Alessandro Picelli, MD1, Paola Bonetti, MD1, Carla Fontana, MD1, Martina Barausse, MD1, Francesca Dambruoso, MD1, Francesca Gajofatto, MD1, Stefano Tamburin, PhD2, Paolo Girardi, MSc3, Raffaele Gimigliano, MD4 and Nicola Smania, MD1,5
From the 1Neuromotor and Cognitive Rehabilitation Research Centre, Department of Neurological, Neuropsychological, Morphological and Movement Sciences, University of Verona, 2Neurology Section, Department of Neurological, Neuropsychological, Morphological and Movement Sciences, 3Unit of Epidemiology and Medical Statistics, Department of Public Health and Community Medicine, University of Verona, Verona, 4Second University of Naples, Naples and 5Neurological Rehabilitation Unit, Azienda Ospedaliera-Universitaria Integrata, Verona, Italy
OBJECTIVE: To investigate the accuracy of manual needle placement and electrical stimulation guidance, compared using ultrasonography, for injection of botulinum toxin type A into the gastrocnemius muscle of adults with spastic equinus.
DESIGN: Prospective clinical study.
SUBJECTS: A total of 81 adults with stroke who were scheduled to receive botulinum toxin type A injection into the gastrocnemius muscle.
METHODS: After randomization into two groups, each patient was injected into two sites at each head of the gastrocnemius muscle. The manual needle placement group (n = 42) underwent injections using anatomical landmarks and palpation. The electrical stimulation guidance group (n = 39) underwent injections under electrical stimulation guidance. The accuracy of needle placement and muscle thickness at each injection site were compared by means of ultrasonography.
RESULTS: The overall accuracy of manual needle placement and electrical stimulation guidance, measured using ultrasonography, was significantly higher for the gastrocnemius medialis than for the lateralis (92.0% vs 79.0%). The gastrocnemius medialis was significantly thicker than the lateralis (mean 13.25 mm (standard deviation (SD) 1.86 mm) vs 10.84 mm (SD 1.52 mm).
CONCLUSION: Electrical stimulation guidance may be useful for injections into the gastrocnemius lateralis of adults with spastic equinus. However, neither manual needle placement nor electrical stimulation guidance showed complete accuracy, when measured using ultrasonography.
Key words: rehabilitation; spasticity; botulinum toxin; injection guidance; gastrocnemius; stroke.
J Rehabil Med 2012; 00: 00–00
Correspondence address: Nicola Smania, Neuromotor and Cognitive Rehabilitation Research Centre, Department of Neurological, Neuropsychological, Morphological and Movement Sciences, University of Verona, Italy. P.le L.A. Scuro, 10. IT-37134 Verona, Italy. E-mail: nicola.smania@univr.it
Submitted October 13, 2011; accepted January 17, 2012
INTRODUCTION
Accurate injection is a fundamental prerequisite for the effective and safe treatment of focal spasticity with botulinum toxin type A (BoNT-A) (1, 2). In patients with spastic equinus, the accuracy of needle placement into the gastrocnemius muscle (GM) has been reported to improve the effectiveness of BoNT-A selective neuromuscular blocking (3–6).
Manual needle placement (MNP) is commonly used to inject BoNT-A into the GM (7), while injections under electrical stimulation guidance (ES) or ultrasonography (US) are recommended for deep-seated or small muscles (2). However, a study involving children with cerebral palsy has shown that the accuracy of MNP for GM is 78.7%, with an acceptable accuracy only for the gastrocnemius medialis (GMM) compared with the gastrocnemius lateralis (GML) (7).
The European consensus table on the use of BoNT-A in adult spasticity (2), emphasized the need for studies aimed at clarifying the most suitable techniques to inject BoNT-A. To date, no study has compared the accuracy of MNP, ES and US for BoNT-A injection in adults with focal spasticity.
The aim of this study was to investigate the accuracy of MNP and ES, measured using US, for BoNT-A injection into the GM of adults with spastic equinus after stroke.
METHODS
The study was performed in the Neurorehabilitation Unit of the University Hospital of Verona, Italy. Inclusion criteria were: age >18 years, spastic equinus after ischaemic or hemorrhagic stroke, GM spasticity graded at least 1+ on the modified Ashworth scale (8), time from stroke at least 6 months and time from last BoNT-A injection at least 4 months. Exclusion criteria were: fixed contractures or bony deformities of the affected leg, any previous treatment of the affected leg spasticity with neurolytic or surgical procedures, other neurological or orthopaedic conditions involving the affected leg. All participants gave informed consent for participation in the study, which was carried out according to the Declaration of Helsinki and was approved by the local ethics committee.
Before being injected with BoNT-A, participants were divided into two groups (MNP and ES) according to a simple, software-generated, randomization scheme (www.randomization.cim). In all patients, GMM and GML were determined using MNP (namely, anatomical landmarks and palpation) and BoNT-A was injected into two sites of GMM and GML: a proximal site (near to the muscle origin) and a distal site (at the mid-belly of the muscle bulk) (3). In patients assigned to the ES group, after MNP, electrical stimulation (1 Hz twitch, intensity adjusted to elicit visible contraction) was performed with a portable, battery-powered, stimulator (ES300, Life-Tech Inc., Stafford, TX, USA) in order further to guide needle positioning. A clinician board with more than 3 years of clinical experience in the treatment of spasticity performed the BoNT-A injections.
The accuracy of needle positioning with MNP and ES was compared by measuring positioning by means of US. A physician with more than 4 years of experience in muscular sonography performed B-mode, real time US, using the Logiq® Book XP system (GE Healthcare; Chalfont St Giles, UK) interfaced with a linear transducer (scanning frequency 8 MHz) to confirm the needle placement into the targeted muscle and measure muscle thickness (distance from the superficial to the deep aponeurosis) at each injection site (7). The transducer was positioned in the transverse view, perpendicular to the GM surface and placed gently on the skin using water-soluble transmission gel to avoid any pressure-induced alteration (7). If the needle was not placed into the targeted muscle (i.e. into the soleus muscle or into the subcutaneous tissue), it was repositioned with US into the GM before injecting BoNT-A. All patients remained in the prone position with their affected leg outstretched during the whole procedure.
The Fisher’s exact test and the Student’s t-test were used to assess the effect of age (< 60 vs > 60 years), sex (male vs female), time from onset (< 2 vs > 2 years), muscle (GMM vs GML) and site (proximal vs distal) on the accuracy of needle placement (accurate vs inaccurate) and muscle thickness. Multivariate logistic model was used to compute adjusted odds ratios and 95% confidence intervals (95% CI) to investigate the effects of injection technique (MNP vs ES), muscle, site, age, sex and time from onset on the accuracy of needle placement (coded as 1 = accurate and 0 = inaccurate). The significance level was p < 0.05. Statistical analysis was carried out using R 2.9.2 for Windows.
RESULTS
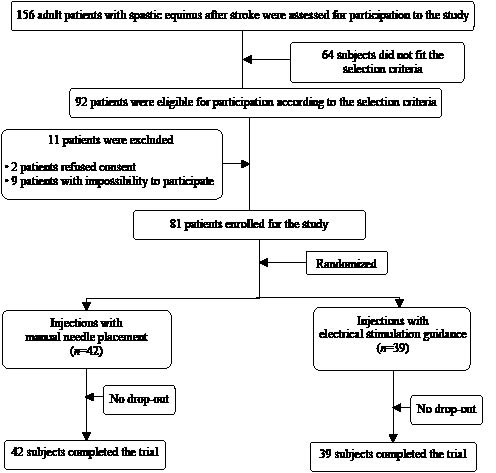
Eighty-one adults (52 males, 29 females; mean age: 59.2 years (standard deviation (SD) 15.2) with spastic equinus after stroke (mean time from stroke: 5.2 years (SD 2.8) were recruited from among 156 outpatients consecutively admitted to our neurorehabilitation unit during the period April 2010–July 2011. A total of 42 patients were assigned to the MNP group and 39 to the ES group. In total, 324 needle insertions into the GM (168 with MNP and 156 with ES) were evaluated (Fig. 1).
Fig. 1. Flow diagram of the study.
The accuracy of MNP and ES, compared using US, was significantly higher for the GMM than the GML (92.0% vs 79.0%, p < 0.001). The GMM was significantly thicker than the GML (13.25 mm (SD 1.86) vs 10.84 mm (SD 1.52), p < 0.001). The effects of age, sex and time from stroke on the overall accuracy of needle placement and muscle thickness are shown in Table I.
| Table I. Effect of age, sex and time from onset on the overall accuracy of needle placement and muscle thickness |
| Parameter | Gastrocnemius medialis (n = 162) | | Gastrocnemius lateralis (n = 162) |
| Proximal site (n = 81) | Distal site (n = 81) | | Proximal site (n = 81) | Distal site (n = 81) |
| Accuracy % | Thickness, mm Mean (SD) | Accuracy % | Thickness, mm Mean (SD) | | Accuracy % | Thickness, mm Mean (SD) | Accuracy % | Thickness, mm Mean (SD) |
| Age, years | | | | | | | | | |
| < 60 (n = 33) | 97.0 | 13.01 (1.53) | 93.9 | 12.71 (1.54) | | 81.8 | 10.59 (1.21) | 78.8 | 10.37 (1.69) |
| > 60 (n = 48) | 87.5 | 13.68 (2.01) | 87.5 | 13.38 (2.02) | | 83.3 | 11.20 (1.66) | 72.9 | 11.00 (1.19) |
| Sex | | | | | | | | | |
| Male (n = 52) | 90.4 | 13.26 (1.95) | 90.4 | 12.98 (1.95) | | 80.8 | 10.84 (1.66) | 75.0 | 10.66 (1.67) |
| Female (n = 29) | 100 | 13.64 (1.68) | 89.7 | 13.33 (1.69) | | 86.2 | 11.14 (1.21) | 75.9 | 10.89 (1.24) |
| Time from onset, years | | | | | | | | | |
| < 2 (n = 14) | 100 | 14.39 (1.64)* | 100 | 14.14 (1.61)* | | 78.6 | 11.50 (1.44) | 50.0* | 11.33 (1.83) |
| > 2 (n = 67) | 92.5 | 13.20 (1.84)* | 88.1 | 12.89 (1.85)* | | 83.6 | 10.83 (1.76) | 80.6* | 10.62 (1.45) |
| *Statistically significant (p < 0.05). |
The accuracy of needle placement into the proximal site of GMM was 88.09% for MNP and 92.30% for ES (p = 0.793), while into the distal site was 92.86% for MNP and 94.87% for ES (p = 0.932). The accuracy of needle placement into the proximal site of GML was 64.28% for MNP and 87.17% for ES (p = 0.033), while into the distal site was 73.80% for MNP and 92.30% for ES (p = 0.057). The multivariate logistic model of covariates influencing the accuracy of needle placement is reported in Table II.
| Table II. Multivariate logistic model of covariates influencing the accuracy of needle placement |
| Parameter | OR | [95% CI] | p-value |
| MNP vs ES guidance | 0.33 | [0.16–0.67] | 0.002 |
| Gastrocnemius medialis vs lateralis | 3.22 | [1.60–6.48] | 0.001 |
| Injection site: Proximal vs distal | 0.61 | [0.32–1.18] | 0.141 |
| Age, < 60 vs > 60 years | 1.59 | [0.80–3.13] | 0.184 |
| Sex, male vs female | 0.75 | [0.34–1.69] | 0.491 |
| Time from stroke, < 2 vs > 2 years | 0.63 | [0.31–1.27] | 0.196 |
| Accurate injection coded as 1; inaccurate injection coded as 0. OR: odds ratio; CI: confidence interval; MNP: manual needle placement; ES: electrical stimulation. |
DISCUSSION
The aim of this study was to investigate the accuracy of MNP and ES, as measured with US, for BoNT-A injection into the GM of adults with spastic equinus. Together, MNP and ES showed an overall accuracy of 92.0% for needle placement into the GMM and 79.0% for needle placement into the GML. In particular, MNP was significantly less accurate than ES for BoNT-A injection into the proximal site of GML (64.28% vs 87.17%).
The accuracy of needle placement into the targeted muscle is a key element in the treatment of focal spasticity with BoNT-A (1–7). Manual needle placement is the injection technique commonly used in large and superficial muscles, such as the GM (2, 7). Data from children with cerebral palsy indicate that the accuracy of GM injections with MNP is approximately 75%, with GMM (92.6%) showing higher figures compared with GML (64.7%) (5, 7). Consistent with these findings, we observed that MNP is more accurate for the GMM vs GML (approximately 90% vs 79%) in adults. Accuracy of needle placement was very high in both the GMM (approximately 93%) and the GML (approximately 90%) in adult patients when guided by ES.
We observed that needle placement into the GM of adults with spastic equinus is not completely accurate when guided by palpation or ES. When GM is injected, the needle can be positioned accurately (i.e. into the muscle mass) or inaccurately (i.e. into the soleus muscle or into the subcutaneous tissue). In our view, ES appeared to be more accurate than MNP because of the exclusion of subcutaneous injections (i.e. non-contractile tissue). However, ES could not result in completely precise injections into the GM of adults, probably because it is “blind” (as well as MNP) to the muscle volume and, consequently, not able to completely exclude injections into the soleus.
The major limitation of this study is the small sample size. The population size may have hindered evaluation of differences in accuracy between MNP and ES in injection sites other than the proximal GML (i.e. a difference close to significance was observed for the distal GML for MNP vs ES comparison). Moreover, our patients were not homogeneous as to the time from stroke (14 patients < 2 years vs 67 patients > 2 years) and this may have hindered evaluation of the effects of disease duration on muscle thickness and the accuracy of needle placement, also considering that in chronic patients the muscle tissue may become less discernible with US due to the development of fibrosis. Furthermore, we did not evaluate the thickness of subcutaneous tissue as well as the clinical effects of BoNT-A injection performed with different techniques (MNP, ES and US). To further validate our findings, future studies should involve a larger population and compare the effectiveness of BoNT-A injection with MNP, ES and US. Future studies on adults should also explore the accuracy of BoNT-A injection into other muscles (e.g. forearm muscles), which contribute to spasticity.
In conclusion, in adults with spastic equinus, ES may be useful for BoNT-A injections into the GML (especially for proximal injections). However, neither MNP nor ES showed full accuracy when measured using US. In contrast, US allows completely accurate injections by precisely evaluating needle position and muscle thickness, and provides increasing opportunities for training (e.g. e-learning) in sono-anatomy for physicians not familiar with the technique.
REFERENCES