OBJECTIVE: To determine the effectiveness of music interventions in increasing physical activity in older adults.
METHODS: Searches until March 2011 were conducted through CINAHL, MEDLINE, EMBASE, PubMED, AMED, PsychINFO, AUSPORT, PEDro, OTseeker, Expanded Academic ASAP, SPORTDiscus, and The Cochrane Library. Selection criteria included older adults, music interventions, physical activity outcomes, and quantitative designs. Two reviewers independently screened records. Study details included objectives, designs, participants, music interventions, physical activity outcomes, and results. Risk of bias was assessed using the PEDro scale.
RESULTS: The review included 12 low to moderate quality studies with 309 participants. Three meta-analyses conducted for the review (4 trials and 99 participants) did not demonstrate any within-session differences in comparisons between music and no-music interventions. Two individual trials of moderate quality demonstrated increased capacity to perform physical activity following exercise programs with music over 4 and 8 weeks compared with no-music. There was no evidence that any particular music intervention was superior to another.
CONCLUSION: Evidence from a small number of low to moderate quality trials did not demonstrate within-session improvements for older adults who listen to music during exercise. However, there may be cumulative benefits following programs with music over several weeks.
Key words: systematic review; music; music therapy; motor activity; aged.
J Rehabil Med 2012; 44: 00–00
Correspondence address: I.N Clark, Music Therapy Department, Wantirna Health, 251 Mountain Highway, Wantirna Victoria 3152, Australia. E-mail: Imogen.Clark@easternhealth.org.au
Submitted December 7, 2011; accepted May 29, 2012
INTRODUCTION
Older adults who participate in physical activity involving regular continuous muscle activation experience health benefits with a reduced risk of mortality and morbidities (1–3). Physical activity includes activity with components of duration, frequency or intensity that significantly increases daily energy expenditure (4–7).
The World Health Organization recommends that older adults participate in a minimum of 150 min of moderate-intensity physical activity per week (8). However, older people may experience difficulty in meeting recommended amounts of physical activity (1, 9). To address this difficulty, music has been described as an environment modifier that might motivate older adults to increase participation in physical activity (10).
Reviews examining music and exercise with older adults have focused on specific functional tasks (11,12), such as improved balance (13, 14) and performance of upper limb function (15), rather than whether music improved physical activity levels. In contrast, research with young adults has demonstrated significantly increased physical activity including energy consumption (16–18), distance (19, 20) and endurance (21, 22) during conditions with music compared with no-music. Proposed mechanisms for this improved physical activity in younger adults during conditions with music include diversion of attention, enhanced mood, psychomotor arousal, and cueing of synchronous rhythm (23).
Based on evidence from younger adults, it could be proposed that music interventions may promote increased physical activity in older adults. Therefore, we conducted a systematic review and meta-analyses of the literature that focused on music interventions and older adults’ physical activity. The primary aim of this review was to determine the effectiveness of music interventions in increasing the physical activity levels of older adults.
METHOD
Data sources
A systematic search of the literature was conducted using the following electronic databases from the earliest available date until March 2011: CINAHL, MEDLINE, EMBASE, PubMED, AMED, PsycINFO, AUSPORT, PEDro, OTseeker, Expanded Academic ASAP, SPORTDiscus, and The Cochrane Library. The search strategy involved two key concepts, music interventions (for example, music therapy and auditory stimulation) and physical activity outcomes (for example, physical performance, energy metabolism, and heart rate). Where possible, key words were mapped to subject headings, and limiters for humans and older adults were applied. When databases did not include age limiters (AMED, The Cochrane Library, SPORTDiscus, AUSPORT, Expanded Academic ASAP), a population search for older adults was also conducted using the following terms: Older Adult*, 60 year*, elderly, geriatric, and older person*. (See Appendix I for search strategy example on MEDLINE).
Manual reference checking and citation tracking of the included articles using Google Scholar were undertaken to find any further studies that met the inclusion and exclusion criteria. All references resulting from the search strategy were imported into a bibliographic library (Endnote X4 Thomson Reuters) and duplicates were deleted.
Eligibility criteria
Studies with sample means of 60 years or more were included as representing older adults (24).
To compare various music interventions, no limits were placed on the types of music used with the inclusion of live, recorded commercial, specifically composed, instrumental, and vocal productions. This review required that study results clearly measured the effects of a music intervention on physical activity. Therefore we excluded research with co-interventions where results could not be solely attributed to a music intervention. There were no limitations placed on comparison interventions, which could include, no music, other types of music, or alternative sounds.
Studies were included if they reported data about the frequency or intensity of physical activity over time. Conversely, studies that only included outcome measures for one-off tasks such as functional independence measures were excluded, as these do not provide information related to energy expenditure (25). Further, it was expected that outcome measures for physical activity and energy expenditure would be expressed in units (for example, distance, number of repetitions, and watts per minute). Therefore, only studies with quantitative methods and statistical analysis were included (Table I).
|
Table I. Eligibility criteria
|
|
|
Inclusion
|
Exclusion
|
|
Participants
|
Mean age ≥ 60 years
|
|
|
Music intervention
|
A music intervention is being investigated for its effects on physical activity
|
Results are not exclusively attributable to the effects of a music intervention on outcome measures for physical activity
|
|
Outcome measures
|
Data about the frequency, duration, and/or intensity of the activity being examined
For example:
Mets/Watts per min
Steps over time
Number of repetitions
Distance walked (e.g., 6 min walk test)
Sessional heart rate
Exercise duration
|
Discrete measures of functional capacity for clinical assessment, goal setting, treatment planning or monitoring
For example, not:
Sit to stand
Functional Independence Measures
The Barthel Index
Walk cadence
Walk velocity
Range of motion
|
|
Methodology
|
Quantitative studies with statistical analysis
|
Qualitative studies, program descriptions and case studies
|
|
Publications
|
Peer reviewed journals with full text in English
Higher Degree theses and dissertations
|
Books
Conference abstracts
|
Study selection
Two reviewers (INC and NFT) independently applied the inclusion and exclusion criteria to titles and abstracts generated through database searches. Potentially relevant articles were identified and retrieved in full text for independent assessment by two reviewers (INC and NFT) using the inclusion and exclusion criteria. Reference checking and citation tracking of included articles was undertaken to identify further inclusions.
Assessment of risk of bias
Two reviewers (INC and NFT) independently assessed the risk of bias of the included studies using the PEDro scale and discrepancies were discussed until consensus was achieved. The PEDro scale has demonstrated validity for measuring the risk of bias in clinical trials (26) with high inter-rater reliability for scores in non-pharmacological studies (intra-class correlation coefficient = 0.91; 95% confidence interval (CI) = 0.84–0.95) (27). The scale includes 11 criteria, however as recommended by the scale developers, scores are only attributed to items 2–11 (internal validity) so that a maximum total of 10 points is available. The first item relates to external validity and is omitted from scoring (28). The quality of each study was rated as low (0–4 points), moderate (5–7 points), or high (8–10 points) (29). The methodological quality of studies did not have any bearing on a paper’s inclusion for the review.
Data extraction
A data extraction form was developed to guide the identification of relevant information. One reviewer (INC) extracted data from the included studies, and a second reviewer (FAB) checked for accuracy. If a discrepancy was detected, this was discussed and resolved with reference to the full text of the relevant article. Extracted data included: reference details; study objective(s); study design; subject details (sample size, demographic details, inclusion and exclusion criteria, recruitment, characteristics, and group similarity); music intervention details (live or recorded, specifically composed or commercial, rhythm and tempo, styles, instrumentation and equipment, duration, and frequency); control and comparison interventions; the type of physical activity; outcome measures (physical activity, other outcome measures, and within or between session data collection); results including statistical analysis (pre and post intervention means, standard deviations, and sample sizes); and author conclusions.
Data analysis
Data were analysed according to recommended guidelines (The Cochrane Collaboration, 2008) (30). To compare results across the included studies, effect sizes with 95% CI were calculated for each study as standardized mean differences, Hedges-g bias corrected (g), between the experimental and control conditions. The standardized mean difference is the difference between two group means divided by the pooled standard deviation from both groups. Where studies provided a standard error (SE), this was converted to the standard deviation. If studies did not provide point measures or measures of variability, but included complete raw data, this information was used to calculate the mean and standard deviation (SD). Where studies reported median scores, data were checked for symmetrical distribution and if this was the case then median scores were used directly in calculations. If trials included outcomes adjusted for baseline scores, then we planned to use unadjusted values for calculations.
Meta-analysis, using a random effects model, was planned if two or more studies were considered to be clinically homogenous. Studies were regarded as being clinically homogeneous if they included similar populations, interventions, and outcome measures. A random effects model assumes that effect sizes will vary between the studies and allows for greater uncertainty than a fixed effects model (31). Meta-analyses were performed using Review Manager 5.1 (Version 5.1, The Cochrane Collaboration, Copenhagen, Denmark) and reported as standardized mean differences, delta (δ). The statistical heterogeneity of studies combined in meta-analyses was assessed by calculating I2, which describes the total statistical variation across the studies as a percentage with values of greater than 50% indicating moderate to high statistical heterogeneity (32). When studies could not be combined in meta-analysis due to clinical heterogeneity or when median scores were reported with abnormally distributed data, a narrative format was used to report individual study results.
Syntheses of results were planned to examine if, and if so, how effective music interventions were in improving physical activity compared with no-music, alternative sounds and other music interventions.
RESULTS
Study selection
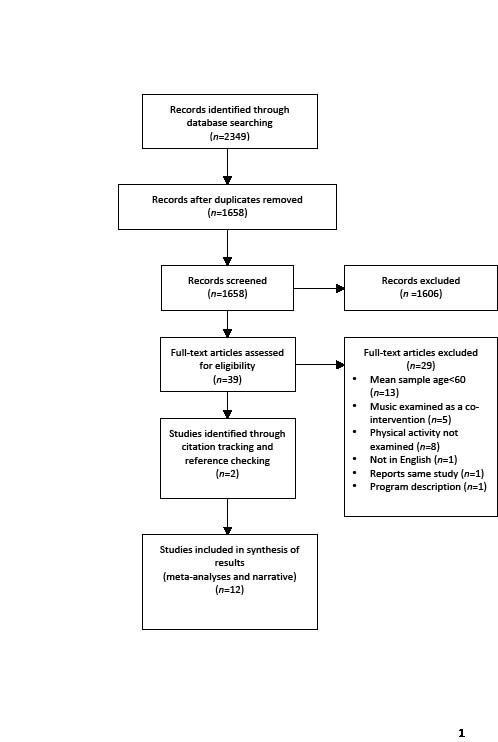
The electronic search yielded 2,349 references, resulting in an initial library of 1,658 records following the removal of 691 duplicates. Independent review of titles and abstracts in the initial library by two reviewers (INC and NFT) resulted in good agreement with exclusion of 1,606 and retention of 39 records (κ = 0.76, SE = 0.05, 95% CI = 0.65 to 0.86). Agreement between two reviewers (INC and FAB) was recorded for 31 of the full text articles, with 7 inclusions and 24 exclusions indicating a moderate level of agreement (κ = 0.51, SE = 0.14, 95% CI = 0.23 to 0.79). The remaining 8 articles were discussed, with a main source of disagreement being in determining if outcome measures met our definition for physical activity. This disagreement was resolved during discussion involving all three reviewers, resulting in 3 further inclusions. Manual reference checking and citation tracking revealed two unpublished theses that met inclusion criteria resulting in a final review library of 12 studies (Fig. 1).
Fig 1. PRISMA Flow diagram: Study selection.
Study characteristics
Samples. The 12 trials included 309 older adults, with samples that ranged from 16 to 45 participants (mean = 26, SD = 9). Participants were recruited from a variety of settings or programs including chronic obstructive pulmonary disease (COPD) rehabilitation programs (n = 5) (33–37), residential care facilities (n = 4) (38–41), community exercise groups (n = 2) (42, 43), and an inpatient rehabilitation program (n = 1) (44). While ten trials provided sample means with a range from 62 to 86 years (33–40, 42, 44), one reported a sample age over 65 years (43) and another described a sample age range of 53 to 94 years (41). Of those trials that provided demographic data (n = 11), 73% of participants were women.
Research designs. The review included 3 randomized controlled trials (33, 34, 44), 4 within subject random crossover designs (35, 36, 38, 39), and 5 within-subject non-random crossover designs (37, 40–43).
Eleven trials compared physical activity during conditions with music and no-music (33–40, 42–44), with two of these also investigating alternative interventions including natural sounds (43) and grey noise (36). One trial compared two music interventions and did not involve conditions with no-music or an alternative intervention (41). Nine trials incorporated recorded commercial music (33–38, 41–43), two examined live music (39, 44), and two investigated specifically composed music (40, 41). Five trials made comparisons between two music conditions including slow tempo and moderate (34) or fast tempo (43), preferred and non-preferred (42), instrumental and vocal (39), and specifically composed and recorded commercial music (41).
All the included trials examined within-session physical activity outcomes and two trials also investigated medium-term training effects of exercise with music over 4 to 8 weeks (33, 34). A variety of physical activities were examined including walking (n = 5), upper body exercise (n = 1), stationary cycling (n = 1), group exercise sessions (n = 4), and individual exercise sessions (n = 1). Physical activity outcome measures included walk distance (33, 35, 37, 43), exercise duration (33, 34, 36, 44), sessional heart rate (35–37, 42, 43), number of exercise repetitions (34, 38, 39–41), and exercise workload (36).
Other outcome measures not classified as physical activity for the purposes of this review included ratings of perceived exertion (35–37, 42), functional respiratory measures (33–37), oxygen saturation (35), range of movement (41), correct exercise performance (41), session attendance (33, 34, 40) and various self-reporting psychosocial scales (33, 34, 37, 41–44) (Table II).
|
Table II. Study characteristics
|
|
Study
|
Design
|
Participants
|
Intervention
|
Activity
|
PA outcomes
|
Other outcomes
|
|
Bauldoff et al., 2002 (33)
|
RCT (2 groups)
|
COPD patients (n = 24)
Age, mean 68.1 (SD 8)
4 male, 20 female
Exp: n = 12; Con: n = 12
|
Exp: Recorded commercial music
Con: No-music
|
Individual home based walking program
|
Between-session 6MWT (baseline, 4 weeks, 8 weeks)
Within-session pedometer and self reported logbook (time & distance)
|
Perceived dyspnea
Anxiety
Depression
QoL
Self reported logbook (sessions)
|
|
Bauldoff et al., 2005 (34)
|
RCT (3 groups)
|
COPD patients (n = 30)
Age, mean 63 (SD 111)
3 male, 17 female
Exp slow: n = 10; Exp fast: n = 10; Con n = 10
|
Exp 1: Slow tempo recorded commercial music
Exp 2: Moderate tempo recorded commercial music
Con: No-music
|
Individual upper body ergometry
|
Between-session 6 Minute peg and ring board test (baseline, 4 weeks)
Within-session self reported logbook (time)
|
Perceived dyspnea
QoL
Self reported logbook (music, breathlessness, fatigue, sessions)
|
|
Bernard, 1992 (38)
|
Within subject random crossover (2 groups)
|
Females in RC (n = 25)
Age, range = 65–99, mean 85.5 (SD 7.67)
|
Exp: Recorded commercial music
Con: No-music
|
Individual exercise sessions
|
Within-session exercise repetitions
|
None
|
|
Davin, 2005 (42)
|
Within subject non-random crossover (3 groups)
|
Females in community exercise (n = 27)
Age, range 63–87, mean 74.6 (SD 6.3)
|
Exp 1: Preferred recorded commercial music
Exp 2: Non-preferred recorded commercial
Con: No-music
|
Group water exercise sessions
|
Within-session average HR measured at 5 minute intervals
|
Feeling states
RPE
|
|
Johnson et al., 2001 (39)
|
Within subject random crossover (3 groups)
|
Individuals in RC (n = 19; Age, range = 65–90, mean 84.3; 4 male, 15 female).
|
Exp 1: Live familiar instrumental music
Exp 2: Live familiar vocal music
Con: No-music
|
Group exercise sessions
|
Within-session exercise repetitions
|
None
|
|
Kendelhardt, 2003 (44)
|
RCT (2 groups)
|
Rehab patients (n = 30)
Exp: n = 15; age, range = 49–88, mean 66.3 (SD 11.9); 4 males, 11 females
Con: n = 15; age, range = 54–72, n = 61.7, (SD 4.5); 5 males, 10 females
|
Exp: Live preferred music
Con: No-music
|
Individual stationary cycling
|
Within-session exercise duration
|
Self perceived pain, anxiety, & rehabilitation
Negative verbalizations
|
|
Lee, 2001 (43)
|
Within subject non-random crossover (single group)
|
Individuals in community exercise program (n = 16) Age over 65 years
|
Exp 1: Fast tempo recorded commercial music
Exp 2: Slow tempo recorded commercial music
Con 1: Nature sounds
Con 2: No-music
|
Individual indoor walking
|
Within-session steps
HR pre and post session
|
Feeling states
|
|
Mathews et al., 2001 (40)
|
Within subject non-random crossover (single group)
|
Individuals in RC with dementia (n = 18)
Age: range 74–97, mean 85
1 male, 17 females
|
Exp: Specifically composed music
Con: No-music
|
Group exercise sessions
|
Within-session exercise repetitions
|
Session attendance
|
|
O’Konski et al., 2010 (41)
|
Within subject non-random crossover (single group)
|
Individuals in RC (n = 45, Age range 53–94
3 males, 42 females
|
Exp 1: Specifically composed music
Exp 2: Recorded commercial music
|
Group exercise sessions
|
Within-session exercise repetitions
|
Self-reported perceptions
Observed exercise adherence
|
|
Table II. Contd
|
|
Study
|
Design
|
Participants
|
Intervention
|
Activity
|
PA outcomes
|
Other outcomes
|
|
Pfister et al., 1998 (35)
|
Within subject random crossover (2 groups)
|
Patients with COPD (n = 19)
Age: range 57–85, mean 71.9 (SD 7.8)
11 males, 8 females
|
Exp: Recorded commercial music
Con: No-music
|
Individual treadmill walking
|
Within-session 6MWT
Within-session HR 30 s intervals
|
RPE
Oxygen saturation
|
|
Thornby et al., 1995 (36)
|
Within subject random crossover (single group)
|
Patients with COPD (n = 36)
Age, range = 45–63, mean 63 (SD 8.8)
11 males, 25 females
|
Exp: Recorded commercial music
Con 1: Grey noise
Con 2: No-music
|
Individual treadmill walking gradual increased workload
|
Within-session maximum HR
Total exercise time
Total exercise workload
|
RPE
|
|
von Leupoldt et al., 2007 (37)
|
Within subject non-random crossover (2 groups)
|
Patients with COPD (n = 20)
Age, mean 65 (SD 10)
12 males, 8 females
|
Exp: Recorded commercial music
Con: No-music
|
Individual indoor walking
|
Post minus pre session HR
Within-session 6MWT
|
Oxygen saturation
Lung function
Perceived unpleasantness
RPE
Affect
|
|
RCT: randomized controlled trial; PA: Physical activity; Exp: experimental group; SD: standard deviation; Con: control group; COPD: chronic obstructive pulmonary disease; 6MWT: 6 min walk test; QoL: quality of life; RC: residential care; HR: heart rate; RPE: ratings of perceived exertion; Rehab: rehabilitation.
|
Risk of bias within studies
A good level of agreement between the two reviewers was recorded for study quality (κ = 0.63, 95% CI = 0.49 to 0.76). Quality of the included trials was rated as low (n = 7) to moderate (n = 5) with scores ranging from 1 to 6 out of a possible 10 points (mean = 3.8, SD = 1.7). The highest quality score of 6 points was achieved by two trials (34, 36). None of the trials concealed group allocation and only one demonstrated baseline similarity between groups (34). None of the trials gained scores for blinding of subjects or therapists administering interventions. Only two trials blinded assessors (36, 41). In addition, two trials did not provide results for all outcome measures (39, 41), and therefore demonstrated possible outcome-reporting bias. (See Appendix II for quality results).
Synthesis of results
Comparisons of music and no-music.
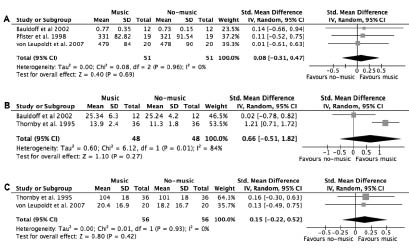
Meta-analysis of 3 trials and 63 participants with COPD comparing conditions with recorded commercial music and no-music did not demonstrate differences for within-session walk distance (33, 35, 37) (δ =0.08, 95% CI = –0.31 to 0.47, I2 = 0%, p = 0.69) (Fig. 2a). Meta-analysis of two trials and 60 participants with COPD comparing conditions with recorded commercial music and no-music did not demonstrate differences for within-session walk time (δ = 0.66, 95% CI = –0.51 to 1.82, I2 = 84%, p = 0.27) (33, 36) (Fig. 2b). Meta-analysis with 2 trials and 56 participants with COPD comparing conditions with recorded commercial music and no-music did not demonstrate differences for within-session heart rate (δ = 0.15, 95% CI = –0.22 to 0.52, I2 = 0%, p = 0.42) (36, 37) (Fig. 2c).
Fig. 2. Meta-analyses comparing within-session physical activity of participants with COPD walking with recorded commercial music (experimental) and no-music (control): (a) distance; (b) time; (c) sessional heart rate.
Other trials comparing music with no-music conditions could not be combined in meta-analyses due to clinical heterogeneity. Two individual trials of moderate quality demonstrated that participants with COPD who listened to recorded commercial music during exercise programs over 4 to 8 weeks improved their endurance for walking (g = 1.58, 95% CI = 0.67 to 2.50, p < 0.01) (33) and upper limb exercise repetitions (slow tempo music, g = 1.27, 95% CI = 0.31 to 2.23, p = 0.01; moderate tempo music, g = 1.87, 95% CI = 0.82 to 2.92, p < 0.01) (34) when compared to exercise over the same period without music (Table III).
An individual trial of moderate quality demonstrated that participants with COPD who listened to recorded commercial music increased their within-session energy consumption (g = 0.70, 95% CI = 0.23 to 1.18, p < 0.01) when compared to sessions without music (36). A further trial of low quality demonstrated that older adults increased their within-session numbers of steps during conditions with no-music compared with slow tempo recorded commercial music (g = –1.19, 95% CI = –1.94 to –0.44, p < 0.01) and fast tempo recorded commercial music (g = –0.91, 95% CI = –1.64 to –0.18, p = 0.01) (43).
Other trials of low to moderate quality comparing conditions with music and no-music did not demonstrate any differences for within-session heart rate (42), numbers of exercise repetitions (38), or exercise time (44). Two final trials of low quality provided inconclusive results with one that reported increased within-sessions exercise repetitions during some specific exercises with music and some with no-music (39), and another reporting results that could not be expressed as a standardized mean difference (40) (Tables III and IV).
|
Table III. Standardized mean differences (95% CI) between recorded commercial music and no-music
|
|
Study
Outcome measure
|
Quality/10
|
Groups: mean (SD)
|
Standardized mean difference
|
Level of significance
|
|
Music
|
No-music
|
Hedges-g (95% CI)
|
p-value
|
|
Between-session results
|
|
|
|
|
|
|
Bauldoff et al., 2002 (33) – Walking
|
5
|
|
|
|
|
|
6MWT, feet
|
|
1,467.5 (363.3)
|
959.8 (245)
|
1.58 (0.67 to 2.50)*
|
p < 0.01
|
|
Bauldoff et al., 2005 (34) – UL exercise
|
6
|
|
|
|
|
|
6MRPB slow music
|
|
174.4 (23.0)
|
144.9 (21.5)
|
1.27 (0.31 to 2.23)*
|
p = 0.01
|
|
6MRPB moderate music
|
|
190.10 (24.7)
|
144.9 (21.5)
|
1.87 (0.82 to 2.92)*
|
p < 0.01
|
|
Within-session results
|
|
|
|
|
|
Bauldoff et al., 2002 (33) – Walking
|
5
|
|
|
|
|
|
Logbook – time
|
|
25.34 (6.30)
|
25.24 (4.20)
|
0.02 (–0.78 to 0.82)
|
p = 0.96
|
|
Logbook – distance, feet
|
|
0.77 (0.35)
|
0.73 (0.15)
|
0.14 (–0.66 to 0.94)
|
p = 0.73
|
|
Logbook – total distance, miles
|
|
19.1 (16.7)
|
15.4 (8.0)
|
0.27 (–0.53 to 1.08)
|
p = 0.51
|
|
Bernard, 1993 (38) – Exercise sessions
|
5
|
|
|
|
|
|
Exercise repetitions
|
|
35.47 (22.28)
|
33.72 (29.59)
|
0.07 (–0.49 to 0.62)
|
p = 0.82
|
|
Davin, 2005 (42) – Water exercise HR, bpm
|
4
|
|
|
|
|
|
Preferred music
|
|
93.39 (13.94)
|
92.06 (12.43)
|
0.10 (–0.43 to 0.63)
|
p = 0.72
|
|
Non preferred music
|
|
92.92 (14.42)
|
92.06 (12.43)
|
0.06 (–0.47 to 0.60)
|
p = 0.82
|
|
Lee, 2001 (43) – Walking steps
|
2
|
|
|
|
|
|
Fast music
|
|
1,140.06 (145.34)
|
1,248.06 (74.3)
|
–0.91 (–1.64 to –0.18)**
|
p = 0.01
|
|
Slow music
|
|
1,105.38 (147.95)
|
1,248.06 (74.03)
|
–1.19 (–1.94 to –0.44)**
|
p < 0.01
|
|
Pfister et al., 1998 (35) – Walking
|
5
|
|
|
|
|
|
6MWT (m)
|
|
331 (82.82)
|
321 (91.54)
|
0.11 (–0.52 to 0.75)
|
p = 0.73
|
|
Thornby et al., 1995 (36) – Walking
|
6
|
|
|
|
|
|
Exercise time
|
|
13.9 (2.4)
|
11.3 (1.8)
|
1.21 (0.71 to 1.72)*
|
p < 0.01
|
|
Energy expenditure, kcals
|
|
11.8 (6.6)
|
7.7 (4.8)
|
0.70 (0.23 to 1.18)*
|
p < 0.01
|
|
Maximum heart rate, bpm
|
|
104 (18)
|
101 (18)
|
0.16 (–0.30 to 0.63)
|
p = 0.49
|
|
von Leupoldt et al., 2007 (37) – Walking
|
2
|
|
|
|
|
|
6MWT (m)
|
|
479 (84)
|
478 (90)
|
0.01 (–0.61 to 0.63)
|
p = 0.97
|
|
Heart rate (post–pre session difference)
|
|
20.4 (16.9)
|
18.2 (16.7)
|
0.13 (–0.49 to 0.75)
|
p = 0.69
|
|
*p < 0.05 in favour of music; **p < 0.05 in favour of no-music conditions. 6MWT: 6 minute walk test; UL: upper limb; 6MPRB: 6 min peg and ring board test; HR: heart rate; bpm: beats per min; kcals: kilocalories.
|
|
Table IV. Within-session standardized mean differences (95% confidence interval) between live music and no-music
|
|
Study
Outcome measure
|
Quality/10
|
Groups: mean (SD)
|
Standardized mean difference
|
Level of significance
|
|
Music
|
No-music
|
Hedges-g (95% CI)
|
p-value
|
|
Johnson et al., 2001 (39) – Exercise repetitions
|
3
|
|
|
|
|
|
Instrumental – hand & wrist
|
|
27.26 (5.16)
|
24.37 (3.31)
|
0.65 (0.00 to 1.31)*
|
p = 0.05
|
|
Instrumental – marching
|
|
29.47 (9.16)
|
26.79 (5.7)
|
0.34 (-0.30 to 0.98)
|
p = 0.29
|
|
Instrumental – bucket lift
|
|
15.29 (2)
|
17.32 (2.08)
|
–0.97 (–1.65 to –0.30)**
|
p < 0.01
|
|
Vocal – knee extension
|
|
17.89 (4.42)
|
20.13 (4.42)
|
–0.50 (–1.14 to 0.15)
|
p = 0.13
|
|
Vocal – rowing
|
|
9.74 (2.11)
|
8.55 (0.98)
|
0.71 (0.05 to 1.36)*
|
p = 0.03
|
|
Vocal – bucket lift
|
|
15.39 (2.94)
|
17.92 (2.08)
|
–0.97 (–1.65 to –0.30)**
|
p < 0.01
|
|
Vocal – arms across chest
|
|
27.74 (4.75)
|
29.63 (3.9)
|
–0.43 (–1.07 to 0.22)
|
p = 0.19
|
|
Kendelhardt 2003 (44) – Cycling
|
3
|
|
|
|
|
|
Exercise time
|
|
61.65 (16.95)
|
56.1 (13)
|
0.36 (–0.36 to 1.08)
|
p = 0.33
|
|
*p < 0.05 in favour of music; **p < 0.05 in favour of no-music conditions. SD: standard deviation; CI confidence interval.
|
Comparisons of music and an alternative sound or music intervention
Trials comparing music and an alternative sound or music intervention could not be combined in meta-analyses due to clinical heterogeneity. One trial of moderate quality demonstrated that participants with COPD who listened to recorded commercial music increased their within-session walk time until voluntary exhaustion (g = 1.07, 95% CI = 0.58 to 1.57, p < 0.01) and energy consumption (g = 0.62, 95% CI = 0.14 to 1.09, p = 0.01) when compared with grey noise (36). Other trials of low to moderate quality comparing a music intervention with an alternative sound or music intervention did not demonstrate any differences for pre to post program upper extremity repetitions over 4 weeks (34), within-session numbers of steps (43), or within-session mean heart rate (42). A final trial of low quality trial comparing two music interventions only reported results for within-session exercise repetitions during 3 of 19 exercises that favoured specifically composed music compared with commercial recorded music (Table V).
|
Table V. Within-session standardized mean differences (95% CI) between music and alternative interventions
|
|
Study Outcome measure
|
Quality/10
|
Groups: mean (SD)
|
Standardized mean difference
|
Level of significance
|
|
Int 1
|
Int 2
|
Hedges-g (95% CI)
|
p-value
|
|
Alternative sound
|
|
|
|
|
|
|
Lee 2001, (43) – Walking steps
|
2
|
|
|
|
|
|
1 fast tempo commercial vs. 2 natural sounds – steps
|
|
1,140.06 (145.34)
|
1,095.5 (341.44)
|
0.17 (–0.53 to 0.86)
|
p = 0.64
|
|
1 slow tempo commercial vs. 2 natural sounds – steps
|
|
1,105.38 (147.95)
|
1,095.5 (341.44)
|
0.04 (–0.66 to 0.73)
|
p = 0.92
|
|
Thornby et al., 1995 (36) – Walking
|
6
|
|
|
|
|
|
1 commercial music vs. 2 grey noise – time
|
|
13.9 (2.4)
|
11.6 (1.8)
|
1.07 (0.58 to 1.57)*
|
p < 0.01
|
|
1 commercial music vs. 2 grey noise – kcals
|
|
11.8 (6.6)
|
8.2 (4.8)
|
0.62 (0.14 to 1.09)*
|
p = 0.01
|
|
1 commercial music vs. 2 grey noise – maximum HR
|
|
104 (18)
|
101 (18)
|
0.16 (–0.30 to 0.63)
|
p = 0.49
|
|
Alternative music
|
|
|
|
|
|
|
Bauldoff et al., 2005 (34) – UL exercise repetitions
|
6
|
|
|
|
|
|
1 moderate tempo commercial music vs. 2 slow tempo commercial music
|
|
190.1 (24.7)
|
174.4 (23.0)
|
0.63 (–0.27 to 1.53)
|
p = 0.17
|
|
Davin, 2005 (42) – Water exercise mean HR
|
4
|
|
|
|
|
|
1 preferred commercial music vs. 2 non-preferred commercial music
|
|
93.39 (13.94)
|
92.91 (14.42)
|
0.03 (–0.5 to 0.57)
|
p = 0.90
|
|
Lee, 2001 (43) – Walking steps
|
2
|
|
|
|
|
|
1 fast tempo commercial music vs. 2 slow tempo commercial music
|
|
1,140.06 (145.34)
|
1,105.38 (147.95)
|
0.23 (–0.46 to 0.93)
|
p = 0.51
|
|
O’Konski et al., 2010 (41) – Exercise repetitions
|
3
|
|
|
|
|
|
1 composed music vs. 2 commercial music – hand grip
|
|
7.8 (3.11)
|
5.47 (2.83)
|
0.78 (0.35 to 1.21)**
|
p < 0.01
|
|
1 composed music vs. 2 commercial music – shoulder shrug
|
|
5.56 (3.33)
|
4.1 (2.63)
|
0.48 (0.06 to 0.90)**
|
p = 0.02
|
|
1 composed music vs. 2 commercial music – butterfly
|
|
2.35 (1.65)
|
1.26 (1.21)
|
0.75 (0.32 to 1.17)**
|
p < 0.01
|
|
*p < 0.05 in favour of commercial music; **p < 0.05 in favour of composed music. SD: standard deviation; CI confidence interval; Int: intervention; HR: heart rate; UL: upper limb.
|
DISCUSSION
Older adults who listen to recorded commercial music while participating in exercise programs over several weeks may experience medium-term benefits with improved capacity to perform physical activity. Evidence for this finding was demonstrated by two randomized controlled trials of moderate quality that examined participants with COPD performing programs of 8-weeks of walking (33) and 4-weeks of upper body exercise (34). Both trials demonstrated large effect sizes in favour of programs with music compared with no-music, with improvements of 53% for the 6 min walk test (33) and 31% for upper limb exercise repetitions (34). These two trials differed from other studies in the review as they examined the between-session cumulative effects of music on physical activity. All other studies in the review reported within-session short-term effects while participants performed physical activity and listened to music.
Trials that examined within-session differences did not provide evidence demonstrating that music interventions offered physical activity benefits compared with no-music or an alternative sound for older adults during exercise. Meta-analyses were hampered by imprecision but did not demonstrate any clear within-session differences in exercise duration, walking distance, or heart rate during conditions with recorded commercial music compared with no-music. Only one moderate quality trial demonstrated increased within-session exercise duration and energy consumption during conditions with recorded commercial music when compared with no-music and grey noise (36).
Although older adults who exercise while listening to recorded commercial music did not appear to experience enhanced within-session physical activity, they may demonstrate cumulative effects with improved endurance following exercise programs with music over a number of weeks. A plausible reason for this enhanced capacity to perform physical activity is that participant attendance (exercise adherence) may have been greater during exercise programs when music was provided. However, 3 trials comparing participant attendance during conditions with music and no-music did not demonstrate any differences (33, 34, 40). It is also possible that small within-session differences over a program of sessions might result in measurable improvements with increased capacity to perform physical activity over time.
While individual studies that used recorded commercial music interventions provided some evidence demonstrating increased physical activity in older adults, there were no indications that live music or specifically composed music offered any benefits. Neither live or specifically composed music demonstrated any measureable effect on numbers of exercise repetitions completed by older adults (39–41), and live music did not increase the voluntary time to exhaustion in older adults performing stationary cycling (44). However, trials that examined live and specifically composed music only included within-session outcome measures. Given indications that recorded commercial music may improve exercise performance over the medium-term, it would be useful to investigate the cumulative effects of live and specifically composed music. However, based on the current evidence in this review no conclusions can be drawn about the superiority of one form of music intervention over another.
Recorded commercial music offers advantages over live music or specifically composed music, as it is accessible and inexpensive. However, to maximize the effects of recorded commercial music during exercise, it is important to consider individual music preferences and exercise requirements (45). For example, consideration of music preferences would respect cultural influences and extra-musical associations, while exercise requirements might determine the rhythm, form and length of song selections (45). Of the trials in the review that investigated recorded commercial music, one examined group preferences (42) and the others included researcher selections. Only two trials considered tempo (34, 43), and there was minimal reporting of other music qualities such as lyrics, melody, form or harmony. Future research might consider using participant selected music with qualities that are matched to the physical activity being performed.
The trials included in this review had a number of limitations. Of the 12 included studies, there were only 3 randomized controlled trials. Meta-analyses were conducted using trials with small sample sizes, which reduces the certainty of conclusions. Overall trial quality was a limitation with none that concealed allocation or blinded therapists assessing outcome measures. In addition, two trials reported selective results indicating publication bias, and other studies did not provide sufficient data to determine effect sizes.
In conclusion, this review presents limited evidence from two individual trials of moderate quality that older adults who listen to recorded commercial music during exercise programs over several weeks may experience cumulative benefits with increased capacity to perform physical activity. There is no current evidence to support the use of live music or specifically composed music. Further high quality research with carefully considered music interventions is recommended to demonstrate the cumulative and short-term effects of music on physical activity with older adult populations.
References