OBJECTIVE: To explore construct(s) (ability, capability, actual performance, and/or perceived difficulty) of activities of daily living measures that have been used in randomized controlled trials.
METHODS: Three databases (Medline, CINAHL, and OTSeeker) were searched. A questionnaire was sent to the author of each eligible study requesting information about the activities of daily living construct(s) that were adopted in his/her study.
RESULTS: A total of 106 studies, which altogether used 17 different activities of daily living measures, were found. Among these, only 12 studies specified in the paper the activities of daily living construct assessed; 7 studies assessed “ability” and 5 assessed “actual performance”. Only 20% of the randomized controlled trials authors reported the mode of administration in the paper. Authors of 34 studies replied to our questionnaire. The most commonly used activities of daily living measures (i.e. the Barthel Index (either the 0–20 or 0–100 scoring version) and the Functional Independence Measure) were employed for assessing various constructs of activities of daily living, with inconsistency between the studies.
CONCLUSION: In stroke randomized controlled trials that measured activities of daily living as an outcome, the measures were used for assessing various construct(s) of activities of daily living (including ability, capability, actual performance, and/or perceived difficulty). This could hamper data interpretation, meta-analysis, and the translation of evidence into clinical practice.
Key words: activities of daily living; stroke; measures; randomized controlled trial.
J Rehabil Med 2012; 00: 00–00
Correspondence address: Ching-Lin Hsieh, School of Occupational Therapy, College of Medicine, National Taiwan University, 4F, No 17, Xuzhou Rd, Taipei 100, Taiwan. E-mail: clhsieh@ntu.edu.tw
Submitted September 2, 2011; accepted March 14, 2012
INTRODUCTION
Stroke is the leading cause of adult disability (1). A person’s performance of activities of daily living (ADL) is considered indicative of the level of concomitant disability (or independence) (2, 3). ADL measures are frequently used as an outcome measure in stroke trials (4, 5). ADL is most commonly used to refer to basic or personal ADL (i.e. self-care activities). However, measuring only basic ADL does not capture the losses in higher levels of physical function or activities that can occur and are necessary for independence in the home and community (i.e. instrumental ADL (IADL)) (6, 7).
It has been proposed that there are 4 distinct constructs of ADL: ability, capability, actual performance, and perceived difficulty (8–11). ADL ability refers to measurement of what a person can do in a standardized, controlled context (11, 12). Capability describes what a person can do in his/her daily environment (8, 13). The main difference between ADL ability and capability is that capability takes into account each individual’s living environmental factors, which might affect a person’s functioning. Both ability and capability are similar in concept to the “activity” of the International Classification of Functioning, Disability and Health (ICF) (14). Actual performance describes what a person actually does do in his/her daily environment (8, 12, 15–17). Perceived difficulty is a report from a person about his/her level of difficulty in performing ADL in daily life (10, 18). Assessment of ability and capability can be useful for identifying problems in performing ADL, and thus can be useful for intervention planning. Actual performance indicates level of dependence/disability in real life (19), and having knowledge of perceived difficulty can help clinicians identify areas of difficulty in ADL performance on the basis of persons’ reports. Because these 4 constructs are distinct, it is important that they are distinguished in both research and clinical practice.
Mode of administration can have a substantial effect on the results of ADL assessments (20, 21). Common modes of administration used in clinical and research settings include observation of performance, participant or proxy-administrated questionnaires, face-to-face interviews, and telephone interviews. Each construct of ADL may be best assessed by a particular mode of administration. For example, ability of ADL is best assessed in a simulated standardized context at a health facility, whereas capability of ADL is best assessed in the real context of a person’s living environment. Therefore, direct observation of patients’ performance is the most appropriate method for assessing ability or capability. Furthermore, actual performance of ADL is known to be best assessed by observation at a person’s living environment in order to determine the client’s real-life performance (22). Performance-based testing in a health facility is not optimal for assessing actual performance, as persons who perform well in a health facility may not be able to achieve the same level of ADL performance in their home (19). Thus, the mode of administration used for ADL measures is relevant to the construct of ADL that are assessed.
Little attention has been paid to the ADL constructs and modes of administration that are used in clinical trials in the field of stroke. Such information, however, is critical for outcome interpretation of clinical trials and analysis in meta-analyses, which is one of the primary tools to facilitate the integration of evidence into clinical practice (23). The primary purpose of this study was to determine the construct of ADL measures that were used in published randomized controlled trials (RCTs) of stroke patients from 2005 to 2009. A second goal was to identify the mode(s) of administration used in these indentified RCTs studies, in order to examine the appropriateness of administration mode(s) for each ADL construct.
METHODS
This study had two parts. The first part was a database search to identify RCTs of stroke patients that had measured ADL as an outcome. This was followed by a survey of the authors of the RCTs to determine which construct and mode of administration were used in their study.
Literature search
In March 2010, 3 databases (Medline, CINAHL, and OTSeeker) were searched with the terms “randomized controlled trial”, “stroke”, and “activities of daily living” and related terms. Searches of these 3 databases were undertaken using the similar search terms described above. The search strategies for Medline and OTSeeker are listed in Appendices I and II, respectively. We searched for all eligible papers that were published between 2005 and 2009. The inclusion criteria were that: (i) RCT participants were persons who had a primary diagnosis of stroke; (ii) the RCT used at least one basic ADL or IADL measure as a primary or a secondary outcome measure; (iii) the full-text paper was published in a peer-reviewed journal; and (iv) the trial was published in English.
Abstracts were screened and the full text of potentially eligible studies was obtained. Data were extracted from the full text of each eligible trial and were rated independently. The data included ADL measure(s)/version used, construct(s) intended to assess, place(s) of assessment, and mode(s) of administration used. These data were commonly described in the methods section of each study. The authors also searched the other sections, if necessary. All these procedures were conducted by one of the authors (Y-CL) and checked by the primary author. Discussion between at least two authors was used to achieve consensus if there was disagreement.
Survey
A questionnaire was developed and e-mailed to the corresponding author of each eligible study. The questionnaire had two parts. The first part was a covering letter containing an invitation to ask RCTs authors to participate, which also included a definition of each ADL construct. The second part asked the authors to report the ADL construct(s) and administrative mode(s) for the ADL measure(s) used in their study. Three reminder e-mails (one per fortnight) were sent to the authors.
Data analysis
Descriptive statistics were used to present the results. Data were analysed with the SPSS 17.0 for Windows Statistical Program. In addition, we examined the location in which the ADL assessments were administered for those studies whose authors replied to our questionnaire. Such information is particularly relevant for assessing constructs of ability and capability, which are best assessed in a standardized context (e.g. a clinical setting) and daily environment (e.g. home), respectively.
RESULTS
Literature search
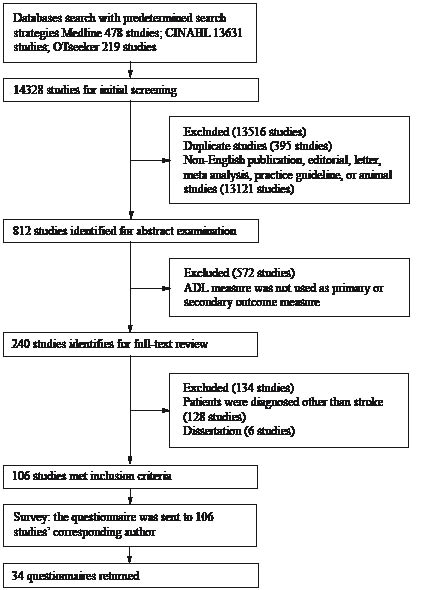
The search of the 3 databases produced 14,328 possible papers. All abstracts and titles were screened using the inclusion criteria. Fig. 1 shows the process and results of the search and screening, which identified 106 papers that met the inclusion criteria. The types of interventions evaluated in the RCTs included 9 studies evaluating pharmaceutical treatment, 84 studies examining rehabilitation therapies, 4 studies evaluating nursing interventions, and 9 studies examining complementary and alternative medicine interventions.
Fig. 1. Process and results of database search, screening and author questionnaires.
Table I lists the ADL measures that were used in the 106 RCTs. Eight measures of basic ADL were used. The Barthel Index (BI) (either the 0–20 or 0–100 scoring version) (24, 25) and 13-item Functional Independence Measure (FIMTM) (26) were the 2 most frequently used basic ADL measures, in 52 and 40 studies, respectively. Six measures of IADL were used. The Nottingham Extended ADL (NEADL) (27) and Frenchay Activities Index (FAI) (28) were the two most commonly used IADL measures; used in 9 and 10 studies, respectively.
| Table I. Number of eligible randomized controlled trials recruited, number of trials with author responses and the activities of daily living (ADL) construct(s) assessed in the trials |
| Measure | Eligible studiesa n | Studies with author responses n | Number of studies assessed the construct/number of study assessed that construct ONLY |
| Ability n | Capability n | Actual performance n | Perceived difficulty n |
| Basic ADL | | | | | | |
| ADL Scale | 1 | 0 | | | | |
| AMAT | 1 | 0 | | | | |
| Augmented BI | 1 | 1 | 1/1 | 0 | 0 | 0 |
| AMPS | 1 | 0 | | | | |
| BI | 52 | 17b | 5/1 | 5/0 | 13/7 | 7/3 |
| MBI | 6 | 5 | 3/1 | 0 | 3/2 | 1/0 |
| FIMTM | 40 | 11 | 10/5 | 3/0 | 5/1 | 4/0 |
| Katz ADL | 1 | 0 | | | | |
| IADL | | | | | | |
| FAI | 10 | 2 | 1/0 | 1/0 | 2/1 | 10 |
| IAM | 2 | 1 | 0 | 0 | 1/1 | 0 |
| Lawton IADL | 2 | 1 | 1/0 | 0 | 1/0 | 0 |
| Katz EADL | 1 | 0 | | | | |
| NEADL | 9 | 2 | 1/1 | 1/ 0 | 1/0 | 0 |
| OARS | 1 | 0 | | | | |
| Both basic ADL and IADL | | | | | | |
| ADL checklist | 1 | 1 | 0 | 0 | 1/1 | 0 |
| EBI (32) | 1 | 0 | | | | |
| KB-ADL | 1 | 0 | | | | |
| aSome studies used multiple ADL measures to assess multiple ADL constructs; thus, the total sum of studies is not 106 studies. bThe original 0–100 scoring BI was used in 9 trials and the 0–20 BI was used in 8 trials. Both versions of the BI are largely the same (e.g. equivalent in content) so we treated them as the same measure here (33). AMAT: Arm Motor Ability Test; BI: Barthel Index; MBI: modified Barthel Index; FIMTM: 13-item Functional Independence Measure; IADL: Instrumental Activities of Daily Living; FAI: Frenchay Activities Index; IAM: Instrumental Activity Measure; Katz EADL: Katz Extended ADL; NEADL: Nottingham Extended ADL; OARS: The Duke Older Americans Resources and Services Procedures; EBI: Extended BI; KB-ADL: Klein Bell ADL Scale. |
Only 12 trials (11.3% of the 106 trials) specified the ADL construct(s) that they had measured in the study. Seven reported that they had assessed ability and 5 reported assessing actual performance. The administrative mode used was reported in 21 trials (19.8% of the 106 trials): 9 used face-to-face interview, 7 used observation, 3 used a patient-administered questionnaire, and 2 used a telephone interview.
Survey
Response rate. Replies were received from 30 of the RCT authors. Four authors had conducted two studies each. Therefore information was provided for 34 (32.1%) of the 106 RCTs. The main characteristics of the 34 trials are listed in Appendix SI (available from: http://www.medicaljournals.se/jrm/content/?doi=10.2340/16501977-1008).
ADL construct(s) employed. Table I reports the ADL construct(s) that were adopted for each measure in the RCTs. Among the 34 trials, the BI and FIMTM were used most frequently, in 17 trials and 11 trials, respectively. Of these 17 trials, 6 used the BI to assess multiple (i.e. 2–4) ADL constructs. Actual performance was assessed by 13 of the 17 trials that used the BI, perceived difficulty by 7 trials, ability by 5 trials and capability by 5 trials. Five out of the 13 trials that used the FIMTM employed it to assess multiple ADL constructs. The FIMTM was used to assess ability only in 5 trials. Furthermore, one of the trials used the FIMTM to assess actual performance only. In addition, the authors of one trial used the modified BI (29) to assess both ability and actual performance.
Altogether, 25 out of 106 trials measured IADL as an outcome. From these 25 trials, 6 trial authors replied the questionnaire and they used 4 different IADL measures (i.e. the FAI used by two trials, the Instrumental Activity Measure (IAM) (30) used by one trial, the Lawton Instrumental Activities of Daily Living (Lawton-IADL) (31) used by one trial, and the NEADL used by two trials). Of these 6 trial authors, 3 reported that they used IADL measures to assess multiple ADL constructs. One of the 6 trial authors reported using the IAM to assess actual IADL performance. One trial used the Lawton-IADL to assess both ability and actual performance. One trial that used the FAI used it to assess all 4 constructs, whereas the other trial that used the FAI used it only to assess actual performance. Two authors reported using the NEADL. One of the trials used it to assess ability only and in the other trial it was used to assess both capability and actual performance.
Mode of administration. Of the 34 trials, more than one mode was used to measure ADL in 15 trials. Face-to-face interviews and observation were the most frequently used modes of administration (Table II).
| Table II. Mode(s) of administration of activities of daily living (ADL) measures used in the trials whose authors replied to the questionnaire |
| Measure | RCTs with author response, n | Mode of administrationa |
| Observation n | Interviewb n | Patient-administered questionnaire n | Proxy-administered questionnaire n |
| Basic ADL | | | | | |
| ADL Scale | 0 | | | | |
| AMAT | 0 | | | | |
| Augmented BI | 1 | 0 | 1/1 | 0 | 0 |
| AMPS | 0 | | | | |
| BI | 17 | 4/1 | 14/6 | 5/1 | 5/1 |
| MBI | 5 | 3/2 | 2/0 | 0 | 2/1 |
| FIM | 11 | 8/4 | 7/1 | 1/0 | 3/0 |
| Katz ADL | 0 | | | | |
| IADL | | | | | |
| FAI | 2 | 1 | 2/1 | 1 | 0 |
| IAM | 1 | 0 | 1/1 | 0 | 0 |
| Lawton IADL | 1 | 1/1 | 0 | 0 | 0 |
| Katz EADL | 0 | | | | |
| NEADL | 2 | 0 | 2/2 | 0 | 0 |
| OARS | 0 | | | | |
| Both basic ADL and IADL | | | | |
| ADL checklist | 1 | 1/1 | 0 | 0 | 0 |
| EBI | 0 | | | | |
| KB-ADL | 0 | | | | |
| aSome studies used multiple modes of administration. The values ‘to the right of the slash’ indicate the number of trials that used that mode of administration ONLY. bOnly 1 study used both face-to-face and telephone interviews for the BI. The others used face-to-face interview. For abbreviations see Table I. |
The two most frequently used basic ADL measures (the BI and the FIM) were administered by all 4 modes of administration. The BI was most frequently (82.4% of the 17 trials) administered as an interview. The FIM was mostly frequently completed by both observation and interview.
The NEADL and the IAM (30) were administered by face-to-face interview only. The Lawton- IADL measure was carried out by observation. The FAI was assessed with multiple modes of administration.
Place of assessment. Of the 34 replied trials, more than half of the assessments (23 trials) were administered in clinical settings. It is noted that 7 trial authors reported assessing capability in clinical settings. Table III shows further details of place and construct of ADL assessment.
| Table III. Place of activities of daily living (ADL) assessment and ADL construct(s) used in the 34 replied studies |
| Construct | Place of ADL assessment administered |
| Clinical setting n | Care home n | Patient’s home n | Patient’s home, hospital, or community service centre n | Unspecified n |
| Ability | 14/6 | 0 | 1/1 | 1/1 | 1/1 |
| Capability | 7/2 | 0 | 0 | 0 | 0 |
| Actual performance | 14/6 | 1/1 | 2/2 | 1/1 | 2/1 |
| Perceived difficulty | 6/0 | 1/1 | 0 | 2/0 | 1/0 |
| aPatients were assessed at several places in the studies. Values are number of studies assessed the construct /number of studies assessed that construct ONLY. It is noted that several studies used ADL measure(s) to assess more than 1 construct. Thus, the summated number of studies is more than 34. Values in italic fonts indicate the mismatched between place to administer the assessment and ADL construct used. |
DISCUSSION
Only 12 of the 106 trials found in this study reported the specific ADL construct(s) used in their studies. Our survey showed that the most commonly used ADL measures (the BI and FIMTM) were employed for assessing one or more of the 4 constructs of ADL. These findings indicate that caution must be taken when directly pooling the ADL outcomes that are reported in the literature into a meta-analysis. The inclusion of data pertaining to different constructs of ADL could provide results that are misleading. It is recommended that authors of clinical trials report the specific construct of ADL that was assessed.
Four distinct constructs of ADL (i.e. ability, capability, actual performance, and perceived difficulty) might be assessed individually or collectively. Each ADL measure, in general, can be used to assess only one construct of ADL. Otherwise, if an ADL measure is used to measure multiple constructs, the data should be reported for each construct. Twelve out of 30 trial authors reported that they used an ADL measure to assess multiple constructs. However, these trial authors reported only one value of assessment in the text, which cannot represent more than one construct of ADL. Thus, the meaning of the data is confusing and hampers interpretation of data. When designing clinical trials, it is recommended that ADL measures be used to assess only one of the ADL constructs. If measures are used to measure more than one construct, trial authors should report values for each construct that is assessed.
All 4 constructs were measured across the RCTs in this study. However, it is not clear if all 4 constructs are appropriate to be used as outcome measures. Capability is defined as ADL performance that is assessed in an individual home environment. As each individual will be assessed in a different home context, with varying task demands and skills requirements, capability scores may not be appropriate for between-person (group) comparisons, which is the typical analysis used in an RCT. Ability represents a person’s performance of standardized ADL tasks in a clinical setting. While such information can be useful for identifying difficulties in performing ADL tasks and for ADL intervention planning, once an individual is discharged to the community, there are many factors that can influence ADL performance, such as motivation and living environment. Thus, ability that is assessed in clinical settings may not necessarily represent level of dependence (disability) in the community. In brief, prospective users have to consider the aforementioned limitations (i.e. capability is not appropriate for between-person (group) comparison and ability does not inevitably reflect independence in the community) when using capability or ability as an indicator of disability or independence.
Perceived-difficulty is a subjective indicator of individual needs. Assessment of perceived difficulty can help clinicians to identify unmet needs in individual persons with stroke and plan intervention toward patient-centred care (34). According to Jette (9), rating of perceived difficulty in performing ADL tasks can be considered the primary indicator of disability, whereas rating of actual performance is an indicator of the consequence of disability. Therefore, only perceived difficulty and actual performance appear to be appropriate as an outcome or disability indicator (9, 15, 18). It is recommended that both perceived difficulty and actual performance should be used as outcome indicators to ensure that the scope of the disability is comprehensively covered.
In general, ADL measures are used not only for outcome measurement, but also for other purposes. For example, researchers often use ADL measures to estimate prevalence of disability and develop a prognosis model (35–37). Clinicians use them to assist with discharge planning, estimate care requirements, and guide treatment planning (22). However, there is still a lack of empirical evidences regarding which ADL constructs are best for each of the aforementioned purpose and future studies that explore this are warranted. We believe that such research would promote the utility of ADL measures for patient management in clinical settings.
Our findings are also important for health professionals who use ADL measures in clinical practice. Clinicians may have to assess several ADL constructs for various purposes and, like trial authors, it is important that they specify which specific construct(s) is being assessed.
The terminology and definition of the constructs of ADL have not been well addressed or unified in the literature. In this study, we used the terminology and definitions that have been used in previous studies (8–11). While the terms, particularly ability, capability, and capacity, are widely used, there are varying published definitions of these terms. As trial authors and users of published trials may interpret the constructs differently, it is recommended that both the terminology and definitions of the constructs of ADL be specified a priori in every study that measures ADL as an outcome.
Nearly 20% of the RCT authors reported the mode of administration in the paper. Three modes (interview, observation, and questionnaire, ranked by frequency of usage, from high to low) were the top 3 commonly used modes in these trials. Some trials used multiple modes of administration for the ADL measure used in the studies. We found that the mode of administration varied substantially for each construct of ADL. This finding and the various uses of ADL construct(s) might be because these RCTs authors had not tried their effort to access and follow the manual of each measure for administration or that they took it for granted in their assessments. In the few studies that have explored the effect of mode of administration on study results, it has been shown that mode of administration may affect the results of ADL assessment (20, 21). For example, self-report by patients may underestimate the level of assistance needed in ADL (20). Thus, it is recommended that trial authors report their ADL administration mode(s). Further studies are needed to determine the most appropriate mode of administration for each construct of ADL.
As aforementioned, the capability construct is best assessed/observed at home or a long-term care institution because of its intention to measure what a person can do in his/her daily environment (8, 13). However, of those who replied, 7 of 8 authors who intended to assess capability administered ADL assessments in clinical settings. Thus, the results of ADL assessments of these 7 studies might be threatened because of an inappropriate place of assessment. Prospective users should select the most appropriate context to assess ADL constructs, particularly for ability and capability, to achieve reliable results.
Every ADL measure has been developed according to a particular philosophy of measurement. For example, the FIM and BI were designed to measure the level of assistance needed for performing ADL tasks (24, 29, 30). Importantly, the manual of the FIMTM specifies that the FIMTM intends to assess a construct of actual performance (38). In addition, the FAI was developed to assess frequency of performing IADL tasks during a specific period (e.g. 3 or 6 months) (28). Thus, clinicians and researchers have to consider whether the measurement philosophy of an ADL measure fits their research purpose to avoid misuse.
The overall response rate to the author questionnaire was low (32.1% of the 106 studies). There were 25 out of 106 studies using IADL measure as an outcome measure. Only 6 author of these trials (24.0% of the 25 studies) replied to our questionnaire. In addition, the 5-year time frame (2005–2009) for searching the RCTs is a limitation. Furthermore, we identified the place of ADL assessment only by reading the full text of the 34 studies for which we received replies. We did not ask RCT authors to report where the ADL assessment was administered in our questionnaire. As a result, place of assessment could not be identified in two studies. Furthermore, our study focused only on RCTs, but not the other types of study (e.g. descriptive studies). These limitations hamper the generalization of the results of this study.
In conclusion, our results showed that the ADL measures were used for assessing various constructs of ADL, which limits data interpretation and hampers future meta-analysis and the integration of research evidence into clinical practice. These findings have important implications for the selection of ADL constructs in both research and clinical settings. We recommend that future studies specify the construct of ADL to measure in order to facilitate further data interpretation and summary of ADL outcomes among clinical trials.
ACKNOWLEDGEMENTS
This study was supported by a research grant from the National Science Council (NSC96-2628-B-002-034-MY3). Ching-Lin Hsieh was partly supported by an Endeavour Research Fellowship with funding provided by the Australian Government. Tammy Hoffmann is supported by a NHMRC/PHCRED Career Development Fellowship with funding provided by the Department of Health and Ageing.
REFERENCES