walk test (6MWT) vs 2nd 6MWT measured by global positioning system (GPS). (b) 1st 6MWT vs 2nd 6MWT measured by measuring wheel (MW).
Concurrent validity
Visual inspection of histograms of the 6MWTs showed normal distributions. Pearson’s correlation coefficient for the first 6MWTs using GPS vs the first 6MWTs using MW was 0.98 (p < 0.00), while the second 6MWT using GPS vs MW yielded an r = 0.99 (p < 0.00).
DISCUSSION
The present study showed that conducting the 6MWT over a predefined course selected with Google Earth, while using GPS or a measuring wheel (MW) to determine the distance walked, is a feasible, highly reproducible and responsive method to assess walking endurance in stroke patients’ own neighbourhood. We also found a strong association between the values of the 6MWT protocol measured by GPS and MW during the outdoor 6MWTs. Re-testing yielded a non-significant 9-m increment in walking distance (on top of a total of over 400 m) when using the GPS and a significant 9-m increment when using the MW. This small increase in both measures may reflect a practice effect (7, 19), but in agreement with a previous study by Salbach et al. (16), the mean differences between the two consecutive 6MWTs were close to zero, suggesting that this learning effect is almost negligible. The fact that the 9-m increment found in the second 6MWT using the MW was significant can be explained by the smaller measurement error and higher responsiveness of the MW when compared with the GPS.
Based on found measurement error on the 6MWT indoors, Fulk et al. (5) described a minimum clinically important difference of 54.1 m. This value is higher than the SRDs calculated in the present study, which were 33.0 m for the MW and 50.2 m for the GPS system, respectively. This finding suggests that outdoor testing can be performed within the accepted limits of error for a 6MWT and that the method is able to measure a meaningful effect for individuals participating in community-based rehabilitation programmes.
Despite the higher responsiveness of the hand-driven MW compared with GPS in the present study, all assessors preferred the GPS to the MW because of its smaller size and the fact that it allowed the therapists to keep their own hands free by attaching the GPS device to the patient’s belt or their own.
Conducting the 6MWT outdoors is subject to some limitations. First, weather conditions have to be dry and calm. In addition, the assessors had to select outdoor walking courses that appeared on Google Earth to be smooth and horizontal, without crossing roads. Finally, 4 patients refused to participate in an outdoor test, as they stated that they would feel embarrassed if they met their neighbours.
The present study had some limitations. First, we selected a relatively small sample of our stroke patients who had been discharged home, so our findings may not be generalizable to people with stroke who do not meet the eligibility criteria for this study. Secondly, the MW is more accurate than the GPS used in the study. However, more accurate types of GPS are now available, and future improvements in the satellite system will be accompanied by further improvements in the accuracy of location and time. Thirdly, we used a conservative approach in testing the reliability and responsiveness of the GPS or MW system, by selecting 4 independent assessors and using a random model to calculate ICCs. This suggests that our results may be an underestimation. In addition, it should be taken into account that the time between the two consecutive measurements was relatively short.
In conclusion, the present study has yielded useful data on the reproducibility and validity of conducting the 6MWT in patients’ own home environments using GPS. In our opinion these results are generalizable to other settings, acknowledging that the GPS (like other navigator systems) is robust amongst tall buildings and in changing environments.
The main finding is that conducting the 6MWT in the patients’ own neighbourhood is highly reproducible and responsive. Outdoor 6MWTs, using either GPS or MW, can be recommended for stroke patients to evaluate their walking endurance in their own neighbourhood.
ACKNOWLEDGMENTS
This study is part of the FIT-Stroke trial, which is supported by ZonMw (grant number 80-82310-98-08303). The authors would like to thank the participants for their willingness to participate and Hanneke Roelse, Lenneke van Kats, Anouk van Weerdenburg and Maaike Brienne for their contributions to the present study.
REFERENCES