Jorit Meesters, MSc1,2,3,5, Sofia Hagel, PhD4,5, Mari Klokkerud, MSc6, Inger Stovgaard, PT7, Ann Bremander, PhD8,9, Margreth Grotle, PhD10, Kim Hørslev-Petersen, PhD, MD7, Ingemar F. Petersson, PhD, MD4,5, Kåre Birger Hagen, PhD11, Winke Pont, PT2 and Thea Vliet Vlieland, PhD, MD2,3
From the 1Department of Rheumatology, 2Department of Orthopaedics, Rehabilitation Medicine & Physical Therapy, Leiden University Medical Center (LUMC), Leiden, 3Sophia Rehabilitation Center, The Hague, The Netherlands, 4Department of Clinical Sciences Lund, Section of Rheumatology, Lund University and Skane University Hospital, 5Department of Clinical Sciences in Lund, Orthopaedics, Lund University, Lund, Sweden, 6National Resource Centre for Rehabilitation in Rheumatology, Diakonhjemmet Hospital, Oslo, Norway, 7University of South Denmark, King Christian 10th, Hospital for Rheumatic Diseases, Graasten, Denmark, 8School of Business and Engineering, Department of Exercise Physiology, Biomechanics and Health, Halmstad University, Halmstad, 9Research and Development Center, Spenshult Hospital for Rheumatic Diseases, Oskarstrom, Sweden, 10FORMI (Communication Unit for Musculoskeletal Disorders), Oslo University Hospital, Ullevaal and 11Institute of Health and Society, University of Oslo, Oslo, Norway
OBJECTIVE: To make a cross-cultural comparison of the contents of rehabilitation goals of patients admitted for rehabilitation and to compare the contents with the comprehensive International Classification of Functioning, Disability and Health (ICF) Core Set for rheumatoid arthritis, by linking their contents to the ICF.
Patients: A random sample of 80 patients with rheumatoid arthritis was retrieved from rehabilitation clinics in 4 countries.
Methods: Rehabilitation goals were extracted from the medical records and linked to the ICF using standardized linking rules.
RESULTS: A total of 495 rehabilitation goals were identified and linked to 952 ICF codes, resulting in 151 unique ICF codes. Two-hundred and seventy-five (29%) of the 952 ICF codes were related to “Body Functions” (b-codes), 80 (8%) to “Body Structures” (s-codes), 419 (44%) to “Activities and Participation” (d-codes) and 178 (19%) to “Environmental Factors” (e-codes). Thirty-five of the 151 unique ICF codes (23%) were not in the comprehensive ICF Core Set for rheumatoid arthritis, whereas 23 of the ICF codes in this Core Set (24%) were not in the rehabilitation goals.
CONCLUSION: The goals set in a team rehabilitation setting for patients with rheumatoid arthritis are related to all ICF components, with “Activities and Participation” being the most frequently addressed. The contents of the goals are, to a considerable extent, covered by the comprehensive ICF Core Set for rheumatoid arthritis, but additional evaluation is required before the ICF Core Set is used as a rehabilitation tool in rheumatoid arthritis.
Key words: rehabilitation; rheumatoid arthritis; patient care team; patient care planning.
J Rehabil Med 2013; 45: 00–00
Correspondence address: J. J. L. Meesters, Leiden University Medical Center, Department of Rheumatology (C1-R), PO Box 9600, NL-2300 RC Leiden, The Netherlands. E-mail: J.J.L.Meesters@lumc.nl
Accepted Mar 14, 2013, Epub ahead of print Aug 8, 2013
INTRODUCTION
Despite important improvements in pharmacological care for patients with rheumatoid arthritis (RA), delivery of comprehensive multidisciplinary care in a rehabilitation setting may be required if treatment by single health professionals fails (1). Goal-setting is considered to be central to rehabilitation (2–4). A rehabilitation goal refers to an intended future state of functioning and therefore implies a change that is established by the planned actions of a rehabilitation team (5). Furthermore, a rehabilitation goal needs to be relevant, motivating and attainable. In addition, a goal must enable well-balanced planning and measurement/evaluation (6); therefore rehabilitation goals need to be specific, measurable, achievable, realistic/relevant and timed, i.e. meeting the criteria for “SMART” formulation (7). The goal-setting process is the formal process whereby a rehabilitation team, together with the patient and/or the family, formulate the rehabilitation goals (5). The importance of goal-setting specifically in the rehabilitation of patients with RA is generally recognized (8), and a number of rehabilitation tools supporting the process of goal-setting and the assessment of goal attainment have been evaluated in this patient group. These rehabilitation tools include the Rehabilitation Activities Profile (RAP) (9, 10), the Canadian Occupational Performance Measure (COPM) (11), and the World Health Organization Disability Assessment Schedule II (WHODAS II) (12, 13). Both the RAP and the WHODAS II are based on the International Classification of Functioning, Disability and Health (ICF) (14), which provides a framework for the description of health and health-related states. The use of the ICF in RA rehabilitation has been comprehensively described (15–18) and the ICF is generally accepted as a reference framework. In particular, the use of ICF Core Sets for RA in RA rehabilitation is advocated, as these concern those contents of the ICF that are most relevant for this specific patient group. A previous study on goals of physiotherapy interventions (19) has shown that linking treatment goals to the ICF is feasible. To our knowledge, no studies have comprehensively described the contents of the actual goals set in patients with RA by classifying them according to the ICF or ICF Core Sets for RA. Since the problems of patients with RA in need of rehabilitation as well as the goal-setting process may vary within and across countries, it is important to take various settings into account when undertaking the analyses. More insight into the goals set in clinical rehabilitation practice may help to improve the goal-setting process, with the ultimate aim of improving the quality of rehabilitation for patients with RA. Based on these insights the process of training professionals with respect to goal-setting and/or the development and implementation of practical tools can be enhanced if needed.
The aim of the present study was two-fold: (i) to make a cross-cultural comparison of the contents of goals set in the rehabilitation of patients with RA; and (ii) to compare the contents of the goals with the ICF Core Sets for RA by linking the contents to the ICF.
PATIENTS AND METHODS
Study design
This study was part of a larger, international, observational, multicentre study in which multidisciplinary team care for patients with rheumatic and musculoskeletal conditions was investigated, the Scandinavian Team Arthritis Register – European Team Initiative for Care (STAR-ETIC; www.star-etic.se). Each centre was responsible for its own data collection. All patients agreed to participate in the study by signing a written consent. Ethical approval was granted by medical ethics boards in Sweden, Norway and the Netherlands. The regional medical ethics committee of Southern Denmark was informed about the study, but advised that formal ethical approval was not required.
Subjects
For this goal-setting study, 497 adult patients in the STAR-ETIC database, meeting the 1987 American Rheumatism Association RA criteria (20) were eligible. One specialist centre was selected by the local investigators in each country, except for Norway where 2 specialist centres were selected in order to recruit at least 20 Norwegian subjects. Thereafter, 80 patients (20 per country) were randomly selected from 5 specialist centres in Denmark (Kong Christian 10th Hospital, University of Southern Denmark, n = 94 eligible patients), the Netherlands (Rheumatology Clinic Sole Mio, Department of Rheumatology, Leiden University Medical Center, n = 49), Norway (Vikersund Kurbad, Vikersund and Lillehammer Rheumatological Hospital, Lillehammer, n = 28) and Sweden (the Clinic of Rheumatology in Lund University Hospital of Skåne, n = 48). The randomization procedure involved assigning a number to each eligible patient from the selected sites, then randomizing the order using the random number generator in Microsoft Excel, and selecting the first 20 numbers from the list. The characteristics of the care process in the participating clinics are described in Table I.
|
Table I. Characteristics of the rehabilitation care structure in the 4 countries |
||||
|
Denmark |
Netherlands |
Norway |
Sweden |
|
|
Treatment |
||||
|
Individual treatment |
● |
● |
● |
● |
|
Group treatment |
● |
● |
● |
● |
|
Outpatient care/day care |
● |
● |
● |
● |
|
Inpatient care |
● |
– |
● |
– |
|
Fixed programme length |
– |
– |
– |
18 days |
|
Team |
||||
|
Rheumatologist |
● |
● |
● |
● |
|
Specialized nurse |
● |
● |
– |
– |
|
Nurse |
– |
– |
● |
– |
|
Assistant nurse |
– |
– |
– |
● |
|
Psychologist |
– |
– |
– |
– |
|
Occupational therapist |
● |
● |
● |
● |
|
Physical therapist |
● |
● |
● |
● |
|
Dietician |
● |
– |
– |
– |
|
Social worker |
● |
● |
– |
– |
|
Number of health professions in team |
n = 6 |
n = 5 |
n = 4 |
n = 4 |
|
Goal-setting |
||||
|
Maximum number of rehabilitation goals |
No limit |
No limit |
3 |
3 |
|
Goal assessment by patient in own words |
● |
– |
● |
● |
|
Goal assessment by rehabilitation tool |
– |
● |
– |
– |
Assessments
Sociodemographic and disease characteristics. At enrolment, data on subject’s sociodemographic and disease characteristics were collected using a questionnaire with items for age, gender, living status, educational level (12 years of education or more/less than 12 years), employment status (yes/no), comorbidities (yes/no), and current medication (oral corticosteroids, disease-modifying anti-rheumatic drugs (DMARDs) and/or biologicals).
The main assessments included:
• Activity limitation, as measured with the self-administered Health Assessment Questionnaire (HAQ, 0–3, best to worse) (21).
• Health-related quality of life (HRQoL) measured by the EuroQol-5 Dimensions (EQ-5D), which consists of 5 questions addressing mobility, self-care, pain, usual activities, and psychological status (0–1, worst to best) (22).
• HRQoL was also evaluated using the Short-Form 36 Health Survey (SF-36), which has 36 questions covering 8 subscales: physical function, bodily pain, role physical, general health, vitality, social function, mental health, and role emotional (each scored from 0 to 100, worst to best) (23).
• Pain and fatigue, measured with numeral rating scales (NRS, 0–10, best to worst).
Rehabilitation goals. In the present study, rehabilitation goals were included from the selected patient records if they were designated as being a rehabilitation goal by the multidisciplinary team, irrespective of whether they met the definitions of rehabilitation goals in the literature (5–7). The goal-setting process differed between countries. In the selected Swedish, Norwegian and Danish centres, patients were asked to formulate the main goals for their rehabilitation in their own words at admission, with a maximum of 3 in Norway and Sweden, and no limits in Denmark. In the Netherlands, the rehabilitation goals were formulated using an adapted version of an ICF-based rehabilitation tool, the RAP (10).
The rehabilitation goals of the included patients were extracted from the medical records by local investigators and translated into English by the local investigator and a local health professional, working independently. The translations were then compared and any disagreements discussed until a consensus was achieved. The translated rehabilitation goals were subsequently linked to the ICF by using established ICF linking rules (24). This was done independently by 2 investigators with experience in ICF linking procedures (JM and WP) (Fig. 1). For this purpose the qualitative data analysis followed the method of meaning condensation (25). The rehabilitation goals were considered as meaning units, defined as words or phrases that were related to each other by content, followed and preceded by a shift of meaning in a text. Within these meaning units, meaningful concepts were identified. In the second step, 2 investigators independently linked each meaningful concept obtained from rehabilitation goals to the most precise ICF component (1st level), chapter (2nd level) and/or category (3rd or 4th level) according to established linking rules (24). In this process, one meaningful concept can be linked to more than one ICF category. If a meaningful concept was not contained in the ICF classification, this concept was assigned as “not classified”, and if a concept was related to the patient’s health condition this concept was assigned to “health condition” (26). The resulting ICF codes were then compared between the 2 investigators and any disagreements were discussed until a consensus was achieved.
Fig. 1. An example of the process of linking the contents of a rehabilitation goal to corresponding ICF categories.
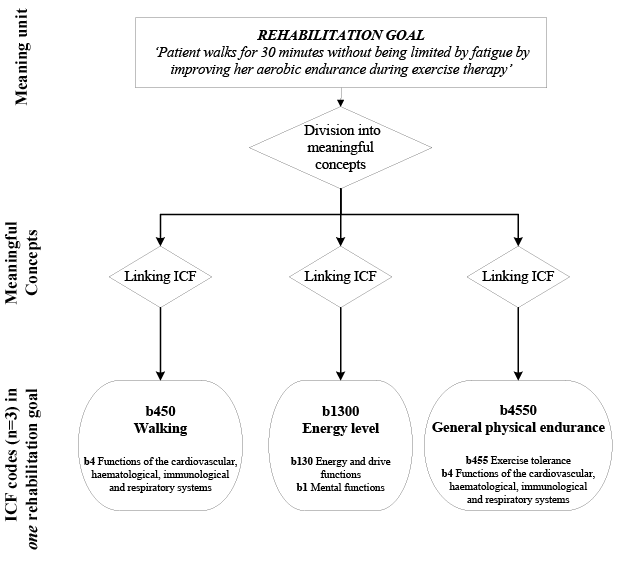
This process resulted in lists of codes on different levels of the ICF. However, ICF categories are “nested”, so that the more detailed second, third and fourth categories are included in ICF chapters. Therefore, each meaningful concept that was linked to an ICF code on the level of second, third or fourth category was also given an ICF code on the level of the corresponding higher ICF levels. Thus, comparisons of frequencies within and among countries and with the contents of the comprehensive ICF Core Set for RA were facilitated. For example, if the meaningful concept was drying oneself, then this was assigned the ICF codes d5102 “Drying oneself”, but also to d510 “Washing oneself”, and d5 “Self care”.
Data analysis
Descriptive statistics were used to analyse patients’ socio-demographic and disease characteristics data, and inferential statistics (Mann-Whitney U test, unpaired t-tests or χ2 tests) were used to assess differences and associations between groups as appropriate. The median (range) number of goals per patient was computed for each of the 4 countries, and then the difference between the medians was assessed using the Mann-Whitney U test. Statistical analyses were performed using the Statistical Package for the Social Sciences (IBM SPSS Statistics 20.0 for Windows; available from: URL: http://www-01.ibm.com/software/analytics/spss/).
The ICF codes derived from the rehabilitation goals were reported as absolute numbers and as relative frequency for all patients and stratified by country. The relative frequency was defined as the absolute frequency of an ICF code divided by the total number of ICF codes that were identified in the rehabilitation goals. The overlap with the comprehensive ICF Core Set for RA (26) was determined by comparing the list of unique ICF codes from the rehabilitation goals with the ICF codes within this Core Set. All levels of ICF codes assigned to meaningful concepts were taken into account.
RESULTS
Patient characteristics
Table II shows the baseline characteristics of 497 patients with RA in the STAR-ETIC project, 80 of whom were included and 417 excluded in the present study. Overall, there were no significant differences between the included and excluded groups, except for pain and fatigue scores, which were significantly higher in the included patients (mean difference = 0.6, p = 0.05 and 0.7, p = 0.02 for pain and fatigue, respectively).
|
Table II. Baseline characteristics of 497 patients with rheumatoid arthritis (RA) included in an international study on rehabilitation in patients with rheumatic and musculoskeletal conditions, of whom 80 were included in the present study on rehabilitation goals |
|||
|
Patients with RA included in present study (n = 80) |
Patients with RA not included (n = 417) |
p-valuea |
|
|
Age, years, mean (SD) |
59.0 (0.7) |
59.2 (1.3) |
0.92 |
|
Health Assessment Questionnaire (0–3), mean (SD) |
1.20 (0.62) |
1.07 (0.63) |
0.12 |
|
EuroQol-5D (0–1)**, mean (SD) Short Form-36 subscales (0–100), mean (SD) |
0.53 (0.26) |
0.54 (0.28) |
0.82 |
|
SF-36 bodily pain |
35.24 (17.16) |
38.18 (19.77) |
0.22 |
|
SF-36 general health |
41.13 (18.99) |
44.90 (19.23) |
0.12 |
|
SF-36 mental health |
68.21 (21.28) |
67.89 (18.21) |
0.89 |
|
SF-36 physical function |
40.00 (21.94) |
45.12 (24.99) |
0.10 |
|
SF-36 role emotional |
52.72 (43.02) |
53.18 (43.27) |
0.93 |
|
SF-36 role physical |
26.77 (32.85) |
26.39 (35.60) |
0.93 |
|
SF-36 social function |
59.36 (24.48) |
64.04 (27.90) |
0.17 |
|
SF-36 vitality |
39.19 (22.18) |
40.19 (21.75) |
0.71 |
|
Numeric Rating Scale, 0–10, medain (range) |
|||
|
Fatigue |
6.0 (0–10) |
6.0 (0–10) |
0.05 |
|
Pain |
6.0 (1–10) |
5.0 (0–10) |
0.02 |
|
Gender, female, n (%) |
58 (73) |
328 (79) |
0.23 |
|
Education > 12 years, n (%) |
21 (27) |
115 (32) |
0.07 |
|
Number of co-morbidities > 0, n (%) |
60 (77) |
296 (79) |
0.69 |
|
Living with partner and/or family, n (%) |
46 (60) |
239 (66) |
0.34 |
|
Paid work, n (%) |
20 (26) |
108 (30) |
0.47 |
|
Using oral steroids, n (%) |
27 (36) |
130 (38) |
0.81 |
|
Using disease-modifying anti-rheumatic drug, n (%) |
55 (72) |
259 (72) |
0.94 |
|
Using biologicals , n (%) |
23 (31) |
88 (26) |
0.43 |
|
*Comparisons between the selected patients and non-selected group of patients with RA were employed with Mann-Whitney U tests, unpaired t-tests or χ2 tests, where appropriate. Bold numbers indicate p < 0.05. aData not available from Norwegian patients. SD: standard deviation. |
|||
Rehabilitation goals
In total, 495 rehabilitation goals were identified. The meaningful concepts in these 495 goals were subsequently linked to 952 ICF codes, comprising 151 unique ICF categories. In the 495 rehabilitation goals, 12 meaningful concepts could not be classified or were assigned to the category “Not classifiable” or “Not classifiable – quality of life” and 44 meaningful concepts were linked to the patient’s “Health condition”, e.g. “the patient’s neurological complaints are examined”.
The median (range) numbers of rehabilitation goals per patient were 5.5 (2–9), 14.0 (5–24), 2.0 (1–3) and 3.0 (1–3) in Denmark, the Netherlands, Norway and Sweden, respectively. There was a significant difference between the countries that limit the number of rehabilitation goals (Norway and Sweden, median 3.0) and those allowing an unlimited number of rehabilitation goals (Denmark and the Netherlands, median 8.5, p < 0.001).
Rehabilitation goals at the level of ICF components
At the level of ICF components, 275 of the 952 ICF codes (29%) were related to “Body Functions” (b-codes), 80 (8%) to “Body Structures” (s-codes), 419 (44%) to “Activities and Participation” (d-codes) and 178 (19%) to “Environmental Factors” (e-codes). In all countries, the frequency of ICF codes related to “Activities and Participation” was highest, with the exception of Sweden, where the majority of ICF codes occurred in “Body Functions”.
The contents of the rehabilitation goals within the ICF components “Body Functions” and “Body Structures” is shown in Tables III and IV. Of the 275 ICF codes within “Body Functions”, 73 pertained to the chapter “Mental functions” (b1), 52 to “Sensory functions and pain” (b2), 30 to “Functions of the cardiovascular, haematological, immunological and respiratory systems” (b4), 4 to “Functions of the digestive, metabolic and endocrine system” (b5), 115 to “Neuromusculoskeletal and movement-related function” (b7), and 1 to “Functions of the skin and related structures” (b8). “Generalized pain” (b2800), “Mobility of several joints” (b7101), and “Experience of self and time functions” (b180) were overall the most frequent ICF codes on the level of ICF categories, with only “Generalized pain” being among the most frequent codes in all 4 countries (Table III). An example of a rehabilitation goal that comprises the ICF category “Generalized pain” (b2800) is the following goal from Norway: “To get an easier life with less pain”. Of the 80 ICF codes within “Body Structures”, “Joints of hand and fingers” (s730210) and “Muscles of hand” (s 7302) were the most frequent; however, this result was seen within only 2 of the 4 countries (Denmark and the Netherlands), whereas in the other 2 countries ICF codes on the level of “Body Structures” were nearly rare (Table IV). An example of a rehabilitation goal that comprises the ICF category “Muscles of hand” (s7302) is the following goal from the Netherlands: “patient has muscle strength exercises for hands to improve the opening of jars”.
The contents of the rehabilitation goals within the ICF component “Activities and Participation” is shown in Table V. Of the 419 ICF codes within “Activities and Participation, 116 pertained to the chapter “Learning and applying knowledge” (d1), 49 to “General tasks and demands” (d2), 4 to “Communication” (d3), 115 to “Mobility” (d4), 82 to “Self care” (d5), 20 to “Domestic life” (d6), 8 to “Interpersonal interactions and relationships” (d7), 9 to “Major life areas” (d8) and 16 to “Community, social and civic life” (d9). Overall, “Learning and applying knowledge” (d1) was the most frequent ICF code within the component “Activities and Participation”; however, this was due to the relatively high frequency in 2 of the 4 countries (Denmark and the Netherlands). “Managing one’s own activity level” (d2303) was also relatively common, for all rehabilitation goals together, as well as in 3 of the 4 countries (Denmark, the Netherlands and Norway). Two other relatively frequent ICF codes, in total and in 2 of the 4 countries, were “Walking” (d450) (Denmark and the Netherlands) and “Looking after one’s health” (d570) (the Netherlands and Norway) (Table V). An example of a rehabilitation goal that comprises the ICF category “Learning and applying knowledge” (d1), which is closely related to the concept of self-management, is the following goal from the Netherlands: “Enlarging knowledge regarding RA by receiving disease-related information from the team, both oral and in writing”. An example of a rehabilitation goal that comprises the ICF category “Managing one’s own activity level” (d2303) is the following goal from Sweden: “To somewhat better balance activity and pain.”
The contents of the rehabilitation goals within the ICF component “Environmental Factors” are shown in Table VI, as well as the meaningful concepts that were linked to the health condition or could not be classified. Of the 178 ICF codes within “Environmental Factors”, 137 pertained to the chapter “Products and technology” (e1), 16 to “Support and relationships” (e3) and 25 to “Services, systems and policies” (e5). In total, and in 2 of the 4 countries (Denmark and the Netherlands) Drugs (e1101) and “Assistive products and technology for personal use in daily living” (e1151) were the most common. In the goals of patients from Sweden and Norway ICF codes within the ICF component “Environmental Factors” were overall very uncommon (Table VI). An example of a rehabilitation goal that comprises the ICF category “Assistive products and technology for personal use in daily living” (e1151) is the following goal from Denmark: “Going through aids for personal hygiene”.
The majority of meaningful concepts linked to “health condition” occurred in goals derived from the Netherlands. Unclassifiable goals were relatively uncommon in all 4 countries.
|
Table III. International Classification of Functioning, Disability and Health (ICF) codes in the ICF-components “Body Functions” derived from the rehabilitation goals of patients with rheumatoid arthritis (RA) and present in the comprehensive ICF Core Set for RA |
|||||||
|
ALL (n = 80) |
DE (n = 20) |
NE (n = 20) |
NO (n = 20) |
SW (n = 20) |
ICF CS RA |
||
|
Rehabilitation goals, n |
495 |
110 |
292 |
50 |
52 |
||
|
Rehabilitation goals per patient, median, n (min–max) |
6.0 (1–24) |
5.5 (2–9) |
14.0 (5–24) |
2.0 (1–3) |
3.0 (1–3) |
||
|
ICF within the component , n (%)a |
178 (19) |
34 (20) |
139 (22) |
4 (6) |
1 (1) |
||
|
ICF code |
|||||||
|
b1 |
Mental functions |
73 |
8 |
45 |
10 |
10 |
|
|
b1c |
Mental functions |
3 |
– |
– |
1 |
2 |
|
|
b126c |
Temperament and personality functions |
1 |
– |
– |
– |
1 |
|
|
b1266c |
Confidence |
1 |
– |
– |
1 |
– |
|
|
b1300 |
Energy level |
14 |
2 |
5 |
5 |
2 |
● |
|
b1301 |
Motivation |
2 |
– |
1 |
1 |
– |
|
|
b134 |
Sleep functions |
8 |
1 |
6 |
– |
1 |
● |
|
b1342 |
Maintenance of sleep |
1 |
– |
1 |
– |
– |
|
|
b1344 |
Functions involving the sleep cycle |
4 |
1 |
3 |
– |
– |
|
|
b147c |
Psychomotor functions |
13 |
4 |
5 |
1 |
3 |
|
|
b152 |
Emotional functions |
2 |
– |
– |
1 |
1 |
● |
|
b1644c |
Insight |
4 |
– |
4 |
– |
– |
|
|
b180 |
Experience of self and time functions |
20 |
– |
20 |
– |
– |
● |
|
b1801 |
Body image |
– |
– |
– |
– |
– |
● |
|
b2 |
Sensory functions and pain |
52 |
11 |
26 |
6 |
9 |
|
|
b2c |
Sensory functions and pain |
2 |
– |
2 |
– |
– |
|
|
b2351c |
Vestibular function of balance |
2 |
– |
2 |
– |
– |
|
|
b2402c |
Sensation of falling |
1 |
1 |
– |
– |
– |
|
|
b280 |
Sensation of pain |
– |
– |
– |
– |
– |
● |
|
b2800 |
Generalized pain |
36 |
7 |
16 |
6 |
7 |
● |
|
b2801 |
Pain in body part |
– |
– |
– |
– |
– |
● |
|
b28010 |
Pain in head and neck |
2 |
1 |
– |
– |
1 |
● |
|
b28013 |
Pain in back |
2 |
1 |
1 |
– |
– |
● |
|
b28014 |
Pain in upper limb |
5 |
– |
4 |
– |
1 |
● |
|
b28015 |
Pain in lower limb |
1 |
1 |
– |
– |
– |
● |
|
b28016 |
Pain in joints |
1 |
– |
1 |
– |
– |
● |
|
b4 |
Functions of the cardiovascular, haematological, immunological and respiratory systems |
30 |
5 |
15 |
3 |
7 |
|
|
b4150c |
Functions of arteries |
1 |
– |
1 |
– |
– |
|
|
b430b |
Haematological system functions |
– |
– |
– |
– |
– |
● |
|
b4451c |
Functions of the diaphragm |
6 |
– |
4 |
1 |
1 |
|
|
b455 |
Exercise tolerance functions |
– |
– |
– |
– |
– |
● |
|
b4550 |
General physical endurance |
17 |
5 |
8 |
2 |
2 |
|
|
b4551 |
Aerobic capacity |
5 |
– |
1 |
– |
4 |
|
|
b4552 |
Fatigability |
1 |
– |
1 |
– |
– |
|
|
b5 |
Functions of the digestive, metabolic and endocrine systems |
4 |
0 |
1 |
0 |
3 |
|
|
b510b |
Ingestion functions |
– |
– |
– |
– |
– |
● |
|
b515c |
Digestive functions |
1 |
– |
1 |
– |
– |
|
|
b530c |
Weight maintenance functions |
3 |
– |
– |
– |
3 |
|
|
b6 |
Genitourinary and reproductive functions |
0 |
0 |
0 |
0 |
0 |
|
|
b640b |
Sexual functions |
– |
– |
– |
– |
– |
● |
|
b7 |
Neuromusculoskeletal and movement-related functions |
115 |
29 |
54 |
9 |
23 |
|
|
Neuromusculoskeletal and movement-related functions |
6 |
– |
1 |
3 |
2 |
||
|
b710 |
Mobility of joint functions |
2 |
– |
2 |
– |
– |
● |
|
b7100 |
Mobility of a single joint |
1 |
– |
1 |
– |
– |
|
|
b7101 |
Mobility of several joints |
30 |
8 |
20 |
1 |
1 |
|
|
b7102 |
Mobility of joints generalized |
13 |
1 |
2 |
3 |
7 |
● |
|
b715 |
Stability of joint functions |
– |
– |
– |
– |
– |
● |
|
b7151 |
Stability of several joints |
3 |
3 |
– |
– |
– |
|
|
b7152 |
Stability of joints generalized |
2 |
2 |
– |
– |
– |
|
|
b730 |
Muscle power functions |
– |
– |
– |
– |
– |
● |
|
b7300 |
Power of isolated muscles and muscle groups |
5 |
4 |
1 |
– |
– |
|
|
b7301 |
Power of muscles of one limb |
19 |
1 |
17 |
– |
1 |
|
|
b7303 |
Power of muscles in lower half of the body |
3 |
– |
3 |
– |
– |
|
|
b7304 |
Power of muscles of all limbs |
1 |
– |
– |
– |
1 |
|

|
Table III. Contd. |
|||||||
|
ALL (n = 80) |
DE (n = 20) |
NE (n = 20) |
NO (n = 20) |
SW (n = 20) |
ICF CS RA |
||
|
b7305 |
Power of muscles of the trunk |
3 |
– |
1 |
– |
2 |
|
|
b7306 |
Power of all muscles of the body |
11 |
1 |
3 |
1 |
6 |
|
|
b740 |
Muscle endurance functions |
– |
– |
– |
– |
– |
● |
|
b7401 |
Endurance of muscle groups |
5 |
5 |
– |
– |
– |
|
|
b7402 |
Endurance of all muscles of the body |
1 |
1 |
– |
– |
– |
|
|
b755c |
Involuntary movement reaction functions |
3 |
2 |
– |
– |
1 |
|
|
b760c |
Control of voluntary movement functions |
3 |
– |
1 |
– |
2 |
|
|
b7602c |
Coordination of voluntary movements |
1 |
– |
1 |
– |
– |
|
|
b770 |
Gait pattern functions |
1 |
– |
1 |
– |
– |
● |
|
b780 |
Sensations related to muscles and movement functions |
– |
– |
– |
– |
– |
● |
|
b7800 |
Sensation of muscle stiffness |
2 |
1 |
– |
1 |
– |
● |
|
b8 |
Functions of the skin and related structures |
1 |
0 |
1 |
0 |
0 |
|
|
b840c |
Sensation related to the skin |
1 |
– |
1 |
– |
– |
|
|
Results are listed as absolute numbers unless mentioned otherwise. a(% of total number of ICF codes). bICF categories from the ICF Core Set for RA that were not in the rehabilitation goals. cICF categories that were in the rehabilitation goals that are not in the ICF Core Set for RA. |
|||||||
|
Table IV. International Classification of Functioning, Disability and Health (ICF) codes in the ICF-components “Body Structures” derived from the rehabilitation goals of patients with rheumatoid arthritis (RA) and present in the comprehensive ICF Core Set for RA |
|||||||
|
ALL (n = 80) |
DE (n = 20) |
NE (n = 20) |
NO (n = 20) |
SW (n = 20) |
ICF CS RA |
||
|
Rehabilitation goals, n |
495 |
110 |
292 |
50 |
52 |
||
|
Rehabilitation goals per patient, median, n (min–max) |
6.0 (1–24) |
5.5(2–9) |
14.0 (5–24) |
2.0 (1–3) |
3.0 (1–3) |
||
|
ICF within the e-component, n (%)a |
178 (19) |
34 (20) |
139 (22) |
4 (6) |
1 (1) |
||
|
ICF code |
|||||||
|
s2 |
The eye, ear and related structures |
0 |
0 |
0 |
0 |
0 |
|
|
s299b |
Eye, ear and related structures, unspecified |
– |
– |
– |
– |
– |
● |
|
s7 |
Structures related to movement |
80 |
24 |
52 |
2 |
2 |
|
|
s710 |
Structure of head and neck region |
1 |
– |
1 |
– |
– |
● |
|
s720 |
Structure of shoulder region |
5 |
– |
5 |
– |
– |
● |
|
s7201 |
Joints of shoulder region |
4 |
– |
2 |
2 |
– |
|
|
s7208 |
Structure of shoulder region, other specified |
1 |
– |
1 |
– |
– |
|
|
s730 |
Structure of upper extremity |
4 |
2 |
2 |
– |
– |
● |
|
s73001 |
Elbow joint |
1 |
1 |
– |
– |
– |
● |
|
s73011 |
Wrist joint |
5 |
1 |
4 |
– |
– |
● |
|
s73012 |
Muscles of forearm |
1 |
– |
1 |
– |
– |
|
|
s7302 |
Structure of hand |
10 |
2 |
8 |
– |
– |
● |
|
s73021 |
Joints of hand and fingers |
15 |
5 |
10 |
– |
– |
● |
|
s73022 |
Muscles of hand |
16 |
4 |
12 |
– |
– |
● |
|
s73023 |
Ligaments and fasciae of hand |
1 |
1 |
– |
– |
– |
|
|
s750 |
Structure of lower extremity |
5 |
4 |
1 |
– |
– |
● |
|
s75001 |
Hip joint |
1 |
– |
– |
– |
1 |
● |
|
s75002 |
Muscles of thigh |
3 |
1 |
2 |
– |
– |
|
|
s75011 |
Knee joint |
1 |
– |
1 |
– |
– |
● |
|
s7502 |
Structure of ankle and foot |
1 |
– |
1 |
– |
– |
● |
|
s75021 |
Ankle joint and joints of foot and toes |
1 |
1 |
– |
– |
– |
|
|
s760 |
Structure of trunk |
1 |
1 |
– |
– |
– |
|
|
s7600 |
Structure of vertebral column |
3 |
1 |
1 |
– |
1 |
|
|
s76000 |
Cervical vertebral column |
– |
– |
– |
– |
– |
● |
|
s770b |
Additional musculoskeletal structures related to movement |
– |
– |
– |
– |
– |
● |
|
s8 |
Skin and related structures |
0 |
0 |
0 |
0 |
0 |
|
|
s810b |
Structure of areas of skin |
– |
– |
– |
– |
– |
● |
|
Results are listed as absolute numbers unless mentioned otherwise. a% of total number of ICF codes. bICF categories from the ICF Core Set for RA that were not that not in the rehabilitation goals. cICF categories that were in the rehabilitation goals that are not in the ICF Core Set for RA. |
|||||||
Overlap between ICF categories from the comprehensive ICF Core Set for RA and ICF categories that were addressed in the rehabilitation goals
The comprehensive ICF Core Set for RA includes 96 unique ICF categories, with 25 categories from the component “Body Functions”, 18 from “Body Structures”, 32 from “Activities and Participation”, and 21 from “Environmental Factors” (26). Twenty-three of the ICF categories (24%) from the comprehensive ICF Core Set for RA were not seen in the rehabilitation goals. These included 3 categories from the component “Body Functions”, 3 from “Body Structures”, 7 from “Activities and Participation”, and 10 from “Environmental Factors”. Moreover, 25 of the 152 unique ICF categories (23%) identified in the rehabilitation goals could not be linked to the contents of the comprehensive ICF Core Set for RA (b in Tables III–VI). These included 17 categories from the component “Body Functions”, 15 from “Activities and Participation”, and 3 from “Environmental Factors”. Examples from this latter category are given for the most frequently mentioned ICF categories. An example of a goal from Sweden that comprises the category “Psychomotor functions” (b147), which is not included in the ICF Core Set for RA, is: “to find acceptance for the disease”. Another example of a goal comprising a topic that is not included in the ICF Core Set for RA was category “Solving problems” (d175) derived from the following goal from the Netherlands: “Patient has learned the right way to administer her own medication”.
|
Table V. International Classification of Functioning, Disability and Health (ICF) codes in the ICF-component “Activities and Participation” derived from the rehabilitation goals of patients with rheumatoid arthritis (RA) and present in the comprehensive ICF Core Set for RA |
|||||||
|
ALL (n = 80) |
DE (n =20) |
NE (n =20) |
NO (n =20) |
SW (n =20) |
ICF CS RA |
||
|
Rehabilitation goals, n |
495 |
110 |
292 |
50 |
52 |
||
|
Rehabilitation goals per patient, median, n (min–max) |
6.0 (1–24) |
5.5 (2–9) |
14.0 (5–24) |
2.0 (1–3) |
3.0 (1–3) |
||
|
ICF within the component, n (%)a |
178 (19) |
34 (20) |
139 (22) |
4 (6) |
1 (1) |
||
|
ICF code |
|
|
|
|
|
|
|
|
d1 |
Learning and applying knowledge |
116 |
17 |
96 |
1 |
2 |
|
|
d1b |
Learning and applying knowledge |
103 |
16 |
84 |
1 |
2 |
|
|
d170 |
Writing |
1 |
– |
1 |
– |
– |
● |
|
d175c |
Solving problems |
12 |
1 |
11 |
– |
– |
|
|
d2 |
General tasks and demands |
49 |
14 |
24 |
9 |
2 |
|
|
d230 |
Carrying out daily routine |
14 |
5 |
3 |
6 |
– |
● |
|
d2303 |
Managing one’s own activity level |
35 |
9 |
21 |
3 |
2 |
|
|
d3 |
Communication |
4 |
0 |
4 |
0 |
0 |
|
|
d360 |
Using communication devices and techniques |
– |
– |
– |
– |
– |
● |
|
d3601 |
Using writing machines |
4 |
– |
4 |
– |
– |
|
|
d4 |
Mobility |
115 |
16 |
87 |
5 |
7 |
|
|
d4c |
Mobility |
3 |
3 |
– |
– |
– |
|
|
d410 |
Changing basic body position |
– |
– |
– |
– |
– |
● |
|
d4100 |
Lying down |
1 |
– |
– |
1 |
– |
|
|
d4103 |
Sitting |
11 |
1 |
9 |
– |
1 |
|
|
d4104 |
Standing |
1 |
– |
– |
1 |
– |
|
|
d4105 |
Bending |
2 |
– |
1 |
– |
1 |
|
|
d415 |
Maintaining a body position |
6 |
– |
4 |
– |
2 |
● |
|
d4150 |
Maintaining a lying position |
2 |
– |
2 |
– |
– |
|
|
d4153 |
Maintaining a sitting position |
12 |
1 |
10 |
– |
1 |
|
|
d4154 |
Maintaining a standing position |
2 |
– |
2 |
– |
– |
|
|
d420c |
Transferring oneself |
1 |
– |
1 |
– |
– |
|
|
d4201c |
Transferring oneself while lying |
1 |
– |
1 |
– |
– |
|
|
d430 |
Lifting and carrying objects |
1 |
– |
1 |
– |
– |
● |
|
d4300 |
Lifting |
7 |
– |
7 |
– |
– |
|
|
d4351c |
Kicking |
1 |
– |
1 |
– |
– |
|
|
d440 |
Fine hand use |
11 |
3 |
8 |
– |
– |
● |
|
d4401 |
Grasping |
3 |
– |
3 |
– |
– |
|

|
Table V. Contd. |
|||||||
|
ALL (n = 80) |
DE (n =20) |
NE (n =20) |
NO (n =20) |
SW (n =20) |
ICF CS RA |
||
|
d4402 |
Manipulating |
8 |
– |
8 |
– |
– |
|
|
d445 |
Hand and arm use |
– |
– |
– |
– |
– |
● |
|
d4452 |
Reaching |
2 |
– |
2 |
– |
– |
|
|
d449b |
Carrying, moving and handling objects, other specified and unspecified |
– |
– |
– |
– |
– |
● |
|
d450 |
Walking |
22 |
7 |
12 |
2 |
1 |
● |
|
d4501 |
Walking long distances |
1 |
– |
– |
– |
1 |
|
|
d455 |
Moving around |
– |
– |
– |
– |
– |
● |
|
d4551 |
Climbing |
6 |
1 |
5 |
– |
– |
|
|
d460 |
Moving around in different locations |
– |
– |
– |
– |
– |
● |
|
d4602 |
Moving around outside the home and other buildings |
1 |
– |
1 |
– |
– |
|
|
d465 |
Moving around using equipment |
2 |
– |
1 |
1 |
– |
● |
|
d470 |
Using transportation |
– |
– |
– |
– |
– |
● |
|
d4701 |
Using private motorized transportation |
1 |
– |
1 |
– |
– |
|
|
d475 |
Driving |
– |
– |
– |
– |
– |
● |
|
d4750 |
Driving human-powered transportation |
6 |
– |
6 |
– |
– |
|
|
d4751 |
Driving motorized vehicles |
1 |
– |
1 |
– |
– |
|
|
d5 |
Self care |
82 |
8 |
67 |
2 |
5 |
|
|
d5b |
Self-care |
1 |
1 |
– |
– |
– |
|
|
d510 |
Washing oneself |
– |
– |
– |
– |
– |
● |
|
d5100 |
Washing body parts |
3 |
– |
3 |
– |
– |
|
|
d5102 |
Drying oneself |
2 |
1 |
1 |
– |
– |
|
|
d520b |
Caring for body parts |
– |
– |
– |
– |
– |
● |
|
d530 |
Toileting |
5 |
– |
4 |
– |
1 |
● |
|
d540 |
Dressing |
4 |
– |
4 |
– |
– |
● |
|
d5400 |
Putting on clothes |
4 |
– |
4 |
– |
– |
|
|
d5402 |
Putting on footwear |
3 |
1 |
2 |
– |
– |
|
|
d550 |
Eating |
4 |
– |
4 |
– |
– |
● |
|
d560b |
Drinking |
– |
– |
– |
– |
– |
● |
|
d570 |
Looking after one’s health |
56 |
5 |
45 |
2 |
4 |
● |
|
d6 |
Domestic life |
20 |
1 |
16 |
2 |
1 |
|
|
d6c |
Domestic life |
1 |
– |
– |
1 |
– |
|
|
d620b |
Acquisition of goods and services |
– |
– |
– |
– |
– |
● |
|
d630 |
Preparing meals |
7 |
1 |
5 |
1 |
– |
● |
|
d640 |
Doing housework |
6 |
– |
6 |
– |
– |
● |
|
d6400 |
Washing and drying clothes and garments |
1 |
– |
1 |
– |
– |
|
|
d6402 |
Cleaning living area |
1 |
– |
1 |
– |
– |
|
|
d6403 |
Using household appliances |
1 |
– |
1 |
– |
– |
|
|
d650c |
Caring for household objects |
1 |
– |
1 |
– |
– |
|
|
d6505c |
Taking care of plants, indoors and outdoors |
1 |
– |
– |
– |
1 |
|
|
d660 |
Assisting others |
1 |
– |
1 |
– |
– |
● |
|
d7 |
Interpersonal interactions and relationships |
8 |
0 |
4 |
4 |
0 |
|
|
d7c |
Interpersonal interactions and relationships |
3 |
– |
2 |
1 |
– |
|
|
d7200c |
Forming relationships |
1 |
– |
1 |
– |
– |
|
|
d7202c |
Regulating behaviours within interactions |
1 |
– |
1 |
– |
– |
|
|
d750c |
Informal social relationships |
3 |
– |
– |
3 |
– |
|
|
d760b |
Family relationships |
– |
– |
– |
– |
– |
● |
|
d770b |
Intimate relationships |
– |
– |
– |
– |
– |
● |
|
d8 |
Major life areas |
9 |
2 |
4 |
3 |
0 |
|
|
d8451c |
Maintaining a job |
1 |
1 |
– |
– |
– |
|
|
d850 |
Remunerative employment |
8 |
1 |
4 |
3 |
– |
● |
|
d859 |
Work and employment, other specified and unspecified |
– |
– |
– |
– |
– |
● |
|
d9 |
Community, social and civic life |
16 |
1 |
11 |
3 |
1 |
|
|
d910b |
Community life |
– |
– |
– |
– |
– |
● |
|
d920 |
Recreation and leisure |
1 |
– |
1 |
– |
– |
● |
|
d9201 |
Sports |
7 |
1 |
5 |
– |
1 |
|
|
d9204 |
Hobbies |
5 |
– |
5 |
– |
– |
|
|
d9205 |
Socializing |
3 |
– |
– |
3 |
– |
|
|
Results are listed as absolute numbers unless mentioned otherwise. a% of total number of ICF codes. bICF categories from the ICF Core Set for RA that were not that not in the rehabilitation goals. cICF categories that were in the rehabilitation goals that are not in the ICF Core Set for RA. |
|||||||
|
Table VI. International Classification of Functioning, Disability and Health (ICF) codes in the ICF-component “Environmental Factors” derived from the rehabilitation goals of patients with rheumatoid arthritis (RA) and present in the comprehensive ICF Core Set for RA |
|||||||
|
ALL (n = 80) |
DE (n = 20) |
NE (n = 20) |
NO (n = 20) |
SW (n = 20) |
ICF CS RA |
||
|
Rehabilitation goals, n |
495 |
110 |
292 |
50 |
52 |
||
|
Rehabilitation goals per patient, median, n (min–max) |
6.0 (1–24) |
5.5 (2–9) |
14.0 (5–24) |
2.0 (1–3) |
3.0 (1–3) |
||
|
ICF within the component, n (%)a |
178 (19) |
34 (20) |
139 (22) |
4 (6) |
1 (1) |
||
|
ICF code |
|
|
|
|
|
|
|
|
e1 |
Products and technology |
137 |
33 |
101 |
2 |
1 |
|
|
e110 |
Products or substances for personal consumption |
1 |
1 |
– |
– |
– |
● |
|
e1101 |
Drugs |
54 |
13 |
38 |
2 |
1 |
|
|
e115b |
Products and technology for personal use in daily living |
– |
– |
– |
– |
– |
● |
|
e1150 |
General products and technology for personal use in daily living |
1 |
– |
1 |
– |
– |
|
|
e1151 |
Assistive products and technology for personal use in daily living |
64 |
19 |
45 |
– |
– |
|
|
e120 |
Products and technology for personal indoor and outdoor mobility and transportation |
– |
– |
– |
– |
– |
● |
|
e1200 |
General products and technology for personal indoor and outdoor mobility and transportation |
1 |
– |
1 |
– |
– |
|
|
e1201 |
Assistive products and technology for personal indoor and outdoor mobility and transportation |
8 |
– |
8 |
– |
– |
|
|
e125 |
Products and technology for communication |
– |
– |
– |
– |
– |
● |
|
e1251 |
Assistive products and technology for communication |
5 |
– |
5 |
– |
– |
|
|
e135b |
Products and technology for employment |
– |
– |
– |
– |
– |
● |
|
e150b |
Design, construction and building products and technology of buildings for public use |
– |
– |
– |
– |
– |
● |
|
e155 |
Design, construction and building products and technology of buildings for private use |
– |
– |
– |
– |
– |
● |
|
e1550 |
Design, construction and building products and technology for entering and exiting of buildings for private use |
2 |
– |
2 |
– |
– |
|
|
e1551 |
Design, construction and building products and technology for gaining access to facilities in buildings for private use |
1 |
– |
1 |
– |
– |
|
|
e2 |
Natural environment and human-made changes to environment |
0 |
0 |
0 |
0 |
0 |
|
|
e225b |
Climate |
– |
– |
– |
– |
– |
● |
|
e3 |
Support and relationships |
16 |
0 |
16 |
0 |
0 |
|
|
e3b |
Support and relationships |
1 |
– |
1 |
– |
– |
|
|
e310 |
Immediate family |
2 |
– |
2 |
– |
– |
● |
|
e320b |
Friends |
– |
– |
– |
– |
– |
● |
|
e340 |
Personal care providers and personal assistants |
3 |
– |
3 |
– |
– |
● |
|
e355 |
Health professionals |
8 |
– |
8 |
– |
– |
● |
|
e360 |
Other professionals |
2 |
– |
2 |
– |
– |
● |
|
e4 |
Attitudes |
0 |
0 |
0 |
0 |
0 |
|
|
e410b |
Individual attitudes of immediate family members |
– |
– |
– |
– |
– |
● |
|
e420b |
Individual attitudes of friends |
– |
– |
– |
– |
– |
● |
|
e425b |
Individual attitudes of acquaintances, peers, colleagues, neighbours and community members |
– |
– |
– |
– |
– |
● |
|
e450b |
Individual attitudes of health professionals |
– |
– |
– |
– |
– |
● |
|
e460b |
Societal attitudes |
– |
– |
– |
– |
– |
● |
|
e5 |
Services, systems and policies |
25 |
1 |
22 |
2 |
0 |
|
|
e540 |
Transportation services, systems and policies |
– |
– |
– |
– |
– |
● |
|
e5400 |
Transportation services |
1 |
– |
1 |
– |
– |
|
|
e570 |
Social security services, systems and policies |
– |
– |
– |
– |
– |
● |
|
e5700 |
Social security services |
3 |
– |
3 |
– |
– |
|
|
e5701 |
Social security systems |
1 |
– |
1 |
– |
– |
|
|
e5702 |
Social security policies |
1 |
– |
1 |
– |
– |
|
|
e5750 |
General social support services |
1 |
– |
1 |
– |
– |
|
|
e580 |
Health services, systems and policies |
– |
– |
– |
– |
– |
● |
|
e5800 |
Health services |
13 |
1 |
10 |
2 |
– |
|
|
e5852c |
Education and training policies |
1 |
– |
1 |
– |
– |
|

|
Table VI. Contd. |
|||||||
|
ALL (n = 80) |
DE (n = 20) |
NE (n = 20) |
NO (n = 20) |
SW (n = 20) |
ICF CS RA |
||
|
e5902c |
Labour and employment policies |
4 |
– |
4 |
– |
– |
|
|
Other |
|||||||
|
hc |
Health condition |
44 |
4 |
38 |
– |
2 |
|
|
nc |
Not classifiable |
7 |
1 |
3 |
1 |
2 |
|
|
nc-qol |
Not classifiable, quality of life |
5 |
– |
1 |
4 |
– |
|
|
Results are listed as absolute numbers unless mentioned otherwise. a% of total number of ICF codes bICF categories from the ICF Core Set for RA that were not that not in the rehabilitation goals. cICF categories that were in the rehabilitation goals that are not in the ICF Core Set for RA. hc: health category; nc: not classifiable; nc-qol: not classifiable - quality of Life. |
|||||||
DISCUSSION
Despite considerable differences in this international, multi-centre study, the contents of the rehabilitation goals in 4 countries were predominantly related to the ICF components “Activities and Participation” and “Body Functions”. In addition, the overlap of the rehabilitation goals and the comprehensive ICF Core Set for RA was considerable.
Our findings reveal that, in all the 4 countries, the majority of rehabilitation goals were related to the ICF component “Activities and Participation”, and that this is consistent with the literature regarding the rehabilitation of patients with RA (27–30), emphasizing that rehabilitation should focus mainly on the level of activities and participation. Rehabilitation goals were also relatively frequently related to the ICF component “Body Structures”. The following ICF components were most frequently addressed in the rehabilitation goals: “Environmental Factors Drugs” (e1101) and “Assistive products and technology for personal use in daily living” (e1151). This finding is in line with the observation that the large majority of patients with RA are on drug treatment, and the proportion of patients using assistive devices ranges from 80% to 90% (31, 32). The finding that these interventions are frequently used and are often addressed in rehabilitation goals underscores the need to include the ICF components “Environmental Factors” in rehabilitation goals for patients with RA (10).
This study showed that the mean number of goals per patient differed among study sites. The optimal number of rehabilitation goals remains to be established. In particular, it is unclear whether, and to what extent, the observed contents of the goals were affected by their total number. The results of our study suggest that having no limit with respect to the number of goals leads to more goals related to ICF components other than Body Functions, but rather within the component Activities and Participation. It is not clear whether this implies that goals on the level of Body Functions and Structures are indeed the most important and relevant for patients and/or these are easier to formulate for patients and health professionals.
Moreover, it is largely unknown to what extent the usage of rehabilitation tools improves the quality of rehabilitation. In a previous study, the usage of a rehabilitation tool (i.e. the RAP) appeared to improve patient-centeredness and goal-directedness of care, but did not affect the effectiveness of rehabilitation (10). However, the RAP includes only “Activities and Participation”, whereas the results of our study suggest that other components of the ICF are also relevant. The use of a rehabilitation tool could also contribute to the appropriate formulation of rehabilitation goals. In our study, a considerable number of extracted goals did not fulfil the definition of Bovend’Eerdt et al. (7), “describing a future state of functioning and/or formulation according to the SMART principle implying that a goal is Specific, Measurable, Attainable, Relevant/Realistic and Timely”. In particular, some of the ICF codes directly derived from rehabilitation goals were on such a relatively high level within the ICF (e.g. d1: learning and applying knowledge) or concerned the process by which the goal needed to be achieved rather than the goal itself. This observation makes it clear that in clinical practice more effort must be put into the training of healthcare professionals with respect to rehabilitation goal-setting or the development and implementation of rehabilitation tools facilitating this process.
In this study the contents of the rehabilitation goals were compared with those of the comprehensive ICF Core Set for RA, which was, among other reasons, originally designed to guide multidisciplinary assessments in patients with RA (33). Indeed, the overlap was considerable, such that the usage of the ICF Core Sets for RA and related tools, such as checklists or ICF tools on the ICF Core Sets and the Rehab-Cycle (34), in the rehabilitation of patients with RA seems promising. An example of the successful use of ICF Core Sets in rehabilitation was related to the rehabilitation of patients with spinal cord injury (SCI), where the ICF Core Sets for SCI served as an important reference in the development of a rehabilitation tool to guide the rehabilitation process of patients with SCI (35, 36). In that case, the ICF Core Sets were used as a directive checklist in the assessment to understand the patient’s functioning and to identify the needs to be addressed with a rehabilitative intervention. Furthermore, the Core Sets were used for the identification of rehabilitation goals by using qualifiers to rate the extent of a patient’s problem in a specific ICF category (34, 35). However, the discrepancies between the contents of the ICF Core Set for RA and the actual goals, underline the need for further research on the feasibility and effectiveness of the usage of this Core Set to guide the rehabilitation of individual patients with RA. It is possible that patients with RA in need of rehabilitation constitute a different group than the patients who were included in the development of the Core Sets. The same may pertain to the health professionals involved in the goal-setting in the present study, who may differ from expert health professionals who were involved in the development of Core Sets. Moreover, the Core Sets were developed several years ago and, therefore, they may not adequately reflect recent developments in the treatment of RA and in society and healthcare as a whole. It remains to be established whether ICF categories that are not in the comprehensive ICF Core Set for RA, but that are relatively frequent in the rehabilitation goals (such as codes related to d1 “Learning and applying knowledge”, which are related to self-management), should be added if the ICF Core Set is used for rehabilitation purposes.
The study has a number of limitations. Firstly, and in each country, a site was selected based on the availability of resources to translate the goals. Therefore the study included only a limited number of sites, the results may not be generalized to all the patients with RA in need of rehabilitation. Indeed, in our study, considerable differences in the goal-setting process, as well as the contents of rehabilitation goals were seen among the 4 countries involved. Secondly, the different methods for goal assessment used resulted in an unequal distribution of the number of goals among study sites. In particular, it is unclear whether and to what extent the observed contents of the goals were affected by their total number. Thirdly, linking free text to the ICF is challenging (37), despite the usage of ICF linking rules. The rehabilitation goals were linked to the most precise ICF category possible; however, this hampers the comparison between frequencies on the 2nd, 3rd and 4th level ICF categories. To overcome this problem we also assigned ICF codes on higher levels where applicable.
Despite these limitations, this study is unique in the way the contents of rehabilitation goals for patients with RA are described. This work contributes to the field of rheumatology rehabilitation by providing an insight into what is really happening in the “black box” of rehabilitation. This study indicates that further research is needed into the optimization of goal-setting in the rehabilitation of patients with RA, whether or not rehabilitation tools are used. Furthermore, future research should incorporate strategies to determine whether the rehabilitation goals are well-timed, sufficiently specific and realistic.
ACKNOWLEDGEMENTS
The STAR-ETIC study was financially supported by the European League Against Rheumatism (grant CLI022).
The authors would like to thank all the participating patients and health professionals at all participating rehabilitation sites for their contribution to this article and the STAR-ETIC study in general. The authors would also like to thank Mwidimi Ndosi, PhD, for proofreading and copyediting the manuscript.
The authors declare no conflicts of interest.
REFERENCES

