Anneli Peolsson, PhD, PT1,2, Michael Peolsson, PhD, MSc CE3, Gwendolen Jull, PhD, PT2 and Shaun O’Leary, PhD, PT2,4
From the 1Department of Medical and Health Sciences, Division of Physiotherapy, Faculty of Health Sciences, Linköping University, Linköping, Sweden, 2NHMRC CCRE (Spinal Pain, Injury and Health), The University of Queensland, Brisbane, Australia, 3Computational Life Science Cluster and Department of Chemistry, Umeå University, Umeå, Sweden and 4Physiotherapy Department, Royal Brisbane and Womens Hospital, Queensland Health, Queensland, Australia
OBJECTIVE: Guild boards and pulleys are apparatus commonly used to train cervical muscle function for their purported benefit in facilitating activity of the deeper muscle layers, although this effect has not been substantiated. The objective of this study was to compare the activity of the different layers of cervical muscles when performing exercise with these 2 types of apparatus.
SUBJECTS: A total of 19 healthy persons (mean age 28 years, (standard deviation 7 years).
DESIGN: Ultrasound measurements of muscle deformation and deformation rate were recorded from the dorsal and ventral neck muscle layers during extension and flexion exercises. Pulley exercises were performed in the upright sitting position against a standardized resistance (men 2 kg, women 1 kg) and guild board exercises at an angle of 45º.
RESULTS: The dorsal muscles generally showed greater levels of deformation and deformation rate during exercise with the guild board compared with the pulley system (p < 0.05), but with no significant differences in relative activity between the deep and superficial muscle layers (condition × muscle interaction (p > 0.05)). No differences were observed for the ventral muscles between exercise methods (p > 0.05).
CONCLUSION: While both exercise methods appear to train cervical muscle function, neither appear to be more selective in facilitating deep cervical muscle activity, probably as they involve very similar cervical kinematics.
Key words: neck muscles; muscle activity; ultrasonography; exercise.
J Rehabil Med 2013; 45: 00–00
Correspondence address: Anneli Peolsson, NHMRC CCRE (Spinal Pain, Injury and Health), The University of Queensland, St Lucia, QLD 4072, Brisbane, Australia. E-mail: a.peolsson@uq.edu.au; Anneli.Peolsson@liu.se
Accepted Apr 8, 2013; Epub ahead of print Jul 4, 2013
INTRODUCTION
Disability due to neck pain is common; annual prevalence values of up to 65% have been reported in the general population (1). Deficits in strength (2–5), endurance (6, 7) and coordination (8–10) of both the ventral and dorsal cervical muscles are a known feature of chronic neck pain disorders (11). Exercise that facilitates the function of the deep cervical flexor and extensor muscle layers is therapeutically desirable, as these muscles form a deep sleeve that envelopes the cervical vertebral column. Muscles that form this deep sleeve have the appropriate morphology and composition to control segmental cervical motion (12, 13), lordotic orientation (13, 14), and unwanted intersegmental buckling and rotary motion, which can result from contraction of the larger and more superficial cervical muscles (15). Thus, exercises that bias training of the deep cervical muscles are strongly recommended clinically (11, 16, 17), as they have been shown to be impaired in mechanical neck pain (11, 17), and targeted training of their performance has been shown to be of benefit in the clinical management of these disorders (16–18). While many different approaches have been proposed to train the performance of the cervical muscles, 2 common methods used by Nordic physiotherapists for many years include exercise with a guild board or with a pulley system (19).
While performing exercise using guild boards and pulleys (19) has been touted as effective in facilitating the deeper cervical muscle layers, to date, there have been no studies that have investigated cervical muscle usage patterns when performing exercise with these types of apparatus. This information would be valuable when using these types of apparatus, as our previous studies have shown that different methods of exercising the ventral and dorsal cervical muscles can result in varying patterns of activity between the deeper and superficial muscle layers (20–23).
The purpose of this study was to compare the activity of the different layers of cervical muscles when performing exercise with the guild board and pulley system. Specifically, we measured the mechanical activity of the ventral and dorsal neck muscles using an ultrasound method during standardized flexion and extension exercises, respectively, using both guild board and pulley apparatus. We hypothesized first, that both exercise approaches would result in similar activation of the deep muscles. Secondly, that the relative activation of the deep and superficial muscle layers would be similar between exercise methods. These hypotheses are based on the similarity in technique of both exercise methods with regard to cervical kinematics, despite using different apparatus and set-up.
METHODS
Participants
A total of 19 healthy volunteers (10 women and 9 men; mean age 28 years (standard deviation; SD 7), age range 21–48 years) were included in the study after answered advertising for the study at a university. Eighteen of the volunteers were right-handed and one ambidextrous. Participants were included if they reported negligible current neck pain (< 10 mm on the visual analogue scale (VAS) (24, 25) (group mean 0.2 mm (SD 0.5) in the present study), or neck disability (< 20% on the Neck Disability Index (NDI) (26) (group mean 0.7% (SD 0.8) in the present study).
Participants were excluded from the study if they reported a previous history of neck pain for which they had sought treatment, previous trauma to the neck or head, rheumatological or neurological diseases affecting the muscles of their spine or upper quadrant, generalized myalgia, or severe pain in other region of the spine, such as the thorax or lumbar spine. They were also excluded if they had undertaken specific exercises to train the cervical muscles in the previous 6 months. Although eligible participants had not performed specific exercises for their cervical spine they were, on average, physically active, as measured by a physical activity scale (group mean 3.9 (SD 0.2) (out of high level maximum score 4) (27).
All procedures were conducted according to the Declaration of Helsinki. The study was approved by the Regional Ethics Committee and the participants provided written informed consent.
Ultrasound measurements of muscle activity
Ultrasound images of cervical muscles were recorded with a 14.0 MHz linear transducer (38-mm footprint) and Ultrasound Vivid 9 Dimension (GE Healthcare, Horten, Norway) with high frame rate (78 frames/s) operated in B-mode, and a 2D ultrasound imaging system. Images of the dorsal (trapezius, splenius, semispinalis capitis, semispinalis cervicis, multifidus) (Fig. 1AB) and ventral (longus colli, longus capitis, semispinalis capitis muscle) neck muscles were recorded on the right side (dominant side in all participants) of the neck at the C4 vertebral level (identified via the C4 spinous process dorsally and the carotid artery bifurcation ventrally). For both dorsal and ventral recordings, the transducer was first positioned in a transverse orientation at the C4 level to permit identification of the appropriate articular and muscular tissues. Once the correct position was achieved the transducer was rotated 90º to a longitudinal orientation relative to the imaged muscles, which is optimal for ultrasound imaging and speckle tracking analysis. Recording of ultrasound videos were made of the dorsal and ventral muscles during each exercise condition for later analysis.
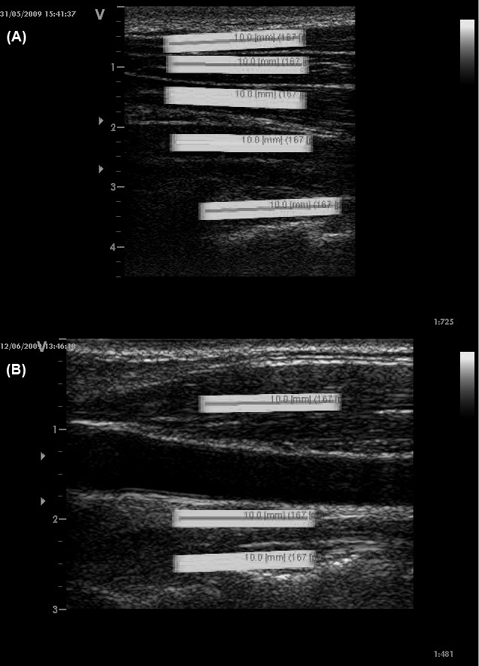
Fig. 1. Longitudinal ultrasound image of (A) dorsal and (B) ventral neck muscles with regions of interest (ROIs; 10 × 2 mm, containing hundreds of measuring points) from superficial to the deep: (A) trapezius, splenius, semispinalis capitis, semispinalis cervicis and multifidus and (B) sternocleidomastoid, longus capitis and longus colli. Each ROI was positioned in the first image (frame) of the video at the mid-point of the muscle belly to avoid facial borders (clear white longitudinal structures in the image).
Speckle tracking analysis. Speckle tracking analysis was performed post-process using the recorded ultrasound movie sequences in AVI format. This process utilizes software to identify and track a distinct pattern of acoustic markers (an interference pattern referred to as a “speckle pattern”), that occurs when muscle tissue is imaged with ultrasound. A region of interest frame (ROI; 10 × 2mm) is positioned over a standardized location within the speckle pattern of each muscle in the first frame (in the resting position) of the video sequence. The ROI tracks its contained unique speckle pattern frame by frame through the movie sequence. The contained speckle pattern changes length with muscle activity, resulting in a change in length of the ROI. The change in the ROI length is measured as muscle deformation and 2 measures are extracted. The muscle deformation measure is calculated as the percentage change in the longitudinal median length variation of the ROI compared with that at rest (expressed as % strain). The muscle deformation rate measure is expressed as deformation per time unit (% strain 1/s).
The technique of speckle tracking analysis utilizes research software containing a speckle tracking algorithm based on a stable mathematical model (Farneback). The calculating algorithm tracks the ROI (containing the unique speckle pattern) and measures deformation of each ROI in each frame sequentially, comparing it with its length in the initial resting movie frame. This software is dependent on at least 80% agreement of the speckle pattern between each frame of the movie for the ROI to be positively identified (28).
It was ensured that the ROI representing each muscle was located in a standardized position between participants. For each muscle the ROI was positioned at the midpoint of the muscle belly and orientated longitudinal to the muscle fibres. In each video sequence the optimal position of the ROI was checked by observing the video sequence in slow motion with the ROIs in situ. This process ensured that each ROI was recognized by the measurement software, and that there was no interference between different ROI frames during the video sequence. Once the investigator was satisfied with the location of each ROI the analysis was performed using the software.
These ultrasound measurements have been shown to have moderate to excellent test-retest reliability both for dorsal (2-way random absolute agreement single measure intra-class correlation coefficient (ICC) 0.61–0.99) and ventral (ICC 0.80–0.99) neck muscles (28, 29). The deformation measurement has been reported to be reproducible by Lopata et al. (30) and to be correlated with electrical stimulation with electromyography (EMG) and voluntary muscular contraction (30).
Exercise conditions
Guild board exercises. The participant reclined on the Guild board, which was positioned at an angle of 45º to the horizontal and attached to wall bars (Fig. 2A and B). For the ventral neck muscle exercise, participants reclined on their back with their head supported so that their lower cervical spine was in a neutral position and the upper cervical spine in slight flexion. The exercise required the participant to lift the torso from guild board en bloc from the pelvis, while maintaining a static head and neck orientation against gravity. For the dorsal neck muscles exercise, participants were positioned in prone with their forehead supported with the cervical spine and head in the same orientation at rest as for the ventral muscle exercise. The exercise required the participant to extending the torso from the pelvis, while maintaining a static head and neck orientation against gravity.
Pulley exercises. The participant sat upright on a bench so that their cervical spine was in a neutral position and the upper cervical spine in slight flexion (Fig.2C and D). A leather strap was fixed to the head just above the ears and attached to a weight. A standardized load was used for all participants (men 2 kg, women 1 kg). This load was selected because it was considered relatively equivalent to the exercise resistance provided by gravity during the guild board exercises (performed at 45º). For the ventral muscle exercise, participants faced away from the pulley and flexed their trunk en bloc from the pelvis, while maintaining a static head and neck orientation against the resistance of the pulley system. For the dorsal muscle exercise, participants faced the pulley and extended their trunk en bloc from the pelvis, while again maintaining a static head and neck orientation against the resistance of the pulley system.
The same instructions and trunk movement were used for both exercise conditions (guild board and pulley), the difference being the starting position and apparatus used. Participants were given standardized instructions by the researcher: “I will count to 3, and on 3 start the exercise gently, holding the neck still in line with the body (keeping your chin down), and slowly bend from the hips so that your trunk and head lifts off the supporting surface (guild board)/away from the pulley. Hold the position for 1 s and lower to the starting position.”
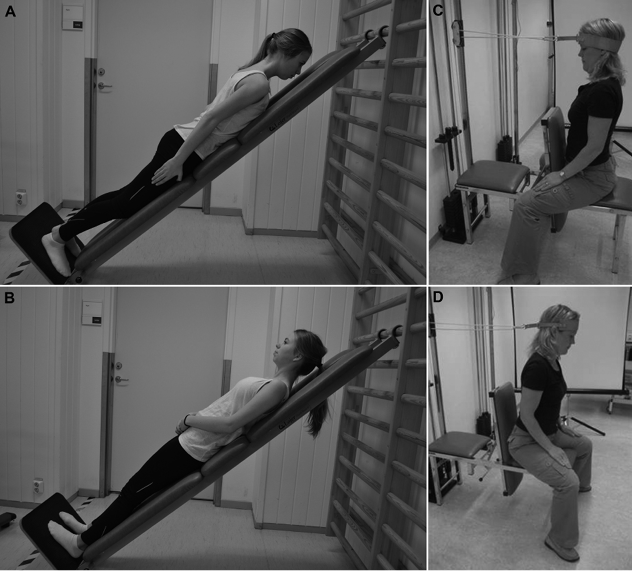
Fig. 2. Exercise technique for (A) dorsal and (B) ventral neck muscles on the guild board and exercise technique for (C) dorsal and (D) ventral neck muscles in the pulley. The figures are published with permission from the person.
Procedure
For each of the 4 experimental conditions (ventral and dorsal muscle exercises on the guild board and the pulley system) all participants performed 2 repetitions as a warm-up and familiarization before performing the experimental exercise. During each exercise, a researcher recorded the ultrasound imaging and saved the image sequences (“videos”) for post-processing speckle tracking analysis and calculation of the deformation and deformation rate measurements. Recordings for each condition commenced at rest with no resistance (the reference analysis video frame), and then continued as the participant performed the exercise against the resistance (gravity for the guild board exercise and the standard weights for the pulley system exercise). Participants were instructed to cease the testing procedure if they experienced any neck symptoms.
Data management and statistical analysis
Measurements of muscle deformation and deformation rate were calculated from the ultrasound video sequences of the experimental exercise conditions, and all values were expressed as the root mean square (RMS) over the duration of the exercise condition. The RMS values are based on the curve of the changes in deformation and deformation rate in the longitudinal ultrasound projection over the entire exercise sequence.
Analyses were performed using a statistical package (SPSS version 20: IBM). A repeated measures general linear model was used to evaluate main effects for exercise (guild board, pulley system) as well as exercise × muscle interactions for the deformation and deformation rate measurements. Separate analyses were conducted for the ventral and dorsal neck muscles. Post-hoc tests of simple effects were performed when indicated. Statistical significance was accepted at the 0.05 alpha level.
RESULTS
Data for the measures of deformation and deformation rate of the dorsal and ventral neck muscles for all experimental exercise conditions are shown in Tables I and II, respectively.
Dorsal neck muscles
For the measurement of muscle deformation there was a significant main effect of exercise condition (p = 0.01), but no exercise × muscle interaction (p > 0.51). Exploratory tests of simple effects revealed significantly greater deformation for the splenius capitis (p = 0.03) and semispinalis cervicis (p = 0.01) muscles during the guild board compared with the pulley exercise (Table I). Analysis of muscle deformation rate revealed a significant main effect of exercise condition (p = 0.02), but no exercise × muscle interaction (p = 0.22). Tests of simple effects revealed significantly greater deformation rate for the semispinalis cervicis (p = 0.04), and multifidus (p = 0.02) muscles during the guild board compared with the pulley exercise (Table I).
|
Table I. Descriptive statistics (mean values and standard deviations (SD) of root mean square) for dorsal and ventral neck muscle deformation (strain) (%) and deformation rate (% deformation/s) measurements during the 2 different exercise (guild board and pulley system) methods |
||||||
|
Muscle |
Deformation (%) |
Deformation rate (%/s) |
||||
|
Pulley Mean (SD) |
Guild board Mean (SD) |
Pulley Mean (SD) |
Guild board Mean (SD) |
|||
|
p-value |
p-value |
|||||
|
Dorsal |
||||||
|
Trapezius |
2.45 (2.78) |
4.09 (6.07) |
0.13 |
0.007 (0.005) |
0.012 (0.013) |
0.06 |
|
Splenius capitis |
3.24 (4.82) |
4.82 (5.04) |
0.03 |
0.012 (0.01) |
0.017 (0.015) |
0.06 |
|
Semispinalis capitis |
3.78 (2.97) |
7.26 (8.96) |
0.1 |
0.015 (0.014) |
0.024 (0.027) |
0.18 |
|
Semispinalis cervicis |
2.93 (2.00) |
4.67 (3.15) |
0.01 |
0.013 (0.008) |
0.024 (0.025) |
0.04 |
|
Multifidus |
3.16 (2.48) |
6.43 (7.68) |
0.06 |
0.011 (0.006) |
0.026 (0.029) |
0.02 |
|
Ventral |
||||||
|
Sternocleidomastoid |
6.3 (5.14) |
6.96 (5.33) |
0.02 |
0.018 (0.007) |
0.025 (0.009) |
0.22 |
|
Longus capitis |
7.18 (5.07) |
8.98 (7.2) |
0.72 |
0.026 (0.018) |
0.031 (0.014) |
0.69 |
|
Longus colli |
7.26 (5.18) |
7.34 (3.73) |
0.89 |
0.032 (0.027) |
0.037 (0.016) |
0.75 |

Ventral neck muscles
There were no significant main effects for exercise condition for either the deformation (p = 0.34) or deformation rate (p = 0.22) measurements for the ventral muscles. Similarly, there were no significant exercise × muscle interactions for the deformation (p = 0.72) or deformation rate (p = 0.73) measurements (Table I).
DISCUSSION
The first hypothesis of this study was not fully supported, with some differences observed in deep muscle activity (deformation, deformation rate) during the 2 different exercise methods, but only for the dorsal and not the ventral muscles. Greater levels of muscle deformation as well as deformation rate were observed when exercising the dorsal neck muscles with the guild board compared with the pulley method in the deeper semispinalis cervicis and cervical multifidus muscle layers. While this study found that the exercise performed on the guild board may facilitate greater deep dorsal muscle activity compared with the pulley exercise, there is no support for greater selective activity of the deep muscles relative to the more superficial muscles. The observed greater activity levels of the deeper dorsal muscle layers during the guild board exercise compared with the pulley exercise coincided with greater levels of activity of some of the superficial muscles, such as the splenius capitis and trapezius muscles. These findings explain the lack of significant exercise condition by muscle interactions observed in this study and support our second hypothesis. The exercise approaches despite their different modes of resistance (gravity vs weights) show similar relative activity of the deep and superficial muscle layers, which is probably attributable to their similar static positioning of the mid/lower cervical spine (neutral) and upper cervical spine (in slight flexion) during the exercise.
We have shown previously that a factor that influences the interaction between the activity of the deep and superficial cervical muscle layers during exercise of the neck is the relative kinematics of the upper and mid/lower cervical spine during the performance of exercise (21–23). Specifically, performing an extension exercise with the upper cervical spine in extension induces significantly greater activity of the superficial semispinalis capitis muscle than performing the same exercise in a neutral upper cervical orientation (23). This is probably due to the attachment of the semispinalis capitis muscle to the head and its subsequent capacity to exert extensor moments to the upper and lower cervical regions (23). On a similar anatomical basis it has been shown that performing a cervical flexion exercise with the upper cervical spine in flexion is more facilitatory of deep cervical flexor muscle activity compared with performing it in a neutral upper cervical orientation (22), and that exercise that combines upper and lower cervical flexion induces far greater activity of the superficial flexor muscles than upper cervical flexion alone (21, 22). On this basis it is not surprising that the relative muscle usage patterns of the deep and superficial muscle layers were similar for the 2 exercises performed in this current study, as both had identical kinematics of the mid/lower and upper cervical spine during their performance.
Exercise performed with the guild board resulted in generalized elevated levels of deformation and deformation rate of the dorsal muscles (but not the ventral muscles) compared with the pulley system, despite attempts to make the relative loads between the exercises similar. One factor may be the significant difference between the relative strength of the ventral and dorsal neck muscles. The dorsal muscles are substantially stronger (nearly twice as strong) than the ventral neck muscles consistent with their larger size (31). Perhaps a reason for the discrepancy may have been a mismatch between the relative challenge imposed on the flexor and extensor muscles. Notwithstanding this, the comparison in this study was made between exercise conditions (guild board, pulley), within muscles groups separately (ventral and dorsal), and therefore theoretically each muscle group should have been challenged under a similar load between exercise conditions. Future studies, however, will have to compare the effect of different load on muscle usage during these exercise approaches, as we have shown previously that load intensity of exercise can affect the relative activity of the different layers of cervical muscles (21).
There are other limitations to this study. Findings can only be extrapolated to healthy individuals; however, in this initial study we wanted to see what the “normal” muscle usage response was between these 2 different exercises. Future studies will need to assess the muscle response in individuals with neck pain who are most likely to be prescribed these exercises, to determine if the muscle response is different to that observed in this study. This will be important, as individuals with neck pain have been shown to have altered muscle performance between muscle layers compared with healthy people (1–10, 32, 33). There are also some technical limitations in this study. Firstly, our 2D ultrasound method was only able to measure longitudinal muscle deformation during muscle contraction, with no capacity to measure any rotational components of muscle motion. Secondly, we could not account for individual anatomical variations in muscle properties (anatomical architecture and position) which may affect results, but this issue should be minimal as the same volunteers were investigated for both exercises. Notwithstanding this, there is evidence of a positive relationship between the magnitude of muscle deformation (recorded with Speckle Tracking analysis) and the magnitude of muscle activity using other measurements (force, progressive electrical stimulation, electromyography) providing justification for the use of the measurements performed in this study (30).
In conclusion, this study compared the muscle activity of the ventral and dorsal neck muscles during exercise performed with a guild board and pulley system. The response to exercise between the exercise conditions was similar for the ventral muscles, while muscle activity (as inferred by measures of muscle deformation and deformation rate) of the dorsal muscles was generally greater during the guild board exercise for both the deeper and more superficial dorsal muscle layers. While both exercise methods appear to be legitimate approaches to training cervical muscle function, neither approach appears to be more selective in facilitating deep cervical muscle activity. Future studies will need to explore the effect of different relative load/resistance on muscle usage patterns of these 2 exercise methods.
ACKNOWLEDGEMENTS
The study is financially supported by the Swedish Medical Research Council, the Wenner-Gren foundations and a Health Practitioner Research Fellowship (Queensland Health and University of Queensland (NHMRC CCRE Spinal Pain, Injury and Health)).
The authors declare no conflicts of interests.
REFERENCES

