OBJECTIVE: To determine whether isometric exercise increases collateral flow in remote ischaemic myocardium in acute coronary occlusion models of patients with coronary artery disease.
DESIGN: A randomized controlled study.
SUBJECTS: Sixty-five patients with 1-vessel coronary artery disease.
METHODS: Subjects were randomly assigned to either the isometric exercise group or non-exercise group. Patients in the exercise group performed isometric handgrip exercises (50% maximal voluntary contraction) during 1 min coronary balloon occlusion, while patients in the non-exercise group remained sedentary. The collateral flow index, heart rate, systolic blood pressure and diastolic blood pressure were determined prior to and following 1 min of coronary occlusion.
RESULTS: In the exercise group, difference values for collateral flow index (after coronary occlusion – before coronary occlusion) were significantly higher than those in the non-exercise group (0.04 standard deviation (SD) 0.05 vs 0.01 (SD 0.03), p < 0.01). Differences in heart rate, systolic blood pressure and diastolic blood pressure were also significantly higher than controls (heart rate 7.84 (SD 8.20) vs 0.88 (SD 3.96), p<0.01; systolic blood pressure: 3.25 (SD 7.17) vs –1.88 (SD 6.21), p < 0.01; diastolic blood pressure 5.88 (SD 6.40) vs –1.5 (SD 6.22), p < 0.01).
CONCLUSION: Isometric exercise in patients with coronary artery disease induced an increase in coronary collateral flow during acute vessel occlusion, which was significantly different from control occlusion.
Key words: isometric exercise; coronary occlusion; myocardial ischaemia; collateral circulation.
J Rehabil Med 2012; 00: 00–00
Correspondence address: Jianan Li, Department of Rehabilitation Medicine, The First Affiliated Hospital of Nanjing Medical University, 300 Guangzhou Road, Nanjing 210029, China. E-mail: lijianan@public1.ptt.js.cn
Submitted August 25, 2011; accepted January 31, 2012
Introduction
Coronary artery disease (CAD) remains a major cause of morbidity and mortality throughout the world. Human coronary collateral vessels and their growth following cardiac events have been studied for years. Animal research has shown that controlled levels of myocardial ischaemia may facilitate coronary collateral formation (1–3). Clinical studies have determined that pre-infarct angina can reduce infarct size (4) and decrease resultant mortality rates. A previous study by our group concluded that exercise-induced intermittent myocardial ischaemia can promote collateral formation in a swine model (5). However, exercise or other factors that directly induce local myocardial ischaemia can cause excessive ischaemia, leading to unintended myocardial damage. Therefore, it is necessary to investigate potential methods for facilitating myocardial collateral recruitment in humans, while minimizing the risk of potentially harmful ischaemia.
Andreka et al. (6) showed that 5-min cycles of ischaemia, followed by 5 min of reperfusion of the hindlimb, repeated 4 times, could reduce myocardial infarct size in pigs. A study by our group showed that ischaemic electrical stimulation of normal limbs can facilitate collateral formation in remote ischaemic limbs and myocardium of rabbits (7). However, all these studies were performed in animals, and the mechanisms of action in humans remain unclear, in particular the effect of remote muscle ischaemia on myocardial collateral formation.
Isometric exercise (IE) is a common daily activity, including tasks such as carrying groceries and performing daily chores. IE is defined as a sustained muscle contraction against an immovable load or resistance, with no change in length of the involved muscle group or joint motion. For many years, IE has been considered a contraindicated type of exercise for patients undergoing cardiac rehabilitation, since it is felt that IE could cause a disproportionate rise in blood pressure and produce high afterload within the left ventricle, leading to an increased risk of myocardial damage (8). However, studies have shown that, compared with maximal aerobic exercise, the rate-pressure product is lower during maximal isometric exercise (9). Therefore, IE may be a safe exercise alternative for individuals with CAD.
IE can induce local ischaemia in the contractile muscle of a normal limb due to a rise in intramuscular pressure. Studies have shown that, during IE, blood flow is partially occluded, with contractile strengths of as little as 20–25% of maximal voluntary contraction (MVC). As the intensity of muscle contraction increases, intramuscular pressure increases and blood flow eventually becomes completely occluded, usually occurring at or above 40–50% MVC (10).
The primary objective of the present study was to observe whether IE induces local ischaemia in the normal limb, which can increase collateral flow in remote myocardial areas of patients with CAD.
Methods
Patients
Sixty-five patients undergoing percutaneous coronary intervention (PCI) were included in the study, based on the following criteria: (i) < 75 years and > 18 years old (mean age 60.2 (standard deviation (SD) 10.1)); (ii), single vessel lesions (> 50% diameter); (iii), absence of unstable angina pectoris, acute or previous Q-wave myocardial infarction, chronic total coronary occlusion, and/or peripheral vascular disease; (iv) written informed consent to participate in the study received prior to the start of any invasive procedures.
Subjects were randomly assigned to either the IE group or the non-exercise group (NG). The study was approved by the ethics committee of the First Affiliated Hospital of Nanjing Medical University, China.
Assessment of haemodynamic parameters and coronary collateral assessment
Diagnostic coronary angiography was performed using the right radial artery approach with a 6-Fr Judkins catheter (Cordis Corporation, USA) for both the left and right coronary arteries. For PCI, 6-Fr guiding catheters were used. Coronary occlusive (i.e. wedge) pressure measurements (Poccl, mmHg) were performed using pressure wires (Smartwire II, Volcano Corporation ComboMap, USA). Central venous pressure (CVP, mmHg) and pulmonary capillary wedge pressure (PCWP) were assessed using a Swan-Ganz catheter (Edwards Lifesciences LLC, USA) inserted into the right femoral vein. Mean aortic pressure (Pao, mmHg), electrocardiography (ECG) and blood pressure were monitored using equilibrium point control (Lead 2000, JJEC, Sichuan, China). Measurements were performed before and after 1-min occlusion.
Coronary pressure-derived collateral flow index (CFI) was determined using simultaneously obtained mean coronary perfusion pressure during vessel occlusion (Poccl), mean aortic perfusion pressure (Pao) and CVP, using the following formula: CFI = (Poccl–CVP)/(Pao–CVP).
Study protocol
Left heart catheterization was performed in each patient, including biplane left ventricular angiography and coronary angiography for diagnostic purposes. Coronary artery stenosis was assessed quantitatively as percentage diameter reduction using the guiding catheter for calibration. Following diagnostic examinations, an intracoronary bolus of adenosine (15–40 μg: left coronary artery and 10–30 μg: right coronary artery) was given for maintenance of epicardial coronary artery calibres. Following coronary angiography, the patients were randomly divided into two groups: IE and NG. All patients were examined for supine maximal voluntary contraction force using a hydraulic hand dynamometer (BASELINE, Fabrication Enterprises Inc., New York, NY, USA). The patients in the IE group then performed a 1-min isometric handgrip exercise (at approximately 50% of maximum contraction force) while undergoing a 1-minute balloon occlusion. The patients in the SC group remained at rest while undergoing the 1-min balloon occlusion. Patients were instructed to avoid performing the Valsalva manoeuvre, in order to maintain stable filling pressures. Data were analysed before and after each balloon occlusion in order to account for collateral recruitment during occlusions. Coronary occlusions were performed at the site of stenosis as a portion of the planned PCI. After occlusion, all the patients received PCI.
Statistical analyses
All continuous data are presented as means (SDs). Intra-individual comparisons of CFI and haemodynamic data between baseline and end of occlusion were assessed using a paired Student’s t-test. An unpaired Student’s t-test was used for comparison of difference values of haemodynamic data and CFI data (data at the end of occlusion-data at baseline) between the two groups. Patient characteristics and clinical state between the two groups were assessed using χ2/Fisher’s exact tests. p < 0.05 was considered statistically significant, with all statistical analyses performed using SPSS 10.0.
Results
Patient characteristics and clinical data
A total of 33 patients were included in the IE group (18 males, 15 females) and 32 in the NG group (15 males, 17 females). No statistically significant differences were found for age, percentage diameter stenosis and maximum voluntary contraction force between the two groups. Patient characteristics, including risk factors and the distribution of target vascular stenosis, in the two groups are shown in Table I.
|
Table I. Patient characteristics and clinical data
|
|
|
IE (n = 33)
|
NG (n = 32)
|
|
Age, years, mean (SD)
|
59.24 (11.30)
|
61.50 (8.74)
|
|
Risk factor, n
|
|
|
|
Obesity
|
14
|
13
|
|
Hypertension
|
30
|
22
|
|
Hypercholesterolaemia
|
24
|
26
|
|
Diabetes
|
24
|
3
|
|
Stenosis undergoing PTCA
(LAD/LCX/RCA), n
|
26/1/6
|
25/5/2
|
|
Percentage diameter stenosis, mean (SD)
|
80.76 (9.11)
|
77.1 (7.03)
|
|
Maximum voluntary contraction force, kg, mean (SD)
|
35.01 (7.36)
|
25.92 (4.52)
|
|
IE: isometric exercise group; NG: non-exercise group; PTCA: percutaneous transluminal coronary angioplasty; LAD: left anterior descending artery; LCX: left circumflex artery; RCA: right coronary artery.
|
Haemodynamic parameters
In the IE group, heart rate (HR), systolic blood pressure (SBP), diastolic blood pressure (DBP), and PCWP after occlusion were increased significantly compared with before occlusion. In the NG group, HR, SBP, DBP and PCWP values at the end of occlusion were not different from those prior to occlusion. Difference values of HR, SBP, DBP and PCWP (ΔHR, ΔSBP, ΔDBP and ΔPCWP = HR, SBP, DBP and PCWP at the end of occlusion – HR, SBP, DBP and PCWP prior to occlusion) in the IE group were significantly higher than values in the NG group (Table II).
|
Table II. Haemodynamic parameters before and after coronary artery occlusion
|
|
|
IE (n = 33)
Mean (SD)
|
NG (n = 32)
Mean (SD)
|
|
HR
|
|
|
|
Baseline
|
82.47 (12.38)
|
79.12 (10.47)
|
|
Occlusion
|
90.31 (13.17)***
|
80.02 (11.95)
|
|
Difference
|
7.84 (8.20)*
|
0.88 (3.96)
|
|
SBP
|
|
|
|
Baseline
|
126.87 (20.98)
|
114.81 (16.05)
|
|
Occlusion
|
130.12 (20.55)**
|
112.87 (14.50)
|
|
Difference
|
3.25 (7.17)*
|
–1.88 (6.21)
|
|
DBP
|
|
|
|
Baseline
|
84.78 (12.96)
|
72.19 (15.58)
|
|
Occlusion
|
90.66 (11.97)***
|
70.65 (14.02)
|
|
Difference
|
5.88 (6.40)*
|
–1.50 (6.22)
|
|
PCWP
|
|
|
|
Baseline
|
21.94 (10.32)
|
17.72 (4.12)
|
|
Occlusion
|
24.88 (10.12)***
|
18.28 (3.99)
|
|
Difference
|
2.94 (2.61)*
|
0.31 (1.02)
|
|
The comparison in the 2 different groups on HR, SBP, DBP and PCWP: *p < 0.01. The comparison in the same group on HR, SBP, DBP and PCWP before and after occlusion: **p < 0.05 ***p < 0.01. ΔHR, ΔSBP, ΔDBP and ΔPCWP = HR, SBP, DBP and PCWP at the end of occlusion – HR, SBP, DBP and PCWP prior to occlusion.
SD: standard deviation; IE: isometric exercise group; NG: non-exercise group; HR: heart rate; SBP: systolic blood pressure; DBP: diastolic blood pressure; PCWP: pulmonary capillary wedge pressure.
|
Changes in collateral flow index
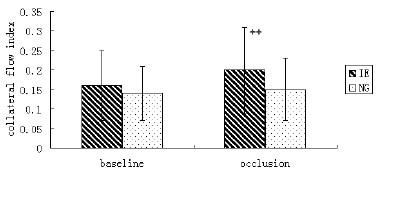
In the IE group, Poccl and CVP values at the end of occlusion were increased significantly compared with prior to occlusion; Pao at the end of occlusion did not differ from before occlusion (p > 0.05). In the NG group, Poccl, CVP and Pao at the end of occlusion were not different from prior to occlusion. Difference values of Poccl (Δ Poccl = Poccl at the end of occlusion – Poccl prior to occlusion) in the IE group were significantly greater than those in the NG group (p < 0.01, Table III, Fig. 1). In the IE group, CFI at the end of occlusion was significantly increased compared with CFI prior to occlusion, but there was no difference in CFI values in the NG group. Difference values of CFI (ΔCFI = CFI at the end of occlusion – CFI prior to occlusion) in the IE group were significantly greater than those in the NG group (p < 0.01, Table III, Fig. 2). There was no significant difference in baseline CFI between the two groups.
|
Table III. Collateral flow index (CFI) between the 2 groups
|
|
|
IE (n = 33)
Mean (SD)
|
NG (n = 32)
Mean (SD)
|
|
Poccl
|
|
|
|
Baseline
|
28.91 (9.81)
|
23.22 (7.91)
|
|
Occlusion
|
33.25 (11.58)***
|
23.81 (8.56)
|
|
Difference
|
4.34 (5.31)*
|
0.59 (2.80)
|
|
Pao
|
|
|
|
Baseline
|
116.01 (16.40)
|
96.19 (13.76)
|
|
Occlusion
|
114.81 (17.26)
|
94.65 (12.72)
|
|
Difference
|
–1.19 (8.59)
|
–1.53 (4.67)
|
|
CVP
|
|
|
|
Baseline
|
12.47 (2.45)
|
10.72 (2.11)
|
|
Occlusion
|
12.69 (2.49)**
|
10.81 (2.15)
|
|
Difference
|
0.22 (0.49)
|
0.09 (0.29)
|
|
CFI
|
|
|
|
Baseline
|
0.16 (0.09)
|
0.14 (0.07)
|
|
Occlusion
|
0.20 (0.11)***
|
0.15 (0.08)
|
|
Difference
|
0.04 (0.05)*
|
0.01 (0.03)
|
|
The comparison the 2 different groups on Poccl and CFI: *p < 0.01. The comparison in the same group on Poccl, Pao, CVP and CFI before and after occlusion: **p < 0.05 ***p < 0.01. ΔPoccl, ΔPao, ΔCVP and ΔCFI = Poccl, Pao, CVP and CFI at the end of occlusion – Poccl, Pao, CVP and CFI prior to occlusion.
IE: isometric exercise group; NG: non-exercise group; Poccl; coronary perfusion pressure during vessel occlusion; Pao: aortic perfusion pressure; CVP: central venous pressure.
|
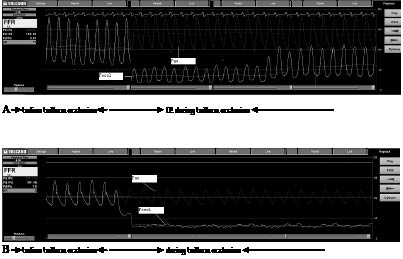
Fig. 1. Changes in Poccl among the two groups during balloon occlusion. (A) Isometric exercise group. When the patient performed isometric handgrip during balloon occlusion, Poccl decreased first, followed by a gradual increase. (B) Non-exercise group. Poccl decreased while the patient remained at rest during balloon occlusion. Pao: mean aortic perfusion pressure; Poccl: mean coronary perfusion pressure during vessel occlusion.
Fig. 2. Collateral flow index (CFI) obtained prior to and at the end of coronary artery balloon occlusion between the isometric exercise group (IE) and the non-exercise group (NG). ++ p < 0.002.
Discussion
Remote heart collateral recruitment due to limb ischaemia in humans has received limited attention. The present study used direct and quantitative assessment of CFI for coronary collateral flow and demonstrated a significant increase in CFI from acutely occluded vessels of patients with chronic CAD during ischaemic handgrip exercise. This effect was more pronounced than collateral flow recruitment due to the effect of vessel occlusion(s) itself.
Isometric exercise in patients with coronary artery disease undergoing rehabilitation
IE can cause an increase in blood pressure and heart rate greater than is observed in more dynamic forms of exercise allowing limb movement (11). The present study showed that, during IE, blood pressure and heart rate were elevated. IE has generally been contraindicated for cardiac patients because of the potential adverse side-effects of increased afterload, which can be induced by higher blood pressure and the possibility of associated ischaemia. However, IE (lifting, squeezing or pressing) frequently occurs during daily activities and is a common form of activity in many routine jobs. Therefore, exclusion of all IE in cardiac rehabilitation programmes could cause cardiac events in patients performing IE in their daily lives who have not been adequately prepared to tolerate these activities. However, studies have shown that during low-intensity IE (40–60% MVC) there are modest elevations in blood pressure, similar to those seen during moderate endurance training (8). An additional study showed that haemodynamic responses to IE (i.e. heart rate, SBP, DBP) were not significantly elevated from those after aerobic exercise (9). Other studies have shown that handgrip or weighted exercise performed alone or in combination with dynamic exercise produce less ischaemic ST-segment depression and arrhythmias than graded exercise testing alone. Therefore, it is possible that IE is a safe and viable exercise alternative during cardiac rehabilitation. It has also been suggested that IE can favour increased myocardial perfusion; however, limited data exist to corroborate this concept (12).
Limb ischaemia induced by isometric handgrip exercises on remote heart collateral recruitment
The coronary collateral circulation is thought to provide supplemental blood supply to the ischaemic regions of the heart. As such, collateral recruitment can preserve myocardial survival during severe stenosis or coronary obstruction, contributing to better residual myocardial contractility and reduced ischaemic symptoms. Therefore, improved collateral circulation could potentially be a new therapeutic target rather than simply a pathological manifestation (13).
Repeated transient myocardial ischaemia can increase collateral blood flow through the formation of collateral circulation. It has also been reported that this type of ischaemia can facilitate collateral circulation formation in animals (1–3, 14–16), without growth in the non-ischaemic condition (17). Clinical studies have shown that pre-infarct angina may reduce infarct size and mortality rate (4, 18). In an earlier study, our group demonstrated that exercise-induced intermittent myocardial ischaemia can promote collateral formation in a swine model (5).
Exercise or other activities that induce local myocardial ischaemia have the risk of causing excessive ischaemia, which can lead to more permanent myocardial damage or cardiac arrest. There is strong interest in identifying methods or activities that can avoid inducing myocardial ischaemia directly as well as facilitate collateral recruitment within the heart. During the past 10 years, studies have shown that brief controlled episodes of intermittent peripheral muscular ischaemia of the arm or leg can confer powerful systemic protection against prolonged ischaemia occurring in a distant organ (19). Andreka et al. (6) showed that 45 minute cycles of ischaemia, followed by 5 min of reperfusion of the hindlimb, can protect against myocardial infarction in the pig. Another study showed that intermittent limb ischaemia occurring during myocardial ischaemia not only reduces MI but also preserves global systolic and diastolic function, thus protecting against arrhythmias during the reperfusion phase (20). We have also shown that ischaemic electrical stimulation of normal limbs can facilitate collateral formation in remote ischaemia limbs of rabbits (7). However, all of these studies have used only animal models, with limited reports on the effects of remote muscle ischaemia on collateral recruitment in the ischaemic myocardium of patients with CAD.
IE can induce ischaemic in the contracting muscle of a normal limb due to an increase in intramuscular pressure. Studies have shown that, during IE, blood flow is partially occluded with contractile strengths as little as 20–25% of MVC. As the intensity of muscle contraction increases above this level, intramuscular pressure increases and blood flow is totally occluded, usually occurring at 40–50% MVC (10). Soller et al. (21) showed that, during exercise at 15% MVC and greater, venous PO2 declined from 40 to 21 Torr (approximately 5.3 to 2.8 kPa). IM PO2 declined from 24 to 8 Torr with 15% MVC, and approached 0 Torr at 30% MVC and 45% MVC. Based on these findings, we asked patients to perform IE at 50% MVC for 1 min to induce limb ischaemia.
Coronary collateral blood flow is quantified objectively using a 0.014 (0.36 mm) intra-coronary wire with a pressure-measuring capability. Collateral flow in an ischaemic area is estimated by calculating CFI during balloon occlusion. A statistically significant improvement in CFI was observed in response to ischaemic isometric handgrip exercises in acutely occluded vessels of patients with CAD. This effect was more pronounced than collateral flow recruitment due to vessel occlusion itself. Since there was no significant difference in baseline CFI and percentage diameter stenosis between the two groups, these results could rule out the effect of the stenosis itself on collateral growth. Therefore, our study demonstrated that ischaemic isometric contraction facilitates collateral flow and perfusion in remote ischaemic heart tissues in patients with CAD. This result challenges prior concepts, which have viewed all forms of isometric contraction as contraindicated in persons with CAD. With this new understanding of how specific IE can influence myocardial collateral flow and perfusion, the judicious use of IE and activity may need to be re-evaluated with respect to its use during the rehabilitation of patients with CAD.
Study limitation
Pressure-derived CFI measurements are not absolute but have a standard error of estimate of 0.08 compared with Doppler-derived CFI measurements (15). In comparison, the mean ΔCFI in the present study is minimal. However, an almost uniformly occurring increase in CFI in response to ischaemic isometric handgrip exercise occurs in patients with CAD.
References