Karl S. Bagraith, BOccThy(Hons)1,2, Julia Hayes, BOccThy(Hons)2 and Jenny Strong, PhD2
From the 1Occupational Therapy Department, Neurosurgical/Orthopaedic Physiotherapy Screening Clinic &
Multidisciplinary Service and the Centre for Allied Health Research, Royal Brisbane and Women’s Hospital, and
2Division of Occupational Therapy, School of Health & Rehabilitation Sciences, The University of Queensland,
Brisbane, Australia
OBJECTIVE: To determine whether the International Classification of Functioning, Disability and Health (ICF) Low Back Pain Core Sets are sufficient to cover the activity and participation goals that patients prioritize when commencing multidisciplinary rehabilitation.
DESIGN: Prospective multi-site cross-sectional questionnaire study.
SUBJECTS: Patients with chronic low back pain attending multidisciplinary outpatient clinics at two metropolitan hospitals in Australia.
METHODS: Participants used the Patient Specific Functional Scale to record goals when commencing rehabilitation. Two raters employed a standardized procedure to extract and link goal concepts to the ICF. A description exploration was undertaken with reference to the low back pain Core Sets. Sample size was determined via saturation.
RESULTS: Saturation was achieved with 33 participants.
Ninety-five goals were identified, from which 109 concepts were extracted. All of the concepts could be linked to the ICF, spanning 23 2nd-level categories. The comprehensive and brief core sets encompassed 95% and 65% of the concepts respectively. Maintaining body position (d415), doing housework (d640), changing basic body position (d410) and walking (d450) accounted for the majority (50.5%) of goals.
CONCLUSION: This study confirms the content validity of the low back pain Core Sets from the patients’ perspective. The Core Sets are likely to have good clinical utility, however, additional research is required to substantiate whether ratings of ICF based goals can be used to measure goal achievement.
Key words: International Classification of Functioning, Disability and Health; ICF; Core Sets; low back pain; goals.
J Rehabil Med 2013; 45: 00–00
Correspondence address: Karl Bagraith, Occupational Therapy Department, Level 2, JMB, Royal Brisbane and Women’s Hospital, Butterfield St, Herston, QLD, Australia, 4029. E-mail: karl.bagraith@gmail.com
Accepted Dec 19, 2012; Epub ahead of print Mar 27, 2013
INTRODUCTION
Non-specific chronic low back pain (CLBP) is one of the most common and costly health conditions in the industrialized world (1). Comprehensive multidisciplinary rehabilitation is consistently recommended as the foremost treatment approach for individuals seeking tertiary care for this condition (2). Pain rehabilitation typically consists of a cyclic process of assessment, treatment and evaluation; in what Steiner et al. (3) have termed the Rehab-Cycle. Patient-generated goals play a key role in guiding rehabilitation and serve to enhance engagement throughout the cycle (4). However, there is currently no single, standardized approach to formulating and monitoring patient goals (5).
The International Classification of Functioning, Disability and Health (ICF) provides the first internationally agreed upon framework to define health and health-related states (6). With its universal language the ICF has been proposed as an ideal framework to guide the rehabilitation cycle across conditions, health care disciplines, treatment settings and geographic regions (7). Recently, along with its qualifier scale, it has also been suggested as a useful tool to classify goals in multidisciplinary musculoskeletal rehabilitation (8, 9). The ICF is exhaustive and contains 1,454 categories covering body functions, body structures, activities and participation, and environmental factors (6). Therefore, in its entirety, the framework is impractical for application in routine clinical practice. To facilitate operationalization of the framework ICF Core Sets were developed for specific conditions and settings (10). Each Core Set provides a selection of the most salient categories for a given condition or setting, consisting of as few categories as practically possible, but as many as necessary to encompass the typical spectrum of function (10). Consequently, the Core Sets, in particular, have been proposed as practical ICF-based clinical tools to guide the rehabilitation cycle (11).
In 2004 the Comprehensive and Brief versions of the Low Back Pain (LBP) Core Set were released (12). The Comprehensive Core Set, with 78 categories, is intended for multidisciplinary practice, whereas, the Brief version contains a sub-selection of 35 categories that can guide uni-professional encounters. The selection of LBP Core Sets categories was made via a formal decision making and consensus process that considered evidence from expert consultation, a systematic literature review and empirical data collection (12). However, to date clinical practice implementation of the ICF, and associated LBP core sets, has been reported to be minimal, despite the advantages that their use may afford patients and practitioners alike (13).
The ICF LBP Core Sets require further validation in diverse regions and settings, and especially from the patient perspective, to establish their content validity and support application in clinical practice. In particular, research is required to substantiate whether the LBP Core Sets are sufficiently comprehensive to reflect the tasks and actions that are important to patients and form the focus of their treatment (13, 14). If this condition is met, the Core Sets may serve as a universal tool, in and of themselves, to guide the development, monitoring and evaluation of patient-generated goals during multidisciplinary rehabilitation (9, 11). The current study was therefore designed to investigate whether the ICF LBP Core Sets were sufficient to cover the activities that patients with CLBP identify as difficult and prioritize as goals when commencing multidisciplinary rehabilitation.
METHODS
Overview
A cross-sectional questionnaire study was undertaken with a convenience sample of outpatients attending a multidisciplinary service at two major metropolitan hospitals in Brisbane, Australia. This multisite public hospital service provides conservative multidisciplinary allied health management of patients with chronic musculoskeletal conditions that are long-term waitlisted for medical specialist opinion. Patients are referred to the service by their general practitioner. As part of normal practice new patients to the service are posted a copy of the Patient Specific Functional Scale (PSFS) (15) just prior to their initial appointment. Patients are instructed to use the PSFS as a tool to document important activities to focus on during treatment. For eligible patients between June and September 2011 a study invitation letter and research packet (information and consent forms as well as additional demographic and functioning questionnaires (detailed below) was included with the PSPS. Participants who volunteered returned all completed materials to their health professional at their initial appointment. Responses to the PSFS were linked to the ICF and a descriptive exploration was undertaken with reference to the activity and participation component of ICF LBP Core Sets. The research team had no direct contact with participants. The study was granted ethical clearance by the relevant multi-site hospital (HREC/11/QPAH/08) and university (MREC/UQ/2011000604) ethics committees in accordance with the Declaration of Helsinki. Each participant provided written informed consent.
Participants
Patients were included in the study if non-specific LBP (16), as assessed by their specialized musculoskeletal physiotherapist during their initial appointment, was their main health condition. In addition, patients were only eligible if they were 18 years or older, able to read and write English, had no known cognitive deficits, and reported LBP of greater than 3 months duration.
Measures
Patient Specific Functional Scale (15). The PSFS, developed prior to the introduction of the ICF, is an individualized measure of disability that is commonly used in musculoskeletal practice and research (17). It asks respondents to list three important “activities” that they find difficult due to their specific health condition (in this case CLBP) and would like to focus on during their treatment. PSFS responses represent tasks and actions that are important to the individual and are in line with their expectations for treatment. Thus these responses are routinely used in clinical practice to direct treatment (17). In terms of the ICF, the activity and participation component of the classification most clearly encompass responses to the PSFS (18). In this regard, as others have (19), we deemed PSFS responses to be synonymous with the content of patient-generated treatment goals, more specifically activity and participation goals.
ICF Core Sets for LBP (12). The Comprehensive LBP Core Set contains a selection of 78 2nd-level ICF categories. Of these, 29 (37%) are from the activities and participation component of the ICF, covering general tasks and demands (1 category), mobility (11 categories), self-care (4 categories), domestic life (5 categories), interpersonal interactions and relationships and major life areas (3 categories each), and community, social and civic life (2 categories). The activities and participation component of the Brief Core Set consists of a sub-selection of 12 categories from the 29 that are included in the Comprehensive version. These 12 categories are similarly distributed across general tasks and demands (1 category), mobility (4 categories), self-care (2 categories), domestic life (1 category), interpersonal interactions and relationships (1 category) and major life areas (3 categories).
Other instruments. Finally, to describe the sample, participants also completed the Oswestry Disability Index v2.1a (ODI) (20), Kessler Scale of Psychological Distress (K10) (21) and Self-Administered Comorbidity Questionnaire (SCQ) (22). The ODI measures LBP related disability, the K10 is a screening tool for non-specific psychological distress and the SCQ records respondents presenting comorbidities. For each tool higher scores represent more of the quantified attribute.
Data analysis
Extracting concepts from patient goals. Goals were analysed according to the meaning condensation procedure described by Kvale (23). In brief, as the general application of the procedure for ICF linking has been illustrated elsewhere (24), this involved careful reading of PSFS responses to identify meaningful concepts from patients’ goals. Each goal could contain more than one concept. For example, a patient recorded “improving everyday maintenance of house and garden” which was broken down into two concepts: “household maintenance” and “garden maintenance”. PSFS responses were re-read several times to cross-check the extraction of meaningful concepts (25).
Linking concepts to the ICF. Established rules (26) were applied to link identified concepts to the ICF category that most precisely represented the concept. The ICF linking rules have been applied in over 37 studies to map health status instruments to the ICF (27), thus they are a widely applied quality control tool (25). A final year occupational therapy student (JH) and a senior pain occupational therapist (KB) undertook the linking with additional reference to a methodological guideline developed by the ICF Research Branch. Both raters completed ICF training and KB had previous experience applying the linking rules (28). Initially, multiple coding (24) was carried out by KB and JH with approximately one third of the goals to establish consensus on the extraction and linking of concepts for this data set. A third rater (JS) was available to resolve any disagreement, however, was not required. JH then independently analyzed the remaining goals followed by a peer review of one third of this data to examine inter-rater reliability. Percentage agreement and prevalence- and bias-adjusted kappa (PABAK) (29) were used to quantify inter-rater reliability. PABAK was selected due to the presence of Kappa’s first paradox (30). To enhance methodological rigor we employed research diaries and continuous data analysis in addition to the multiple coding and peer review triangulation strategies (25).
Absolute and relative frequencies were used to examine the distribution of linked categories with respect to the LBP Core Sets. The content validity of each Core Set category was considered to be supported if it encompassed at least one goal concept. As is typical, results are presented at the 2nd-level of the ICF to permit ready comparison with the LBP Core Sets (E.g. 8, 31, 32, 33). All analyses were performed with Microsoft Excel 2007 and SPSS Version 19.0 for Windows.
Sample size. Sample size was determined by saturation, which refers to the point where no additional new information is obtained from the data (25). When a-priori saturation rules have been used to iteratively determine sample size in qualitative ICF linking studies, two definitions have typically been employed that focus on the 2nd-level of the classification (27). Firstly, when two consecutive ‘units’ revealed no new categories and, secondly, when two consecutive ‘units’ revealed fewer than 5% new categories, with respect to the categories that have already been linked. The ‘units’ in these studies have usually been focus groups and individual interviews, with saturation generally reached after 5 focus groups and 9 to 12 individual interviews (27, 34). However, unlike focus groups or interviews, we were unlikely to obtain the same richness of qualitative information from each participant due to the structure and specificity of our data collection method, a written questionnaire. Therefore, in this study, saturation was conservatively defined as the point when goal concepts from 10 consecutive participants revealed no new linked 2nd-level ICF category.
RESULTS
Thirty-five eligible patients consented to participate in the study. Two participants were removed during the analysis as they did not complete the PSFS. As can be seen from Fig. 1, saturation was reached with 33 participants. Accordingly, the results presented below pertain to those 33 participants.
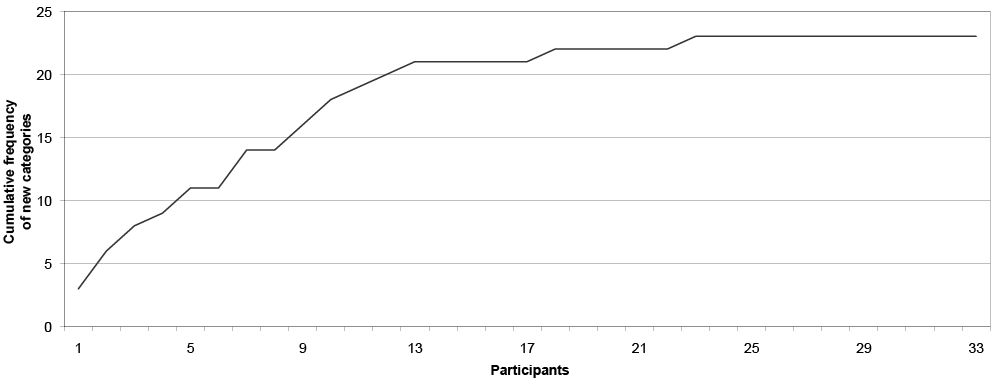
Fig 1. Accumulation of linked 2nd level International Classification of Functioning, Disability and Health (ICF) categories from consecutive participants’ goals. Saturation was achieved with the questionnaire responses from 33 participants; which were linked to 23 different ICF categories.
Patient characteristics
Tables I and II provide participant demographic details and self-reported health status respectively. The sample was comprised of similar numbers of males (n = 15) and females (n = 18) and the participants were on average 58.7 years old (standard devaition [SD] 13.8). The length of time participants had experienced pain ranged from 8 months–44 years (SD 157.3 months). Twenty-seven percent of participants were currently employed (full- or part-time) and just over half (60.6%) rated their general health as at least “good”. According to the K10 and ODI, 60.6% of patients were likely to have at least mild symptoms of psychological distress (total score ≥ 40) and, 63.6% had at least severe pain-related physical disability (total score ≥ 40) respectively.
|
Table I. Demographic variables (n = 33) |
|
|
Variable |
|
|
Gender, n (%) |
|
|
Male |
18 (54.5) |
|
Female |
15 (45.5) |
|
Age, years, mean (SD) |
58.7 (13.8) |
|
Pain duration, months, mean (SD) |
133.6 (157.3) |
|
Marital status, n (%) |
|
|
Single |
1 (3.0) |
|
Married |
19 (57.6) |
|
Separated |
1 (3.0) |
|
Divorced |
8 (24.2) |
|
Windowed |
3 (9.1) |
|
Defacto/stable relationship |
1 (3.0) |
|
Education, n (%) |
|
|
Primary school |
8 (24.2) |
|
Junior high school certificate |
10 (30.3) |
|
Senior high school certificate |
5 (15.2) |
|
Tertiary non-university |
6 (18.2) |
|
Tertiary university |
4 (12.1) |
|
Employment status, n (%) |
|
|
Full-time |
6 (18.2) |
|
Part-time |
3 (9.1) |
|
Retired |
14 (42.4) |
|
Home duties |
4 (12.1) |
|
Unemployed due to pain |
6 (18.2) |
|
SD: standard deviation. |
|
|
Table II. Self-reported health status (n = 33) |
|
|
Variable (scale range) |
|
|
Pain intensity (0–10)1, mean (SD) |
6.8 (1.6) |
|
Kessler scale of psychological distress (10–50), mean (SD) |
23.2 (8.6) |
|
Oswestry disability index (0–100), mean (SD) |
45.8 (13.6) |
|
Overall function (0–10)2, mean (SD) |
4.0 (1.7) |
|
Self-Administered Comorbidity Questionnaire, mean (SD) |
2.9 (2.0) |
|
General health, n (%) |
|
|
Excellent |
1 (3.0) |
|
Very good |
5 (15.2) |
|
Good |
14 (42.4) |
|
Fair |
9 (27.3) |
|
Poor |
4 (12.1) |
|
111-point numerical rating scale (0 = no pain, 10 = pain as bad as you can imagine). 211-point numerical rating scale (0 = complete limitation in all aspects of functioning, 10 = no limitation) (8, 31). SD: standard deviation. |
|
Linking activity goals to the ICF
In total 95 goals were reported, with one participant only proving 2 responses to the PSFS. A total of 109 concepts were extracted from these goals, each of which could be linked to an ICF category. Almost all (96%) of the concepts were linked to the activities and participation component. As can be seen from Tables III and IV, concepts were linked to 23 different 2nd-level ICF categories from 7 different chapters – mental functions (b1), sensory functions and pain (b2), mobility (d4), self-care (d5), domestic life (d6) interpersonal interactions and relationships (d7) and community, social and civic life (d9).
Of the 109 identified goal concepts, 95.4% were linked to categories contained in the Comprehensive LBP Core Set, and 65.1% to Brief LBP Core Set categories. Goals were most frequently focused of the following tasks and actions: maintaining body position (d415) (15.6%), doing housework (d640) (14.7%), changing basic body position (d410) (11.0%) and walking (d450) (9.2%). Doing housework (d640) was the most frequently reported within patients’ first goal, whilst maintaining body position (d415) and changing basic body position (d410) were most frequently reported within their second and third goals respectively. Goals frequently identified by patients that were not included in the Brief LBP Core Set were driving (d475) and caring for household objects (d650). Table IV displays the allocation of the 5 concepts (4.6%) that were linked to non-LBP Core Set categories; these being: sensations associated with hearing and vestibular function (b240), grasping (d440) and caring for body parts (d520).
|
Table III. International Classification of Functioning, Disability and Health (ICF) linkable goal concepts that were covered in the low back pain Core Sets1 (n = 33) |
|||||
|
ICF Code |
ICF Category label |
PSPS goal 1 frequency (%2) |
PSPS goal 2 frequency (%2) |
PSPS goal 3 frequency (%2) |
Total frequency (%2) |
|
d410 |
Changing basic body position |
2 (1.8) |
3 (2.8) |
7 (6.4) |
12 (11.0) |
|
d415 |
Maintaining body position |
5 (4.6) |
9 (8.3) |
3 (2.8) |
17 (15.6) |
|
d420 |
Transferring oneself |
0 (0.0) |
0 (0.0) |
1 (0.9) |
1 (0.9) |
|
d430 |
Lifting and carrying objects |
1 (0.9) |
3 (2.8) |
4 (3.7) |
8 (7.3) |
|
d445 |
Hand and arm use |
1 (0.9) |
0 (0.0) |
0 (0.0) |
1 (0.9) |
|
d450 |
Walking |
6 (5.5) |
3 (2.8) |
1 (0.9) |
10 (9.2) |
|
d455 |
Moving around |
1 (0.9) |
2 (1.8) |
1 (0.9) |
4 (3.7) |
|
d470 |
Using transportation |
0 (0.0) |
1 (0.9) |
2 (1.8) |
3 (2.8) |
|
d475 |
Driving |
5 (4.6) |
2 (1.8) |
1 (0.9) |
8 (7.3) |
|
d510 |
Washing oneself |
1 (0.9) |
1 (0.9) |
0 (0.0) |
2 (1.8) |
|
d530 |
Toileting |
0 (0.0) |
1 (0.9) |
1 (0.9) |
2 (1.8) |
|
d540 |
Dressing |
1 (0.9) |
1 (0.9) |
0 (0.0) |
2 (1.8) |
|
d570 |
Looking after one’s health |
1 (0.9) |
0 (0.0) |
2 (1.8) |
3 (2.8) |
|
d620 |
Acquisition of goods and services |
0 (0.0) |
0 (0.0) |
3 (2.8) |
3 (2.8) |
|
d640 |
Doing housework |
8 (7.3) |
5 (4.6) |
3 (2.8) |
16 (14.7) |
|
d650 |
Caring for household objects |
3 (2.8) |
2 (1.8) |
1 (0.9) |
6 (5.5) |
|
d760 |
Family relationships |
0 (0.0) |
2 (1.8) |
0 (0.0) |
2 (1.8) |
|
d920 |
Recreation and leisure |
0 (0.0) |
0 (0.0) |
2 (1.8) |
2 (1.8) |
|
b134 |
Sleep functions |
0 (0.0) |
0 (0.0) |
1 (0.9) |
1 (0.9) |
|
b280 |
Sensation of pain |
0 (0.0) |
0 (0.0) |
1 (0.9) |
1 (0.9) |
|
1Brief ICF Core Set categories are in bold. 2Percentage of the 109 total extracted concepts. PSPS: Patient Specific Functional Scale. |
|||||
|
Table IV. International Classification of Functioning, Disability and Health (ICF) linkable goal concepts that were not covered in the low back pain Core Sets (n = 33) |
|||||
|
ICF Code |
ICF Category label |
PSPS goal 1 frequency (%1) |
PSPS goal 2 frequency (%1) |
PSPS goal 3 frequency (%1) |
Total frequency (%1) |
|
b240 |
Sensations associated with hearing and vestibular function |
1 (0.9) |
0 (0.0) |
1 (0.9) |
2 (1.8) |
|
d440 |
Grasping |
0 (0.0) |
0 (0.0) |
1 (0.9) |
1 (0.9) |
|
d520 |
Caring for body parts |
1 (0.9) |
1 (0.9) |
0 (0.0) |
2 (1.8) |
|
1Percentage of the 109 total extracted concepts. PSPS: Patient Specific Functional Scale. |
|||||
Inter rater reliability
Percentage agreement for the peer review was 82.1 and PABAK was 0.64, suggesting moderate to substantial inter-rater reliability (30). This result is consistent with that of previous ICF linking studies which have reported inter-rater reliability (27).
DISCUSSION
In this study we sought to examine CLBP patients’ goals and their relation to the ICF. The results firstly confirm the usefulness of the ICF framework for describing and categorizing patient-generated goals in a standardized and meaningful way (8, 9, 31). Secondly, the findings reveal that the LBP Core Sets are sufficiently comprehensive to cover patient-generated activity and participation goals. Accordingly, this study substantiates the content validity of the activity and participation component of the LBP Core Set from the perspective of patients with non-specific CLBP attending multidisciplinary rehabilitation. It also provides evidence to support the clinical utility of the Comprehensive Core Sets as a tool to specify activity and participation goals during the rehabilitation cycle. Furthermore, the results suggest that the Brief Core Set may serve as a useful tool in uni-professional practice and, when used as a minimum data set, is likely to capture most of the activity and participation outcomes that are meaningful to patients.
Our results are most closely aligned with those of a recent study by Fairbairn et al. (18) which also mapped LBP patients’ PSFS responses to the ICF. However, there are important differences that warrant consideration before contrasting the results. We employed a prospective design that focused on patients with non-specific CLBP attending a public multidisciplinary service. Fairbairn et al. (18) used a retrospective file audit with an arbitrary sample size to examine heterogeneous musculoskeletal patients attending physiotherapy teaching clinics; the majority being university staff and students whose management was typically funded under an insurance scheme (23% having LBP of unspecified duration). In addition, we made explicit comparisons to the LBP Core Set categories, whereas Fairbairn et al. (18) only described responses, mostly at the component level of the framework. Accordingly, only general comparisons can be made. Fairbairn et al’s. (18) primary finding was that, according to the ICF, the PSFS is chiefly a measure of activity and participation (92% of LBP responses were linked to this component). With a comparable result (96% of responses), our findings substantiate that the PSFS almost exclusively measures activities and participation in people with LBP.
Currently there is limited qualitative research that has specifically examined the content validity of the LBP Core Sets from the patients’ perspective. When placing our results in the context of such research, two European studies are of particular relevance. First, using a questionnaire, Mullis et al. (32) revealed maintaining and changing body position as tasks that also pose significant problems for patients with acute and sub-acute LBP. Second, Abbott et al. (33), who used semi-structured interviews to retrospectively elicit CLBP patients’ problems before undergoing lumbar surgery. Consistent with our results maintaining body position and walking were frequently identified as problematic. In contrast to this study, where only a small proportion of patients identified recreation and leisure (d920) goals, these two studies highlighted the importance that people with LBP place on recreational pursuits. This disparity may be due to the approach used to obtain responses, as question phrasing is likely of significance. For example, Mullis et al. (32) found that patients did not report their most difficult activity as recreational, yet when asked about an activity they were unable to enjoy, recreation and leisure comprised 54% of responses. Moreover, caring for household objects (d650) and driving (d475), were common goals for patients in this study and warrant further consideration for inclusion in the Brief Core Set.
Whilst there are 3 categories related to employment in both versions of the LBP Core Sets, no participant identified work goals in this study. Conversely, Abbott et al. (33) identified remunerative employment (d850) as the most frequently restricted area for patients undergoing LBP surgery. Similarly, when health professionals apply the LBP Core Sets to classify patient problems they typically rate employment categories as mildly-severely restricted (35, 36). Likewise, in qualitative studies physiotherapists and doctors have reported work as an important goal for their treatment (37, 38). This difference may reflect the characteristics of our sample, as the majority were retired (42.4%). Thus, work was not a focus for many of our participants and, for those in the workforce (27.3%), it may not have been prioritized as an immediate goal for treatment. Further qualitative research targeting workers with CLBP would be useful to justify the inclusion of all 3 work categories in both Core Sets, particularly given their overlapping content and, especially for the Brief Core Set, need for brevity.
This study focused on patient-generated goals and their relation to the LBP Core Sets. To date the research examining ICF Core Sets as tools to specify goals has been confined to the acute and post-acute settings, and accordingly, focused on the acute and early post-acute Core Sets. Nonetheless, in patients with heterogeneous musculoskeletal conditions receiving acute and post-acute rehabilitation, the majority of patient goals have been attributable to activities and participation (8, 31). Suggesting that, irrespective of the setting (acute, post-acute or chronic), patients with musculoskeletal conditions tend to prioritize activities and participation, and in particular mobility, as important for treatment outcomes. However, in contrast to the present study where 95% of patient goals were contained in the LBP Core Set, only 65% and 68% of goals were contained in the acute and post-acute musculoskeletal conditions core sets respectively (8, 31). Thus ICF Core Sets may have greater relevance as tools to specify and evaluate goals in chronic conditions.
In the present study we restricted our consideration to content validity. We cannot comment on other aspects of construct validation or clinical utility. Of importance, before recommending the LBP Core Sets as a tool to also evaluate goal attainment, further research is required into the ICF qualifier scale. For example, poor inter-rater reliability for ICF category ratings, such as those for the LBP Core Set (39), has been a source of criticism for the operationalization of Core Sets in clinical practice (40). However, recent work has suggested that reliability may approach levels required for clinical practice when the qualifier levels are reduced and additional definition is provided for each graduation (41).
This study has some limitations that warrant consideration and reveal directions for future research. First, in using the PSFS we intended to collect data related to the activities and participation component of the ICF. People with chronic pain consider this functional area to be of great importance (42) and, even in the acute setting, the majority of musculoskeletal patient goals are focused on activities and participation (8, 31). Nonetheless, further research into patient goals from the remaining ICF components is necessary for comprehensive validation of the LBP Core Sets. Second, there can be discrepancies between patients’ and professionals’ perceptions of functioning and treatment goals (43). Therefore, we would recommend additional research to substantiate whether multidisciplinary professionals’ goals and assessments (28) are contained in the LBP Core Sets. Third, it could be suggested that PSFS responses may not represent traditional ‘goals’ (i.e. specific, measurable, achievable, relevant and time-based goals (4). However, our approach is consistent with research that has considered patient identified “relevant aspects of functioning” to be synonymous with goals (8, 31). Thus we similarly feel justified in considering PSFS responses to be goals, because they too represented areas that were important to patients and were in line with their functioning desires and expectations concerning their treatment (8, 31). In fact, by using the PSFS, we were able to overcome goal specificity issues identified in such studies, which likely contributed to the present result of all goal concepts being ICF-linkable. Conversely, it is unknown whether the restriction to three specific goals and use of a structured tool, as compared to individual interviews for example, provided a complete account of participants’ goals. Fourth, the PSFS does not explicitly request respondents to list goals in order of importance. However, the participating clinics reported that in their experience patients do list responses in such an order, which is consistent with available theories concerning the way people form lists (44). Accordingly, whilst we can’t be certain that patients listed their goals in order of importance, in the absence of cognitive interviewing to support a contrary viewpoint, we feel that it is unlikely that they would have done so otherwise. Finally, as there are currently no Australian studies investigating goals of patients with CLBP using the ICF, our results add evidence to the cross-cultural validity of the LBP Core Sets. Additional content validation studies in different countries and settings would serve to strengthen the psychometric evidence base of the LBP Core Sets.
In conclusion, this study confirms the content validity of the LBP Core Set’s activity and participation component from the perspective of goals that CLBP patients have when commencing multidisciplinary rehabilitation. Adoption of the LBP Core Sets in clinical practice will permit specification of patient goals in a language that is common to each member of the multidisciplinary team, facilitating more integrated and effective patient care. Further research is required to establish whether patients and clinicians can produce reliable ratings of ICF based goals that can be used to measure functioning and goal accomplishment.
ACKNOWLEDGEMENTS
The authors are grateful to the clinicians and, in particular, the administration officers and therapy assistants, for their assistance with data collection. We appreciate the support provided by the Manager of each clinic (Darryl Lee and Louise Matthews) and the Assistant Program Manager for the statewide service (Maree Raymer). We are thankful for the materials provided by the ICF Research Branch in collaboration with the WHO FIC CC in Germany (at DIMDI). Funding support was provided by the Royal Brisbane and Women’s Hospital Foundation and the Allied Health Professions’ Office of Queensland (AHPOQ). The Foundation AHPOQ and ICF Research Branch did not provided input on any aspect of the study, manuscript preparation or submission. The authors declare no conflicts of interest.
REFERENCES

