Anne-Mette Momsen, PhD1, Jens Ole Rasmussen, PT2, Claus Vinther Nielsen, MD1,5, Maura Daly Iversen, DPT, SD3,4 and Hans Lund, PhD4
From the 1MarselisborgCentret, Public Health and Quality Improvement, Central Denmark Region, 2Clinic of Physiotherapy, Wichmandsgade, Odense, Denmark, 3Department of Physical Therapy, School of Health Professions, Bouve College of Health Sciences, Northeastern University, and Section of Clinical Sciences, Division of Rheumatology, Brigham & Women’s Hospital, Harvard Medical School, Boston, USA, 4Research Unit for Musculoskeletal Function and Physiotherapy, The Institute for Sports Science and Clinical Biomechanics, University of Southern Denmark and 5Section of Clinical Social Medicine and Rehabilitation, Institute of Public Health, Aarhus University, Aarhus, Denmark
OBJECTIVES: To systematically investigate current scientific evidence about the effectiveness of multidisciplinary team rehabilitation for different health problems.
DATA SOURCES: A comprehensive literature search was conducted in Cochrane, Medline, DARE, Embase, and Cinahl databases, and research from existing systematic reviews was critically appraised and summarized.
STUDY SELECTION: Using the search terms “rehabilitation”, “multidisciplinary teams” or “team care”, references were identified for existing studies published after 2000 that examined multidisciplinary rehabilitation team care for adults, without restrictions in terms of study population or outcomes. The most recent reviews examining a study population were selected.
DATA EXTRACTION: Two reviewers independently extracted information about study populations, sample sizes, study designs, rehabilitation settings, the team, interventions, and findings.
DATA SYNTHESIS: A total of 14 reviews were included to summarize the findings of 12 different study populations. Evidence was found to support improved functioning following multidisciplinary rehabilitation team care for 10 of 12 different study population: elderly people, elderly people with hip fracture, homeless people with mental illness, adults with multiple sclerosis, stroke, aquired brain injury, chronic arthropathy, chronic pain, low back pain, and fibromyalgia. Whereas evidence was not found for adults with amyetrophic lateral schlerosis, and neck and shoulder pain.
CONCLUSION: Although these studies included heterogeneous patient groups the overall conclusion was that multidisciplinary rehabilitation team care effectively improves rehabilitation intervention. However, further research in this area is needed.
Key words: rehabilitation; patient care team; outcome assessment; multidisciplinary team.
J Rehabil Med 2012; 00: 00–00
Correspondence address: A. M. Momsen, MarselisborgCentret, P. P. Oerums Gade 11, DK-8000 Aarhus C, Denmark. E-mail: anne-mette.momsen@stab.rm.dk
Submitted January 27, 2012; accepted June 7, 2012
Introduction
In Denmark, as in other Western countries, the population is ageing, and, consequently, chronic diseases are increasing. Yet problems with rehabilitation remain that cannot be adressed with medicine or surgery. Healthcare changes, including a reduction in the number of hospitals, increased numbers of specialized hospitals and shorter hospital stays, have resulted in a greater demand for rehabilitation. Under the 2006 Danish Health Act, responsibility for the rehabilitation of patients shifted towards local authorities in the municipalities (1). This shift of responsibility requires cooperation and coordination between health sectors and local authorities, and highlights the need for standards and guidelines for rehabilitation services. In addition, as rehabilitation requires the expertise of various disciplines, methods for improving the performance of interdisciplinary teams are paramount.
Rehabilitation has been defined in the Danish White Paper as: “A goal-oriented, cooperative process involving a member of the public, his/her relatives, and professionals over a specified period of time. The aim of this process is to ensure that the person in question, who has, or is at risk of having, seriously diminished physical, mental and social functions, can achieve independence and a meaningful life. Rehabilitation programmes consider the person’s situation and the decisions he or she must make, and consist of coordinated, coherent, and knowledge-based measures” (2).
The World Health Organization (WHO) has defined rehabilitation as “The use of all means aimed at reducing the impact of disabling and handicapping conditions and at enabling people with disabilities to achieve optimal social integration” (3). A comprehensive description of Physical and Rehabilitation Medicine (PRM), which is the medical specialty with rehabilitation as its core health strategy, is well established in all Western countries except Denmark (3).
WHO has created the International Classification of Functioning, Disability and Health (ICF) for assessing health status, for example in relation to rehabilitation (4). The ICF recognizes human functioning as a universal human experience focusing on the consequences and not on the causes of the limits of functioning (5).
Three perspectives regarding good rehabilitation process include: consideration of all aspects of a person’s life, recognizing the individual as the primary focus in the rehabilitation process, and ensuring continuity and related interventions across the sectors (2).
The present challenge is to implement evidence-based optimal rehabilitation interventions between health and social services. The focus of this review is multidisciplinary rehabilitative team care (MTC). MTC can be defined as “a group of diverse clinicians who communicate with each other regularly about the care of a defined group of patients and participate in that care” (6). The characteristics of optimal MTC in rehabilitation include cooperation of all participants in a structured way and directed towards common goals to develop individualized plans, and to evaluate the processes used to achieve these goals (7–9). The purpose of this review is to link knowledge gained from existing work to provide insights into how best to coordinate rehabilitation services across the health and social services and across professions.
The aim of MTC is to optimize the rehabilitation process at all levels according to ICF; body functioning, activity, and participation. Levels of MTC can be divided according to levels of cooperation (7), as follows:
(A) Interdisciplinary – the highest level in which team members work towards shared goals.
(B) Multidisciplinary – different professionals work with the same person, but within their own professional limits and often without knowledge about each other’s practice.
(C) Transdisciplinary – professionals cross the border into another team member’s professionalism.
(D) Unidisciplinary/intradisciplinary – only focused on one’s own profession.
This review highlights research addressing the cooperation of professionals defined in levels (A) and (B), using the overall term “multidisciplinary team care”. In MTC the professionals work towards shared goals using a common approach or strategy. Among PRM specialists, the preferred pattern of team working is “interdisciplinary working”. However, published studies have tended to use the term “multidisciplinary team” (10).
Aim
The primary aim of this literature review was to highlight current scientific evidence about MTC in rehabilitation in different categories of patient groups. A secondary aim was to evaluate whether rehabilitation based on MTC is more effective compared with a control or usual rehabilitation intervention.
MethodS
Inclusion criteria were: systematic review; no restrictions in type of populations, all types of patient groups considered; no restrictions in type of outcome measures, all types of outcome measures; and MTC defined as cooperation of all participants in a structured way towards a common goal, development of individualized plans in order to attain this, and evaluation of the process towards the goals.
Literature search
Data sources. We searched for critically appraised and summarized research from existing systematic reviews and meta-analyses without restrictions in terms of study population or outcomes, which were published between 2000 and July 2010 (Table I). Agreement on the criteria for selecting studies, quality assessment, and data extraction and conclusions was reached by consensus. The types of rehabilitation interventions included in this review were either multidisciplinary, interdisciplinary team or team care, respectively. The main search terms used were “rehabilitation”, “interdisciplinary or multidisciplinary” and “health care team” or “patient care team”. The search was carried out in the Cochrane Database of Systematic Reviews, Database of Abstract of Reviews of Effects (DARE), Medline, Embase and Cinahl.
The search was carried out on 2 July and 5 July 2010. One reviewer (JOR) used a common search strategy for Cochrane, DARE, and Medline, while search strategies were modified appropriately by a librarian for Embase and Cinahl. The complete search strategy is available in Appendix S1 (available from http://www.medicaljournals.se/jrm/content/?doi=10.2340/16501977-1040).
Two reviewers (A-MM, JOR) independently reviewed all titles and identified potentially relevant studies based on abstracts. Full papers were retrieved if the abstract provided insufficient data to enable selection. Inclusion criteria were applied to full papers of potential reviews by one of the reviewers.
Study selection. This review is based primarily on systematic reviews, inasmuch as they may be a better guide than original studies and they generally focus on randomized controlled trials (RCTs), which are regarded as providing the most reliable estimates of effects (11). In addition to the fact that systematic reviews are considered to be the highest level of evidence (11), a compilation of systematic reviews with the same focus will increase both implementation of the achieved knowledge, and thereby increase the quality of daily clinical practice. Overviews compile evidence from multiple systematic reviews into a single accessible and usable document. Each overview has its specific focus, for which there are two or more potential perspectives (for example different patient groups, but the same type of intervention).
Inclusion criteria for this review are shown in Table I by the type of study, population, intervention, and outcome measures. To capture the most recent RCTs, only the most recent systematic reviews and meta-analysis for each study population were included. The search was not restricted to specific languages, but captured only English language reviews for inclusion. Exclusion criteria were: single studies without a control group or without a description of the search strategy. To improve the consistency of the search strategy, preliminary criteria were pilot-tested in abstracts on a sample of articles from the initial search. Two reviewers independently assessed the scientific quality using the 10-item Overview Quality Assessment Questionnaire (OQAQ) and consensus was reached prior to reporting (12, 13).
|
Table I. Overview of reviews on multidisciplinary team care (MTC) in rehabilitation |
|||||
|
Author, year, Country OQAQ-score |
Patient group (title) Studies Sample size Countries |
Setting interventions |
Team professions |
Outcomes at ICF-levels: Body functioning (B) Activity (A) Participation (P) |
Findings and conclusion |
|
Johansson et al., 2010 (14) Sweden Minimal flaws |
Elderly persons Multidisciplinary team, working with elderly persons living in the community. 28 studies (12 RCTs) n = ---7,173 in RCTs Western countries (8 RCTs from USA) |
a) In-patient and follow-up at home (6 RCTs) b) Primary care (5 RCTs) c) Community care (1 RCT) Apart from MTC, very heterogeneous interventions Controls: Not described |
Minimum 2, most often 3–4 professions. Order of frequency of professions: 1. nurse 2. occupational therapist 3. physiotherapist 4. social worker 5. physician |
B: A: Functional capacity ADL, social activity P: Rate of falls Hospital stay (days) Re-admission rate No specific clinical outcomes |
a) Improved functional capacity (3 RCTs), mental health (1 RCT), and self-perceived health and life satisfaction (1 RCT) Reduced episodes of falling (2 RCTs), and shortened stay/delayed readmission to hospital or nursing home (3 RCTs) b) Improved ADL (2 RCTs), increased social activity (2 RCTs), and general well-being and life-satisfaction (3 RCTs) Reduced deterioration of health and functional ability (3 RCTs). Continuous evaluation and management benefitted the possibility of maintaining health status and improving of health perception (4 RCTs) c) Improved survival, ADL, use of adaptive strategies, self-efficacy, and reduced fear of falling CONCLUSION: In summary MTC showed significant effects vs. control group on health status and perception, activity and admission to hospital |
|
Handoll et al., 2009 (17) UK Minimal flaws |
Hip fractures Multidisciplinary rehabilitation for older people with hip fractures. 13 RCTs n = 2,498 Western countries, Taiwan (1 RCT) |
a) In-patient (11 RCTs): b) Out-patient ambulatory rehabilitation (2 RCTs) Interventions very heterogeneous apart from MTC Controls: Usual care, but very different |
Rehabilitation delivered by a multidisciplinary team.
|
B: A: Barthel Index (3 RCTs) modified Barthel Index (3 RCTs) P: Mortality Rate of falls Hospital stay (days) Readmission rate Requirement for institutional care |
a) Data pooled from 8 RCTs showed a non-statistically significant tendency in favour of the intervention for readmission rate (RR 0.89, 95% CI 0.78–1.01) at long-term follow-up Mortality data were reported for all 11 RCTs, show no statistically significant difference in mortality at the scheduled end of follow-up (RR 0.90, 95% CI 0.76–1.07) Individual trials found better results, often short-term only, in the intervention group for ADL and mobility b) The trial comparing primarily home-based MTC with usual inpatient care found marginally improved function and a clinically significantly lower burden for carers in the intervention group One trial found no significant effect from doubling the number of weekly contacts at the patient’s home from a multidisciplinary rehabilitation team. CONCLUSION: Data showed significantly lower burden for carers, a tendency for a decrease in requirement for institutional care, and marginally improved function |
|
Langhorne, 2007 (21) UK Minimal flaws |
Stroke Organised inpatient (stroke unit) care for stroke Stroke unit care versus general wards: 26 RCTs n = 5,592 Part of 31 RCTs, which aim was to compare more organized vs. less organized services Countries not given |
MTC in stroke units Controls: a) Care in general wards (acute medical or neurology ward without routine multi-disciplinary input) b) Care in less organized services |
A mobile stroke team that exclusively manage stroke patients in a dedicated ward or within a generic disability service (mixed rehabilitation ward) |
B: A: Barthel index (15 RCTs) Participation: Mortality Many different |
a) Stroke unit vs. general wards showed reductions in the odds of: Death at follow-up (median 1 year), OR 0.86; 95% CI 0.76–0.98; p = 0.02, death or institutionalised care, OR 0.82; 95% CI 0.73–0.92; p = 0.0006, death or dependency, OR 0.82; 95% CI 0.73–0.92; p = 0.001 b) Stroke rehabilitation vs. alternative services (6 RCTs) showed a pattern of improved outcomes in the stroke rehabilitation ward with statistically significantly fewer deaths (p < 0.05) and a statistically non-significant trend for fewer patients with the composite end-points of death or requiring institutional care and death or dependency. However, the numbers were small and no definite conclusions could be drawn CONCLUSION: Stroke unit (MTC rehabilitation) showed significant reduction in mortality and a tendency towards decrease in requirement for institutional care |
|
Khan et al., 2007 (28) Australia 2005 Minimal flaws |
Multiple sclerosis Multidisciplinary rehabilitation for adults with multiple sclerosis 8 (7 RCTs) n = 747 England, Italy, USA |
MTC – not described a) In-patient (3 RCTs), b) Out-patients (4 RCTs) c) Home care (1 RCT) Controls: Routinely local service, minimal level of interventions, or waiting list |
Two or more professions in connection with a doctor’s consultation |
B: Symptoms Expanded Disability status scale (5 RCTs) 13 other outcomes (1–2 RCTs) A: Functional independence measure (3 RCTs) 6 other outcomes (1–2 RCTs) P: SF-36 (6 RCTs) 16 other outcomes (1–2 RCTs) Length of stay 7 other outcomes (1–2 RCTs) |
a) There was strong evidence that despite no change in the level of impairment, in-patient MTC rehabilitation can produce short-term gains at the levels of activity (disability) and participation for patients with multiple sclerosis b), c) There was limited evidence for short-term improvements in symptoms and disability with high-intensity programmes, which translated into improvement in participation and QoL Although some studies reported potential for cost-savings, there is no convincing evidence regarding the long-term cost-effectiveness of these programmes CONCLUSION: There was strong evidence for gains in QoL for low intensity MTC programmes conducted over a longer period, and for MTC improving short-term levels of activity and participation |
|
Ng et al., 2009 (29) Australia 2009 Minimal flaws |
Amyotrophic lateral sclerosis or motor neuron disease Multidisciplinary care for adults with amyotrophic lateral sclerosis or motor neurone disease 5 observational studies (0 RCT/CCT) 4 Western countries, Cuba |
a) Low-intensity b) High-intensity |
|
B: A: Disability P: Mortality Hospital stay |
The best evidence to date is based on these 5 studies, 3 “low” and 2 “very low quality” observational studies a) They suggest “very low quality evidence” for an advantage for only mental health domains of QoL without increasing healthcare costs, and “low level quality” evidence for reduced hospitalisation for MTC in low-intensity outpatient settings; b) They find “very low quality” evidence for improved disability in high-intensity settings CONCLUSION: The evidence is low quality for improved disability and mental QoL, and the evidence for survival is conflicting |
|
Turner-Stokes et al., 2005 (30) UK 2008 Minimal flaws |
Acquired brain injury Multi-disciplinary rehabilitation for acquired brain injury in adults of working age – traumatic brain injury – diffuse acquired brain injury – cerebrovascular accident (stroke) – other causes 16 RCTs n = 1,789 Countries unknown |
a) In-patient, milder ambulatory patient (5 RCTs) n = 1258 b) In-patient rehabilitation (2 RCTs) n = 111 c) Out-patient physiotherapy and occupational therapy (2 RCTs) n = 182 d) Community-based MTC care (3 RCTs) n = 238 Heterogeneous interventions except MTC Controls: Routinely local service, minimal level of interventions, or waiting list In-patient vs. out-patient |
MTC defined as any intervention delivered by 2 or more disciplines working in coordinated effort to meet these objectives |
B: Rivermead post-concussion symptoms questionnaire (3 RCTs) More outcomes (1–2 RCTs) A: Barthels Index (4 RCTs) Functional independence measures (3RCTs) More outcomes (1–2 RCTs) P: Return to work SF-36 (3 RCTs) More outcomes (1–2 RCTs) |
a) The general conclusion was that intervention in a totally unselected group of patients with mild traumatic brain injury was not effective. Both the treatment group and control intervention group made substantial gains in terms of reduced post-concussion symptoms and enhanced participation, including return to work No significant differences were recorded between groups a) There is limited evidence that specialist in-patient rehabilitation services can improve functional outcome in terms of activity (reduced disability) vs. home-based or other rehabilitation b) There is moderate evidence that out-patient therapy improves the outcomes of stroke rehabilitation, with limited evidence that more intensive treatment regimens are associated with better outcomes There is indicative evidence that this type of intervention may be effective even late (at least 1 year) after stroke. In general, there is moderate evidence for improved functional outcome and indicative evidence for MTC has a long-term effect c) There is limited evidence that multidisciplinary, community-based rehabilitation can improve functional outcome (disability), especially when targeted towards specific goals CONCLUSION: For improvement of functional outcome at the ICF-level of activity there is limited evidence for in-patient and community-based MTC rehabilitation, and moderate evidence for out-patient therapy There is strong evidence that more intensive rehabilitation programmes (4 RCTs, n = 360) are associated with earlier function gains, once patients are fit to be engaged |
|
Kahn et al., 2008 (18) Australia 2006 Minimal flaws |
Chronic arthropathy (joint replacement at the hip and knee) Multidisciplinary rehabilitation programmes following joint replacement at the hip and knee in chronic arthropathy. 5 RCTs n = 619 Western countries |
In-patient (2 RCTs) n = 261) Home-based (3 RCTs, n = 358): Heterogeneous interventions except MTC Controls: routine care |
Minimum 2 professions in the team |
B: Oxford Hip score (2 RCTs) A: Transfer Ambulation 9 other outcomes (1 RCT) P: Hospital stay Complication Readmission rate 5 other outcomes (1 RCT) |
a) Early commencement of rehabilitation and clinical pathways led to more rapid attainment of functional milestones, Functional Independence Measures (FIM): transfer WMD 0.5, 95% CI 0.15, 0.85, number needed to treat to benefit (NNTB) = 6, ambulation WMD 1.55 (95% CI 0.96, 2.14), NNTB = 3), shorter hospital stay, fewer post-operative complications and reduced costs in the first 3–4 months b) MTC improved functional gain: Oxford Hip Score (OHS) WMD at 6 months –7.00 (95% CI –10.36, –3.64), NNT = 2, QoL and reduced length of hospital stay in the medium term (6 months) CONCLUSION: Silver level evidence that early MTC rehabilitation can improve outcomes at the level of activity and participation |
|
Scascighini et al., 2008 (22) Switzerland 2006 Minimal flaws |
Chronic pain Multidisciplinary treatment for chronic pain. (back pain, fibromyalgia, chronic pain syndrome) 35 RCTs n = 2,407 Countries not given |
a) In-patient (5 RCTs) b) Out-patient (18 RCTs) 4 RCTs compared the 2 settings Interventions not described Controls: Usual care, waiting list, or attention control mono-disciplinary |
Minimum 3 of the following therapies: psychotherapy, physiotherapy, relaxation, techniques, medical treatment, patient education, vocational therapy |
B: Pain, emotional strain A: Pain behaviour, disability, coping, physical capacity P: QoL, return to work, sick leave, use of medicine/ healthcare system |
MTC vs. usual care or vs. waiting list: 13 of 15 RCTs showed positive effects MTC vs. other control group treatment: 10 of 15 RCTs showed positive effects CONCLUSION: In general MTC showed significant effects on all ICF-levels of outcomes |
|
Norlund et al., 2009 (25) Sweden Minimal flaws |
Low back pain Multidisciplinary interventions: Review of studies of return to work after rehabilitation for low back pain 7 RCTs, n = 1,450 Western countries, 5 in Scandinavia |
Heterogeneous interventions Controls: Out-patient physical training, group education Control treatment as usual, physical therapy |
Two or more healthcare disciplines |
P: Return to work Sick leave (days) SF-36 |
The meta-analysis of all 7 RCTs shows (despite heterogeneity) a significant difference of effect on return to work (15%, i.e. RR 1.15) The meta-analysis including Scandinavian RCTs only shows an even larger difference of effect (21%, i.e. RR 1.21), which is of reasonable clinical relevance CONCLUSION: MTC rehabilitation for low back pain shows a significant effect on return to work |
|
Geen van et al., 2007 (26) Minimal flaws |
Low back pain (back training) The long-term effect of multidisciplinary back training 10 studies (5 RCTs), n = 1,958 Western countries |
Heterogeneous interventions. 2–4 healthcare professionals Controls: No treatment, low-intensity multidisciplinary back training
|
Involvement of several disciplines: psychologists, physiotherapists, occupational therapists, and/or medical specialists |
B: Pain severity Functional status A: More outcomes P: Ability to work QoL More outcomes
|
Three of the 4 high-quality RCTs that used work participation as an outcome reported a positive effect on this measure All the high-quality studies found a positive effect on at least 1 of the 4 outcome measures used, whereas none of the low-quality studies reported effectiveness Only 1 of 7 studies reported a positive effect on experienced pain and functional status. Only 2 studies used QoL as an outcome measure, effectiveness was reported by 1 of these CONCLUSION: The high-quality RCTs reported positive effects on participation outcomes, only 1 study reported effects on ICF-levels of impairment (B) |
|
Karjalainen et al., 2003 (24) Finland Minimal flaws |
Subacute low-back Multidisciplinary bio psychosocial rehabilitation for subacute low back pain among working age adults 2 RCTs, n = 233 Sweden, Canada |
a) Graded 4-part activity program. b) Occupational and clinical intervention Controls: Traditional care, occupational intervention, clinical intervention or usual care |
Physician’s consultation plus either a psychological, social or vocational intervention, or a combination of these |
B: Pain intensity (McGill) More outcomes A: Functional status More outcomes P: Return to work More outcomes |
CONCLUSION: There was moderate scientific evidence showing that MTC rehabilitation, which includes a workplace visit or more comprehensive occupational healthcare intervention, helps patients to return to work faster, results in fewer periods of sick leave and alleviates subjective disability |
|
Karjalainen et al, 2003 (31) Finland 2002 Minimal flaws |
Neck and shoulder pain Multidisciplinary bio psychosocial rehabilitation for neck and shoulder pain among working age adults. 1 RCT, 1 CCT n = 177 |
a) Physical training, information, education, social inter-action, work place visit. b) Multimodal Cognitive behavioural treatment, administered by a clinical psychologist directly to patients. Controls: Physiotherapy, medication, rest and sick leave. Psychologist (coaching other professionals. |
MTC had to consist of a physician’s consultation plus either a psychological, social or vocational intervention, or a combination of these |
B: Pain (VAS) More outcomes A: Health Assessment Questionnaire Generic functional status P: Sick leave Days off in 6 months Costs US$/patient |
a) Effects of the MTC programme did not differ from traditional care in any of the outcomes assessed at 12- and 24-months follow-up b) No significant difference between the 2 groups in any of the assessed outcomes besides the cost of the rehabilitation programme. The intervention (where a psychologist executed the behavioural component of the rehabilitation) was less cost-effective than the control intervention (where a psychologist merely advised the rehabilitation team) CONCLUSION: There was no difference between effect of the MTC and traditional care |
|
Burckhardt et al., 2006 (23) USA Major flaws |
Fibromyalgia Multidisciplinary Approaches for Management of Fibromyalgia 10 (8 RCTs, 2 CCT) n = 1340 |
Exercise (7 RCTs), Exercise combined with education (6 RCTs), (3 of these with cognitive behavioural therapy) Controls: Mono-intervention no treatment, or waiting list |
Not defined Professionals not given |
B: Pain (VAS,NRS) (8 RCTs) A: Different outcomes P: Fibromyalgia Impact Questionnaire (FIQ) (4 RCTs) Arthritis Self-Efficacy Scale (4 RCTs) Self-efficacy |
Self-efficacy was significantly enhanced in the treated groups in 4 of the 5 groups, and the score of overall FIQ was significantly decreased in 3 of 5 studies Pain measured by a VAS was significantly decreased in 4 of 8 trials Eight of the controlled trials collected follow-up data between 3 months and 1 year after completion of the experimental treatment. In 6 studies treatment gains were maintained CONCLUSION: Studies with MTC approaches show significant increase in self-efficacy and decrease in total score of FIQ and pain at 3 months and 1 year follow-up. |
|
Coldwell et al., 2007 (32) USA Minimal flaws |
Homeless with severe mental illness The effectiveness of assertive community treatment for homeless population with severe mental illness: a meta-analysis 10 studier (6 RCTs) n = 5775 Countries not given |
Assertive Community Treatment. Controls: Standard case management |
Team of professions within: social work, rehabilitation, counselling, nursing and psychiatry provided Assertive Community Treatment services |
B: Colorado Symptom Inventory score Brief Psychiatric Rating Scale Global Severity Index score P: Different outcomes of homelessness Hospitalization |
The summary effect across RCTs was 37% (95% CI = 18%–55%, Z = 3.85, p = 0.0001), signifying that assertive community treatment subjects, experienced a 37% greater reduction in homelessness compared with standard case management subjects The summary effect revealed no significant difference in hospitalization, 10% (95% CI = –7%–27%, Z = 1.17, p = 0.24). When combined, assertive community treatment subjects averaged a 26% (95% CI = 7%–44%, Z = 2.76, p = 0.006) further symptom improvement in randomized trials CONCLUSION: Assertive community treatment subjects had significant reductions in psychiatric symptom severity beyond that experienced by comparison subjects |
|
RCTs: randomized controlled trial(s); CCT: controlled clinical trial(s); ADL: activity of daily living; RR: relative risk; OR: odds ratio; CI: confidence interval; QoL: quality of life; OQAQ: Overall Quality Assessment Quality; FIQ: fibromyalagia impact. |
|||||
Data extraction. Data on study design, source population, sample size, setting, team, intervention, length of follow-up, and outcome were extracted from the selected reviews by one reviewer (JOR).
Results
The initial search for rehabilitation and MTC yielded a total of 1,892 articles (Fig. 1): 22 records in the Cochrane database, 8 in DARE, 1,372 in Medline, 437 in Embase, and 53 in Cinahl. All titles were screened after duplicates were removed (383), and abstracts of the potentially relevant articles (236) were reviewed.
Fig. 1. Flow diagram.
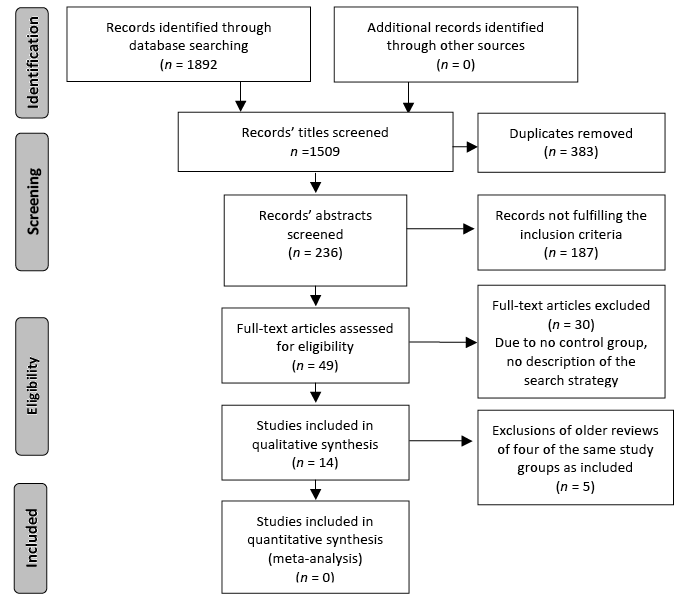
A number of reviews represented the same study population, thus we included the most recent review. For elderly people we identified 2 reviews (14, 15). For arthropathy and hip fractures there were 2 reviews, respectively (16–19). For stroke we found 3 reviews of interventions in different settings (either stroke units or at home) (15, 20, 21). For musculoskeletal diseases MTC reviews covered chronic pain (22) and fibromyalgia (23). Some of the reviews did not include RCTs. For low back pain there were reviews on sub-acute and chronic pain (24, 25), respectively and a review on back training (26). After selecting 49 articles for full text reading, 14 articles met our inclusion criteria.
To summarize the findings of MTC in rehabilitation, 14 systematic reviews were included, of which 7 were Cochrane Reviews. This yielded a total of 182 studies and 26,819 participants. Results for MTC for 12 different populations were reported: elderly persons living in the community, older people with hip fractures, adults with stroke, multiple sclerosis, amyotrophic lateral sclerosis, chronic arthropathy, acquired brain injury, chronic pain, back pain, neck and shoulder pain, fibromyalgia, and homeless people with severe mental illness. The extracted information, the OQAQ score of the review, and conclusions about the effect of MTC were organized by patient category (Table I). The OQAQ score of review with fibromyalgia (24) showed major flaws, whereas the other reviews scored minor flaws.
Table II presents some characteristics and examples of possible changes by MTC in rehabilitation with reference to the included studies.
|
Table II. Characteristics of rehabilitation and possible changes by multidisciplinary rehabilitation team care (MTC) |
|
|
Characteristics of rehabilitation |
Possible changes due to the MTC interventions in the reviews |
|
An individually adjusted intervention |
The person in need is the focus of the intervention (23) Each professional is obliged to care for only a few persons in need, which leads to a more intensive contact with each person (32) Offers in the local community, give a more direct contact instead of intermediate communication (32) A 24-h covering service provides possibilities for contact with professionals (32) |
|
All relevant parts are involved |
The MTC is either a trans- and/or an inter-disciplinary intervention (14, 21) Habitually, the nursing staff is involved in the rehabilitation (21) The workplace is more often involved in return to work after rehabilitation (24, 25) |
|
Working towards a common goal and common assessment of efficiency |
Documents on common agreements, goals, guidelines for the team’s work are elaborated (14) Follow-up is regarded as important and realized (30) |
|
Frequent contacts between all parties involved |
Honest and continuous communication about planning and setting goals is taking place (14) There are close relations in cooperation, awareness of communication, and sharing of knowledge within the team (14) To coordinate MTC joint conferences are held at least once a week (21) |
|
A high professional standard |
Regular education and training programmes for the professionals are implemented (21) |
Table III shows a summation of results from the included studies graded after the level of evidence (A: quantitative analyses (meta-analyses) based on RCTs; B: qualitative analyses based on RCTs, qualitative or observational studies.)
A brief summary of potential implications for the practice of MTC in rehabilitation is presented here:
|
Table III. Summation of the reviews’ results on multidisciplinary rehabilitation team care, graded after level of evidence |
|
|
Outcomes, ICF-levels |
Results, review(s), level of evidence A: based on meta-analysis, RCTs; B: based on RCTs, OCTs and observational studies |
|
Body functioning |
More effect on functional status (18) A, (14) B Faster recovery of functional status (18) A Less reduction of function and health (14) B Better mental status (14) B Less psychiatric symptoms (32) A Increased well being and satisfaction with life (14) A, (23) B |
|
Activity
|
Increased level of ADL and performance of ADL (14) B Less falling and fear of falling (14) B |
|
Participation |
Less dependence on help from others (23) A, (21) B More self-efficacy (21) A, (14) B Increased social participation (1) B Faster return to work (24) A Less sickness absence (25) A |
|
Other outcomes |
Better survival (21) A, (14) B Fewer admissions to hospitals (32) A Shorter stay in hospital (18) A, (14) B Fewer post-operative complications (18) A Later readmission to hospitals or moving to residential homes (14) B |
|
ICF: International Classification of Functioning, Disability and Health; RCT: randomized controlled trials(s); ADL: activities of daily living; OCT(s): observational controlled trial(s). |
|
For elderly people living in the community MTC can lead to (14):
• Increase in the elderly persons’ capacity (performance) and participation.
• Potential improvements in ADL, and self-reported life satisfaction.
• Decreased falls, removal from home.
• Decreased length of hospital stay, and readmissions to hospitals.
Home-based MTC for elderly people with hip fractures showed favourable results compared with inpatient MTC regarding (17):
• Patient functioning.
• Health professional strain.
Length of hospital stay decreased, and rehabilitation time increased.
No conclusions can be drawn from the review due to study heterogeneity. The data suggest trends for effects on all outcomes, and MTC does not increase the costs compared with standard treatment.
For adults with stroke, MTC showed significant improvement in (21):
• Potential chances to survive (death rate).
• Being independent and living at home one year after the stroke.
• Trend towards less required institutional care.
However, no definite conclusion could be drawn due to small sample sizes.
The convincing impact of a stroke unit is probably due to a number of factors (27) including: the mixture of professional’s inasmuch to the structure and location of the unit, the fact that these professionals share a special interest in stroke and rehabilitation and regular educational programmes (conferences held at a minimum of once a week). A primary factor is the organization with integration of the nursing staff into rehabilitation, the training of professionals, and specialized nursing care these patients routinely receive.
For adults with multiple sclerosis there was strong evidence for benefits regarding (28):
• Activity and participation outcomes with in-patient MTC.
• Quality of life (QoL) from less intensive, but long-term, MTC interventions.
• There was limited evidence for highly intensive home or municipality-based interventions.
MTC for adults with amyotrophic lateral sclerosis revealed a lack of RCTs, but the authors mention a number of single interventions with published effects (29).
For adults with acquired brain injury there was evidence for effect on (30):
• Participation (including return to work from intensive in-patient MTC and community-based MTC rehabilitation).
For adults with chronic arthropathy MTC improved the following outcomes (13):
• Functional capacity.
• Reduced hospital stay.
MTC had to commence early after joint replacement.
For adults with chronic pain there was strong evidence for a number of different interventions’ positive effects at all ICF levels (22):
• Body functioning (e.g. pain).
• Activity (e.g. physical capacity, pain behaviour, emotional strain).
• Participation (QoL, return to work, use of healthcare).
The programmes used in these studies varied from 3 to 15 weeks and involved a number of health professionals.
For adults with chronic low back pain the meta-analyses showed strong evidence of MTC rehabilitation (25):
• Return to work improved by 21%.
The MTC rehabilitation was based on group intervention, workplace visit and involved 2 or more healthcare disciplines.
Multidisciplinary back training showed positive effects on participation outcomes only (26):
• Work participation and QoL (1 RCT).
The intervention involved 2 or more professionals (26).
For adults with sub-acute low back pain there was moderate evidence (2 RCTs) on (24):
• Faster return to work.
MTC interventions involved workplace visit or more comprehensive occupational healthcare.
For adults with neck and shoulder pain the 2 MTC interventions (1 RCT) showed no significant difference at 1–2 years follow-up (31).
For fibromyalgia MTC interventions (4–24 weeks) showed significant effects on all ICF levels of outcomes (23):
• Body functioning (symptoms).
• Activity (self-efficacy).
• Participation (return to work and QoL).
For homeless with severe mental illness, the meta-analysis showed significant effects on 2 ICF levels (32):
• Psychiatric symptoms reduced by 26%.
• Homelessness reduced by 37%.
In the following section we present 3 examples of MTC studies in rehabilitation:
(i) MTC intervention for adults with acquired brain injury (30).
“The study involved meetings with the principal investigator, neuropsychological and personality assessment, and consultation with a physical therapist who specializes in post-concussion problems.
The purpose of the study was to compare an education-oriented single session treatment (SS) to a more extensive assessment, education, and treatment-as-needed intervention (TAN) for adults with mild traumatic brain injury (MTBI).
Persons in the SS group met with the principal investigator and discussed any concerns they had about their injury. They also read the National Head Injury Foundation’s Minor Head Injury brochure, chosen because of its reported helpfulness in a previous MTBI treatment study, and discussed any questions about it with the principal investigator.
Subjects were told that no further MTBI treatment would be provided as part of the study, and that any further concerns should be addressed with their family physician.
Persons in the TAN group received the same base treatment along with a 3–4 hour neuropsychological and personality assessment, consultation with a physical therapist who specializes in post-concussion problems (e.g. dizziness), a feedback session on the psychological test results, and thereafter treatment-as-needed for MTBI complaints. The treatment available included further psychological care and physical therapy and access as needed, to the Glenrose Rehabilitation Hospital’s full multidisciplinary outpatient brain injury treatment programme. Treatment for non-MTBI issues was coordinated by the patient’s family physician and provided by the usual community-based services for such non-MTBI problems.
Overall, the aim of SS treatment was to:
• Legitimize the participants’ post-MTBI experience as being “real”, and not brush aside their concerns or tell them that there was nothing wrong with them.
• Educate participants about common complaints after MTBI.
• Provide participants with suggestions about how to cope with common problems, especially by encouraging rest as needed and gradual reintegration into activities.
• Provide reassurance of a good outcome.
• In short, the TAN intervention was an abbreviated model of treatment commonly used, in this setting, with more severe TBI and with MTBI survivors who have persisting, significant complaints” (33).
(ii) A brief summary of an MTC intervention for adults with fibromyalgia (23, 34).
“The professionals of the team were physiotherapists, psychologist, and nurses. The program lasted 6 weeks and consisted of 2 exercise classes and 2 multidisciplinary educational sessions per week. Exercise classes were conducted in a warm, therapeutic pool and were 30 minutes long. Each class consisted of 20 minutes of walking/jogging/side-stepping/arm exercises against water resistance and 5 minutes of stretching at the beginning and end of each class. Educational sessions were one hour long and were run in a group setting, immediately prior to pool classes. During educational sessions, patients were provided with information on exercise, postural correction, activities of daily living, sleep, relaxation, medication, nutrition, and psychosocial coping strategies. The format for the educational sessions varied but included didactic lectures, interactive discussions, and hands-on learning (e.g. relaxation techniques)” (34).
(iii) A synopsis of a study of Assertive Community Treatment (ACT) for homeless people with mental disorders (32).
“The team consisted of 12 full-time equivalent staff, including a program director with a masters’ degree in social work, a full-time psychiatrist and medical director, 6 clinical case managers (social workers, psychiatric nurses, and rehabilitation counsellors), 2 consumer advocates, a secretary-receptionist, a part-time family outreach worker from the Alliance for the Mentally Ill of Metropolitan Baltimore, and a part-time nurse practitioner who treats chronic medical problems. Each patient was assigned to a “mini-team” consisting of a clinical case manager (case load, 10–12 patients), an attending psychiatrist, and a consumer advocate. The entire ACT team, including the consumer advocates, worked together in decision making and each staff member was knowledgeable about most of the patients. Teamwork was fostered through daily sign-out rounds and twice-weekly treatment planning meetings. The ACT team’s long-term commitment was to promote continuity of care, and the team was available 24 hours every day”.
Discussion
In optimal rehabilitation, the focus is on the patient and his/her level of functioning, and not the diagnosis. The process of rehabilitation and the effectiveness of MTC are presented in this review. Specifically, the following elements have been described, and will be discussed (10, 35):
• Identification of the need for rehabilitation.
• Mutually agreed aims and outcomes of MTC and a shared understanding of how to achieve these aims.
• Establishing a team based on the patient’s need with the person in need as a central actor.
• Communication and coordination between all parties involved in the patient’s care including relatives and professionals.
• An appropriate range of knowledge and skills of the MTC team.
• Willingness to share knowledge and mutual trust to speak openly.
• Evaluation of the aims and, if necessary, adjustment of these aims.
Identification of needs
The theory behind the interventions employed in these reviews is not described, except for MTC being “based on the bio-psycho-social thinking” (24, 31). Apart from this theoretical basis there is little evidence about key elements of successful MTC (10, 36).
It is suggested that the framework of the ICF provides elements of a theory about rehabilitation (37, 38). The model provides a taxonomic system of human functioning, and may well be used to help prioritize and provide a description of the composition of the professionals needed to treat different sub-groups. The ICF can be used to test hypotheses about the composition of MTC (39), and as a common framework in which to set criteria for the aim of rehabilitation and how to organize MTC. The process surrounding the development of common goals is described in one review through participation in honest and continuous communication among the patient and professionals involved in the patient’s care (16).
Mutual aims and outcomes
Within the context of treating adults with fibromyalgia, (23, 34) an important goal is to change the patient’s perception of self-efficacy. Through patient education and the use of cognitive behavioural strategies and exercises, patients can learn to move from feelings of hopelessness to taking responsibility for their own health promotion.
As seen in Table II, there are some common characteristics across studies. The diversity of interventions and professionals involved illustrate that MTC can be efficient in several forms. A generalization between different sub-groups is possible, because the interventions typically are focused on common functional problems despite the specific diagnoses.
Establishing a team
The results (Table I) show evidence for MTC in rehabilitation in 10 of the 12 different patient groups. Most studies limited their description of MTC to the professionals involved, and their general performance, such as close cooperation, awareness of communication and sharing of knowledge within the team (16). The element of close contact was described in a review as assignment to a “mini-team” with 24-hour provision of local, direct and individual contact (28).
In certain situations, rehabilitation may require the participation of only one profession for certain periods. Whereas “effective team working produces better patient outcomes (including better survival rates) in a range of disorders, notably following stroke” (10).
Competencies
The components of the MTC interventions were most often described in general terms, such as educational sessions of group therapy, exercise, behavioural cognitive training, and assertive communicative training. We suggest that the CONSORT criteria are used in order to improve the reporting of future RCTs performed in this field (40).
Evaluation of aims
The results demonstrate the heterogeneity of outcomes employed in clinical trials of non-pharmacological interventions. Some reviews have outcomes at all ICF levels, but as Table I illustrates, the outcomes are highly variable and some are lacking the level of participation.
The lack of standard measures appropriate for studying processes of care and the number of different outcomes is a limitation. A set of outcomes would be necessary to compare studies on effectiveness in clinical practice. We suggest use of the ICF to guide the selection of outcomes, and to define influencing factors on functioning. However, unfortunately data are not gathered consistently, and there is no common definition of disability across countries (41). Functioning at all levels is relevant and is the main goal of rehabilitation, and is relevant to disease prevention, cure, and to target strategies for support.
There are some limitations of this review that should be noted. First, the external validity of the review can be questioned, as it presents research only on specific patient groups. However, as the person in need may have equal limitations of functioning no matter what their diagnosis, there are a number of characteristics from MTC that can be generalized to other groups of patients.
The authors of the review on multiple sclerosis discuss the issue of applying the RCT design on assessment of MTC in rehabilitation. It is questioned whether the evidence base for effectiveness coming from clinical trials and outcomes research can be applied to assessment of outcomes in the context of rehabilitation.
There is a need for more RCTs in other patient groups. Whereas there are reviews on both in-patient and out-patient MTC rehabilitation programmes for a number of musculoskeletal disorders, there is a lack of reviews on conditions such as pulmonary diseases (COL) and different forms of cancer. As suggested by Groote, research within rehabilitation should address all dimensions of the ICF, and the WHO World Report on Disability includes work in multi-professional teams (36). Although the literature provides limited evidence concerning the key components of MTC, the theoretical basis of a multi-professional team is well described: agreed aims and shared understanding on how to best achieve these, an appropriate range of knowledge and skills, mutual trust and respect, willingness to share knowledge and expertise; and to speak openly (10).
Conclusion
Despite the variety of interventions and level of MTC, the literature demonstrates that MTC promotes the effects of rehabilitation compared with a control group or standard rehabilitative care in 10 of 12 patient groups. There is not 1 single MTC method, but some general characteristics of MTC in rehabilitation of different patient groups are presented.
References


