Jarno Gauffin1, Tiina Hankama2, Pekka Hannonen2,5, Hannu Kautiainen3,4, Timo Pohjolainen1 and Maija Haanpää6,7
From the 1ORTON Rehabilitation Centre, ORTON Foundation, Helsinki, 2Department of Medicine, Central Hospital Jyväskylä, 3Unit of Family Practice, Central Finland Central Hospital, Jyväskylä, 4Unit of Primary Health Care, Kuopio University Hospital, 5University of Eastern Finland, School of Medicine, Kuopio, 6Etera Mutual Pension Insurance Co. and 7Department of Neurosurgery, Helsinki University Central Hospital, Helsinki, Finland
OBJECTIVE: The aim of this study was to examine the types of pain management strategies used by patients with fibromyalgia.
METHODS: A total of 158 patients with primary fibromyalgia attended a clinical visit to confirm the diagnosis. They completed 3 questionnaires: (i) a self-made questionnaire, (ii) Beck Depression Inventory IA (BDI IA), and (iii) Finnish version of Fibromyalgia Impact Questionnaire. The self-made questionnaire included questions about: intensity of current pain; general well-being; pain management strategies, including pain medications; efficacy of the pain management methods; current health problems other than fibromyalgia. The pain management strategies were subcategorized (e.g. physical exercise, massage and heat treatment). The strategies were also divided into active and passive types.
RESULTS: The most frequently reported pain management strategies were physical exercise (54%), physical therapy (32%) and cold treatment (27%). The use of active pain management strategies, BDI IA < 10 points and age were independent predictors of the reported pain management efficacy. Patients who used active pain management strategies reported better efficacy with the BDI IA score ≥ 10 points.
CONCLUSION: Active pain management strategies are most efficacious for fibromyalgia patients, regardless of the severity of fibromyalgia or optional comorbid depression.
Key words: fibromyalgia; pain; management; activity.
J Rehabil Med 2013; 45: 00–00
Correspondence address: Jarno Gauffin, Tenholantie 10, FI-00280 Helsinki Finland. E-mail: jarno.gauffin@gmail.com
Accepted Dec 14, 2012; Epub ahead of print 26, 2013
INTRODUCTION
Fibromyalgia (FM) is a chronic pain syndrome that affects up to 5% of the general population world wide (1). Characteristic features of FM are widespread musculoskeletal pain, tenderness and fatigue in the absence of any explanatory organic disease (2). Other common symptoms are disturbed and unrefreshing sleep, cognitive problems and a variety of psychosomatic symptoms originating from various organs (3). The aetiology of FM is obscure, although recent studies have shown that central pain processing plays a pivotal role in its pathogenesis (4). Impediments caused by FM are heterogeneous, and treatment approaches should be individually planned (5). The pharmacotherapy of FM relies on tricyclic antidepressants (TCAs), serotonin-noradrenaline reuptake inhibitors (SNRIs) and gabapentinoids (6). Non-pharmacological treatments are also important considering the diverse nature of FM and the common intolerance to pharmaceuticals displayed by patients with FM (7). European Leauge Against Rheumatism has recommended heated pool therapy, with or without exercise, as a non-pharmacological treatment for patients with FM. The recommendations also note that individually tailored exercise programmes, including aerobic and strength training, cognitive behavioural therapy, relaxation-therapy, physical therapy and physiological support, may be beneficial for patients with FM (8). A multidisciplinary approach was found to be more effective than mono-disciplinary treatment at the post-treatment evaluation (9). However, Finnish FM-specific multidisciplinary rehabilitation programmes did not have better efficacy than non-specific musculoskeletal programmes regarding the maintenance of working capacity (10). The lack of FM-specific diagnostic laboratory tests or imaging options (11), the severe burden caused to the patients and society (12) and the absence of long-term evidence of treatment efficacy (5, 13, 14) creates a demand to understand what kind of symptom management strategies are useful for patients with FM in their daily lives.
The objective of this study was to examine what kind of pain management strategies patients with FM use and the appropriate predictors of the efficacy of those strategies.
Patients and methods
Patients
Participants for the study were recruited from the patients with primary FM who had been diagnosed and treated in outpatient departments of rheumatology or physical medicine and rehabilitation of Jyväskylä Central Hospital between 2006 and 2008. Patients were identified using the International Classification of Diseases-10 code M79.0 according to the 2006 version. Based on medical records, patients with active inflammatory arthritis, systemic connective tissue disease, cognitive impairment, severe psychiatric disorders or any other unstable disease (e.g. cancer) were excluded. Only patients aged > 18 years were included.
Data collection
The questionnaires and consent form were sent to all traceable patients in January 2009. The patients were asked to complete 3 questionnaires: (i) a self-made questionnaire, (ii) Beck Depression Inventory IA (BDI IA) (15, 16), and (iii) the Finnish version of the Fibromyalgia Impact Questionnaire (Finn-FIQ) (17, 18).
The study protocol was approved by the Committee of Research Ethics of Central Finland Health Care District, and the patients gave their written consent.
The self-made questionnaire (consisting of 15 questions) included questions regarding the intensity of the current pain, general well-being of the patient, pain management strategies used by the patients, including pain medications and non-pharmacological ways to control pain, and the efficacy of the pain management methods. Furthermore, the questionnaire inquired about current health problems other than FM. The intensity of perceived current pain and general well-being were assessed with visual analogue scales (0–100 mm), while a numerical rating scale from 0 to 10 (10 meaning the best possible efficacy) was applied when assessing the efficacy of pain management strategies.
Regarding pain management strategies, the patients were asked in an open question to name the strategies. There was no restriction in the number of strategies. The pain management strategies were categorized by the authors into 9 different types: (1) physical exercise, (2) physical therapy, (3) cold treatment, (4) massage, (5) complementary and alternative medicine, (6) rest, (7) heat treatment, (8) relaxation exercise, and (9) other activities intended to direct attention away from the pain.
The pain management strategies were divided into active and passive types of strategies. Physical exercise, relaxation exercise and other activities to direct attention elsewhere from pain were regarded as active types because they required the patient’s activity to initiate and carry on the pain management. Other strategies were categorized as passive types.
BDI IA is a 21-item questionnaire to assess possible depression. The questionnaire has been validated in Finnish (16). A cut-off score of 10 was selected to determine clinical depression.
Finn-FIQ is a multidimensional self-administered questionnaire including 10 questions that evaluate physical functioning, work status, depression, anxiety, sleep, pain, stiffness, fatigue and well-being and has been validated in Finnish (18). The total score of Finn-FIQ is the sum of 10 sub-scores ranging from 0 to 100 is most impaired functioning (where 0 is unimpaired physical functioning).
Those subjects who replied were invited to a clinical visit, where an experienced physician (TH) examined the patients and confirmed the diagnosis of FM according to the classification criteria of the American College of Rheumatology (19).
Statistical methods
The data are presented as means with standard deviations (SD), medians with interquartile ranges (IQR) or counts with percentages. Statistical comparison between groups was made with the Fisher-Pitman permutation test for two samples, χ2 test or Cochran-Armitage Trend Test, when appropriate. Robust regression analyses were used to identify the appropriate predictors of the efficacy of pain management strategies using standardized regression coefficients (beta). Robust regression is an alternative to least squares regression when data is contaminated with outliers or influential observations, and it can also be used for the purpose of detecting influential observations. Standardized regression coefficients value is a measure of how strongly each predictor variable influences the criterion (dependent) variable. The beta is measured in units of SD. Bootstrap-based multiplicity adjustment is applied to correct the levels of significance for multiple testing when appropriate.
RESULTS
The postal survey was sent to 239 patients with primary FM, and 169 patients (71%) replied. There was no significant age or gender distribution difference between the respondents and non-respondents. Five patients declined to attend the clinical visit due to long distances. Six patients had completed questionnaires insufficiently and were excluded from the analyses. Hence, 158 patients who had undergone clinical evaluation and had completed the questionnaires adequately were included in the analyses. Clinical and demographic data for these patients are shown in Table I.
Table I. Demographic and clinical characteristics of 158 patients with fibromyalgia (FM) | |
Variables | Demographic and clinical data, n = 158 |
Female, n (%) | 149 (94) |
Age, years, mean (SD) | 47 (11) |
Duration of FM, years, median (IQR) | 3 (6) |
FIQ total score, mean (SD) | 49 (20) |
Body mass index, mean (SD) | 28.1 (6.6) |
Efficacy of pain management, NRS, mean (SD) | 7 (2) |
Pain VAS, mm, mean (SD) | 54 (23) |
General well-being VAS, mm, mean (SD) | 48 (22) |
Beck Depression Inventory, mean (SD) | 14 (9) |
Other disorders, n (%) | |
Musculoskeletal and associated disorders | 62 (39) |
Cardiovascular disorders | 32 (20) |
Psychiatric disorders | 18 (11) |
Endocrinological disorders | 13 (8) |
Neurological disorders | 1 (1) |
Pulmonary disorders | 40 (25) |
Regular use of pain medication, n (%) | 92 (58) |
Use of medication recommended for FM, n (%) | 66 (42) |
Inpatient rehabilitation, n (%) | 31 (20) |
NRS: numerical rating scale; SD: standard deviation; VAS: visual analogue scale; IQR: interquartile range. | |
The most frequently reported pain management strategies were physical exercise (54%), physical therapy (32%) and cold treatment (27%). Pain management strategies, as divided into tertiles according to Finn-FIQ total score, are presented in Fig. 1. No single pain management strategy showed statistically significant linearity after multiple corrections. Fifty-nine percent reported usage of active pain management strategies.
The use of active pain management strategies, lack of depression (BDI IA less than 10 points) and age were independent predictors of the efficacy of the pain management strategies (Table II).
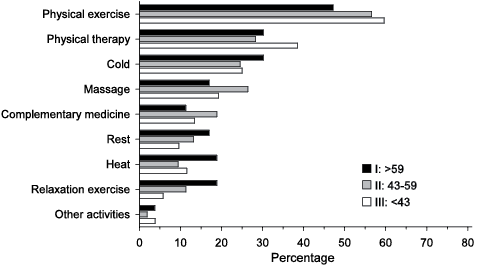
Fig. 1. Percentage distribution of the pain management strategies as divided into tertiles according to Finnish version of Fibromyalgia Impact Questionnaire total score.
|
Table II. Standardized beta coefficients with 95% confidence intervals for multiple robust regression analysis of the efficacy of the pain management strategies |
||
|
Variable |
Beta (95% CI)a |
p-value |
|
Active pain management strategy |
0.20 (0.04 to 0.37) |
0.017 |
|
BDI IA ≥ 10 |
–0.21 (–0.40 to –0.03) |
0.026 |
|
Age |
–0.20 (–0.38 to –0.03) |
0.022 |
|
Male |
0.08 (–0.08 to 0.24) |
0.31 |
|
Duration of FM |
0.05 (–0.12 to 0.22) |
0.54 |
|
BMI |
0.05 (–0.12 to 0.23) |
0.55 |
|
Finn-FIQ total score |
–0.13 (–0.32 to 0.05) |
0.16 |
|
Regular use of pain medication |
–0.06 (–0.27 to 0.15) |
0.57 |
|
Use of medication recommended for FM |
0.15 (–0.06 to 0.35) |
0.15 |
|
Other musculoskeletal disorders |
0.04 (–0.13 to 0.21) |
0.64 |
|
Cardiovascular disorders |
–0.02 (–0.19 to 0.15) |
0.83 |
|
Endocrinological disorders |
–0.04 (–0.21 to 0.13) |
0.66 |
|
Pulmonary disorders |
–0.13 (–0.29 to 0.04) |
0.12 |
|
aStandardized regression coefficient. FM: fibromyalgia; BDI IA: Beck Depression Inventory IA; BMI: body mass index; CI: confidence interval; Finn-FIQ: Finnish version of Fibromyalgia Impact Questionnaire. |
||
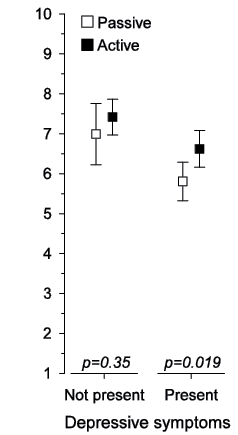
Even with the BDI IA score ≥ 10 points, patients who used active pain management strategies reported better efficacy of their pain management than the other cases (Fig. 2).
Fig. 2. Age-adjusted efficacy of the pain management with 95% confidence interval (95% CI) according to depressive symptoms in active and passive pain management strategies.
DISCUSSION
Our main finding was that active pain management strategies are the most beneficial. Physical exercise and relaxation exercise are at the opposite ends of the activity, but the crucial feature they have in common is an active subject, who relies on his or her self-management. Recent recommendations for physical exercises are focused on enhancing physical condition (20), but patient’s self-confidence to manage painful symptoms themselves seems to be at least as important. An active role of the patient is also true when he or she consciously uses other activities to direct attention elsewhere from pain. When those 3 active methods (physical exercise, relaxation and other activities to direct attention elsewhere from pain) are compared, for example, with heat or cold treatments (where the physical variable is active and the patient is passive after first initiation), they require activity throughout the process. Patients who are active entire pain management process appear to have a better impression of dealing with the pain in their own terms. Outsourcing of management usually takes place when physical therapy or alternative and complementary medicine are applied as a pain management strategy. The role of the therapist overrides self-management and unintentionally inactivates the patients. This may explain the lack of long-term efficacy of physical therapy in previous studies (5, 13, 15). However, patients need guidance to learn how to use active pain management strategies. A multidisciplinary approach, which has been shown to be most effective, provides the best option to reach the target of fewer symptoms (9).
A further important result was that, even mild clinical depression (BDI IA ≥ 10), decrease the efficacy of the symptom management, but the benefits of the active type of strategies remain statistically significant. Thus, it is very important to identify depressive symptoms in the patients with FM and treat depression effectively. Patients should also be encouraged to use active symptom management strategies regardless of whether depressive symptoms are present. Furthermore, we emphasize the selection of active exercises according to each patient’s current resources.
Lack of linearity in any single pain management strategy according to Finn-FIQ total score tertiles showed that patients with all levels of functioning chose to use pain management strategies included in all 9 reported categories. The level of functioning did not predict what kinds of strategies were used. This heterogeneity is important to recognize when individual pain management strategies are tailored. Some patients whose functioning is severely affected by FM can benefit from even rigorous exercises, whereas other patients with better functioning may prefer less strenuous ones. From that perspective, healthcare professionals who treat patients with FM should not only be supportive, but also responsive to patients’ history and wishes to ensure that the most opportune rehabilitation measures are adopted.
It is also a noteworthy finding that either other health problems (with the exception of depressive symptoms) or pain medication (use of any pain medication or use of medication recommended for FM, e.g. gabapentinoids, TCAs or SNRIs) did not predict the efficacy of the pain management strategies. Of course, other health problems have to be taken into account when individual pain management strategies are planned, but they did not alter the efficacy of the active types of strategies. In an individual FM patient, pain should be treated as effectively as possible, but pain medication should be regarded as an adjunct to active pain management strategies.
In general, our cohort represented patients with FM well, as Jyväskylä Central Hospital is the only hospital with rheumatology and physical medicine and rehabilitation services receiving referrals from an area with a population of 270,000. Compared with the cohorts used in randomized controlled drug trials for FM, our sample is most probably closer to a “real life” population. We also made a point of including male patients. Therefore, our study gives a good general view of the real-life management strategies. However, our study sample was recruited by postal survey, which may decrease the representativeness of the sample. This should be kept in mind when considering the results obtained. It should also be noted that we did not test our own questionnaire before the study. Therefore, studies with other cohorts investigating patients with FM pain management strategies are needed. We also acknowledge that we did not use existing questionnaires measuring pain coping, e.g. Chronic Pain Coping Inventory (21). The use of a validated questionnaire is recommended for future studies.
Our “real-life” population of patients with FM was found to consist of active people who were interested in their well-being. They used those pain management strategies that were available to them and tried to cope with their pain as well as they could. This is in contrast to the general prejudice regarding patients with FM as passive and non-compliant patients (22). It is our job as healthcare professionals to direct patients towards those strategies that are the most beneficial and at the same time to look for and treat comorbidities, such as depression.
In conclusion, active pain management strategies have the best efficacy regardless of the severity of FM or optional comorbid depression. Patients with FM should be encouraged and properly instructed to use active pain management strategies to improve their well-being.
ACKNOWLEDGEMENTS
The study received financial support from the research funds of Rehabilitation Orton and the Social Insurance Institute of Finland. We appreciate their support for this study.
The authors declare no conflicts of interest.
References

