Eva Ekvall Hansson, PT, PhD1, Liselott Persson, PT, PhD2 and Eva Maj Malmström, PT, PhD3
From the 1Lund University, Department of Clinical Sciences/Family Medicine, Malmö, 2Department of Health Sciences, Division of Physiotherapy, Lund University and 3Rehabilitation Medicin & ENT, Skåne University Hospital, Lund, Sweden
OBJECTIVE: To describe how vestibular rehabilitation influences pain and range of motion among patients with whiplash-associated disorder and dizziness, and to describe whether pain or range of motion correlated with balance performance or self-perceived dizziness handicap.
SUBJECTS: A total of 29 patients, 20 women and 9 men, age range 22–76 years.
METHODS: Patients with whiplash-associated disorder and dizziness were randomized to either intervention (vestibular rehabilitation) or control. Neck pain intensity, cervical range of motion (CROM), balance and self-perceived dizziness handicap were measured at baseline, 6 weeks and 3 months.
RESULTS: There were no differences in neck pain intensity or CROM between the 2 groups either at baseline, 6 weeks or 3 months (p = 0.10–0.89). At baseline, neck pain intensity correlated with CROM (–0.406) and self-perceived dizziness handicap (0.492). CROM correlated with self-perceived dizziness handicap and with 1 balance measure (–0.432). Neck pain intensity did not correlate with balance performance (–0.188–0.049).
CONCLUSION: Neck pain intensity and CROM was not influenced by vestibular rehabilitation. Importantly, the programme did not appear to increase pain or decrease neck motion, as initially thought. Neck pain intensity and CROM correlated with self-perceived dizziness handicap. CROM also correlated with 1 balance measure.
Key words: whiplash; dizziness; self-perceived handicap; vestibular rehabilitation; neck pain; cervical range of motion.
J Rehabil Med 2013; 45: 00–00
Correspondence address: Eva Ekvall Hansson, Lund University, Department of Clinical Sciences in Malmö/Family Medicine, Jan Waldenströms gata 35, SE-205 02 Malmö, Sweden. E-mail: eva.ekvall-hansson@med.lu.se
Accepted Apr 8, 2013; Epub ahead of print Aug 8, 2013
Introduction
The upper cervical region has an important role in postural control, via the direct access to the vestibular nuclear complex and the reflex centre for coordination between vision and neck movement (1). In addition, disorder of the cervical region influences vestibular reactions (2), which might be a possible cause of symptoms such as dizziness among patients with whiplash-associated disorders (WAD) (1). Patients with WAD and dizziness have shown greater deficits in postural response, both compared with healthy controls and compared with patients with WAD but without dizziness (3).
Dizziness has been reported as the most common symptom after neck pain among patients with WAD (4). Symptoms of postural control disturbances have also been known as a probable cause of poorer prognosis among these patients (5, 6).
In 2006, our research group performed a randomized controlled trial for patients with WAD and dizziness as a pronounced symptom. Therefore, the intervention addressed dizziness and comprised a vestibular rehabilitation programme. We found that the intervention group improved their balance and their self-perceived dizziness handicap, significantly more than the control group (7). However, at that time the correlation between dizziness and neck pain among patients with WAD were not the focus of study. It was postulated at that time that the vestibular rehabilitation programme might increase pain and decrease range of motion in the neck, but we were not aware of the opposite possiblity, that the intervention might influence neck pain and range of motion in a positive way. Therefore, we measured these variables but, as pointed out by other authors (6), we did not describe them in our results.
The aim of the present paper was therefore to describe how vestibular rehabilitation influenced pain and cervical range of motion among patients with WAD and dizziness as a pronounced symptom. We also wanted to describe whether neck pain intensity or cervical range of motion correlated with balance performance or self-perceived dizziness handicap.
Material and methods
Patients
Patients were recruited from general practitioners and physiotherapists in primary healthcare, orthopaedic physicians in private practice, administrators of rehabilitation at the regional social insurance office and the orthopaedic hospital clinic all in Malmö, Sweden during a period of 2.5 years, as described in a previous paper (7). Criteria for inclusion in the study were a history of whiplash and dizziness reported as 1 of the main symptoms. Patients with benign paroxysmal positional vertigo were excluded. A total of 29 patients met the inclusion criteria of the study. Sixteen patients were randomized to the training group and 13 to the control group. There were 8 drop-outs in the training group and 3 in the control group (Fig. 1). At baseline, 28 of the 29 patients had neck pain and musculoskeletal symptoms and 1 patient also had sensory deficits. Twenty patients had been dizzy since the accident, 5 since 1–2 weeks and 4 since approximately 6 months after the accident. Thirteen patients described dizziness as unsteadiness (45%), 9 as rotational or spinning sensation (31%), 5 patients as both and 1 patient as other type of dizziness. Five patients also underwent other types of individually adapted physiotherapy during the study period. Factors that aggravated dizziness were head and neck movements (9 patients), neck pain or headache (6 patients), strain (5 patients), visual and hearing impressions (3 patients), fatigue (2 patients) and travelling by car, rail, and underground or by air (2 patients). The time since accident varied from 6 months to 15 years (median 1 year). Fifteen subjects were working, 9 were on sick leave or retired.
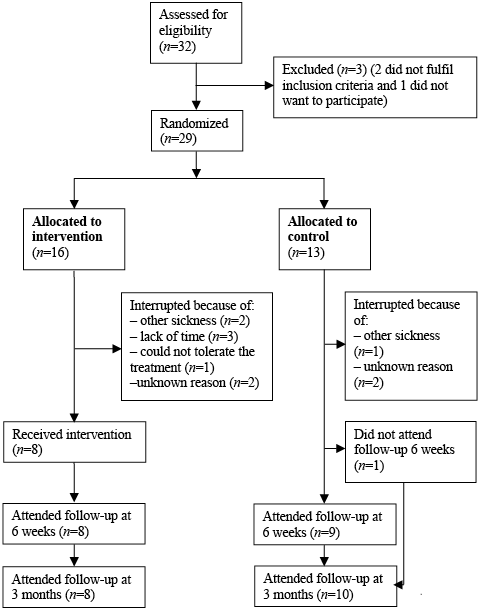
Fig. 1. Study flow-chart.
Initial assessment included anamnesis, statements of neck pain intensity, examination with balance performance measures and cervical range of motion (CROM), the Dix-Hallpike manoeuvre (8) and the Dizziness Handicap Inventory (DHI) (9). After assessment, the patients were randomized, by an independent person using a random number table, into either an intervention group or a control group. The same independent person also carried out the intervention. All assessments were performed by one of the authors (EEH), who was blind to the randomization (Fig. 1).
Measures
All patients were assessed at baseline, 6 weeks (directly after intervention) and 3 months (after baseline).
Neck pain intensity was measured, using a visual analogue scale (VAS) (10, 11). The patients were asked “How severe has your neck pain been the last week?” and estimated their answer on a 100-mm line, with no marks on it. Their answers were measured in mm.
CROM was measured with Myrin© goniometer (12, 13) in the directions flexion, extension, lateral flexion and rotation. One movement with the largest possible range was performed in each direction.
Four different balance measures, both static and dynamic, were performed. Static balance was measured using tandem standing and standing on one leg. The time the subject was able to maintain each position, up to 30 s, was measured. Tandem standing was performed with eyes open and with eyes closed, with preferred foot in back (14–16). Standing on one leg was performed for 30 s with eyes open (SOLEO) and standing on one leg eyes closed (SOLEC) (16, 17). In SOLEO and SOLEC, both left and right legs were tested and the results were averaged. In each test, 3 trials were allowed and the best result was used.
Dynamic balance was measured using the tests walking in a “figure-of -8” (18), and “walking heel to toe on a 5-m line” (14). The number of steps outside the figure-of-8 and the number of steps outside the line were counted.
To establish the level of self-perceived dizziness handicap, a Swedish version of the DHI was used (19, 20). The inventory comprises 25 different items, organized in 3 different dimensions: functional, emotional and physical. The total maximum score is 100 points: 32 points for the functional dimension; 40 points for the emotional dimension; and 28 points for the physical dimension. The higher the score, the greater the level of self-perceived dizziness handicap.
Intervention
The intervention comprised a vestibular rehabilitation programme, held at group sessions in a physiotherapy centre, for approximately 50 min, twice a week for 6 weeks. The programme started with a warm-up phase. This was followed by exercises aimed to stimulate the vestibular system, using eye, head and trunk movements (Table I). The patients were instructed to perform all exercises with optimal postural alignment. Patients, who were randomized to the intervention group, were consecutively allocated to the vestibular rehabilitation programme.
The control group was tested at the same intervals as the intervention group, but received no intervention. However, after assessment at 3 months, the patients in the control group were offered the same training as the intervention group. Both groups continued with earlier initiated treatments.
|
Table I. Intervention programme |
|
|
Warm-up phase |
10 min: walking around in the room and changing direction, as well as turning the head from side to side. Exercises in standing, including training of co-ordination of movements. |
|
Circuit training 2 min for each exercise and 2 laps in the circuit |
Walking forward and backwards on a slope while turning the head from side to side. Standing up and sitting down on a chair while turning the head from side to side. Closed eyes if possible. Standing on a trampoline, eyes closed and slightly flexing the knees and turning the head from side to side simultaneously. Standing on 10 cm foam with eyes closed and turning the head from side to side. Standing on a sport mat, walking on the spot and turning the head from side to side. Closed eyes if possible. Sitting on a ball, feet on foam, eyes closed and bouncing slightly while turning the head from side to side. Walking forward and backward while turning the head from side to side. |
|
Recovery phase |
5 min: soft, relaxing movements. Stretch of the muscles in the upper cervical region. |
Statistical analysis
Considering a standard deviation (SD) of 13.3 for SOLEO and 7.4 for SOLEC and a clinically relevant difference of 1.5 for SOLEC, and a SD of 23 and clinically relevant difference of 18 for DHI (9, 21–23), a power of 80% and a significance level of 0.05, a sample size of 40 persons was required (24). However, due to technical reasons, recruitment had to be terminated after 2.5 years, resulting in a final sample size of 29 subjects.
Since the sample was small (fewer than 20 persons in each group), Mann-Whitney U was used to test for differences between the groups and 95% confidence intervals were calculated for the median differences. The results was analysed on an intention-to-treat basis, using the last observation carried forward (25). An on-treatment analysis was also performed for comparison. Correlations were calculated using Spearman’s rank correlation (24)
The data package SPSS version 18.0 was used (SPSS Inc., software location Lund University).
Ethics
The study was approved by the ethics committee of Lund University, registration number LU 702-01.
Results
Neck pain intensity (measured with VAS) at baseline was, on average, reported as severe with a wide spread for both groups (Table II). Both groups reported similar neck pain 6 weeks after the intervention, but the intervention group reported lower pain intensity values at the 3 months follow-up (Table III). There were no statistical significant differences between the groups at either 6 weeks or 3 months (p = 0.10–0.89).
|
Table II. Baseline measures for the whole group, the intervention group and the control group. p-values for difference between intervention group and control group |
||||
|
Measure |
All (n = 29) Median (min–max) |
Intervention (n = 16) Median (min–max) |
Control (n = 13) Median (min–max) |
p-value |
|
VAS pain, mm |
60 (14–100) |
60 (14–91) |
60 (36–100) |
0.47 |
|
Flexion, ° |
32 (15–70) |
30 (15–70) |
35 (15–60) |
1.00 |
|
Extension |
40 (10–80) |
45 (25–80) |
40 (10–65) |
0.15 |
|
Lateral flexion |
60 (30–95) |
60 (40–95) |
50 (30–95) |
0.39 |
|
Rotation |
102 (25–170) |
105 (65–170) |
90 (25–135) |
0.31 |
|
Total CROM |
232 (80–385) |
245 (175–385) |
200 (80–305) |
0. 32 |
|
Age, years |
40 (22–76) |
40 (22–73) |
43 (23–76) |
0.45 |
|
Women/men, n |
20/9 |
10/6 |
10/3 |
0.53 |
|
VAS: visual analogue scale; Total CROM: all cervical range of motion measures added together. |
||||
CROM was reduced for most patients at baseline, with considerable spread, without any significant differences between the groups (Table II). The intervention group had improved CROM in flexion both at 6 weeks and at 3 months and in rotation at 3 months. The differences was not statistically significant (p = 0.52, 0.79 and 0.44, respectively). The control group had improved in rotation at 3 months (p = 0.09). There were no statistically significant differences between the groups in change from baseline to 6 weeks or 3 months follow-up (Table III).
|
Table III. Intention to treat analysis of differences from baseline to 6 weeks and 3 months. Median values and (95% CI) for the median difference in change and statistical significance of the difference between the groups |
|||||||||||
|
Measure |
Baseline |
6 weeks |
3 months |
||||||||
|
Intervention (n = 16) Median |
Control (n = 13) Median |
p-value |
Intervention (n = 16) Median |
Control (n = 12) Median |
95% CI |
p-value |
Intervention (n = 16) Median |
Control (n = 13) Median |
95% CI |
p-value |
|
|
VAS pain, mm |
60 |
60 |
0.47 |
64 |
62 |
0.0–1.0 |
0.35 |
42 |
61 |
0.0–6.0 |
0.18 |
|
CROM, ° |
|||||||||||
|
Flexion |
30 |
35 |
1.00 |
45 |
30 |
0.0–10.0 |
0.22 |
47 |
30 |
0.0–10.0 |
0.10 |
|
Extension |
45 |
40 |
0.15 |
40 |
30 |
0.0–0.0 |
0.79 |
40 |
25 |
0.0–0.0 |
0.82 |
|
Rotation |
105 |
90 |
0.31 |
105 |
88 |
0.0–20.0 |
0.49 |
110 |
95 |
0.0–20.0 |
0.89 |
|
Lateral flexion |
55 |
45 |
0.31 |
35 |
20 |
–5.0–0.0 |
0.43 |
38 |
20 |
0.0–5.0 |
0.29 |
|
Total |
245 |
200 |
0.16 |
245 |
198 |
0.0–25.0 |
0.83 |
250 |
207 |
0.0–40.0 |
0.82 |
|
VAS: visual analogue scale; CROM: cervical range of motion; CI: confidence interval. |
|||||||||||


Data on balance measures and self-perceived dizziness handicap have been presented in an earlier study (7).
At baseline, neck pain intensity correlated to DHI total, DHI emotional scale and DHI physical scale, but did not correlate with any of the balance measures (Table IV). CROM correlated at baseline with DHI total, DHI functional scale, DHI physical scale and with tandem standing, eyes open (Table IV).
|
Table IV. Correlations between baseline measures of neck pain intensity, cervical range of motion, self-perceived dizziness handicap and balance |
|||
|
Measure |
VAS pain |
Total cervical range of motion |
|
|
DHI total |
0.492** |
–0.431* |
|
|
DHI functional |
0.291 |
–0.489** |
|
|
DHI emotional |
0.599** |
–0.321 |
|
|
DHI physical |
0.412* |
–0.519** |
|
|
Balance measures |
|||
|
Tandem Romberg eyes open |
–0.188 |
0.417* |
|
|
Tandem Romberg eyes closed |
–0.070 |
0.220 |
|
|
SOLEO |
–0.137 |
0.280 |
|
|
SOLEC |
0.049 |
0.054 |
|
|
Figure-of-8 |
–0.071 |
–0.059 |
|
|
Walking heel to toe |
–0.087 |
–0.002 |
|
|
*p < 0.05. **p ≤ 0.01. VAS: visual analogue scale; DHI: Dizziness Handicap Inventory; SOLEO: Standing One Leg Eyes Open; SOLEC: Standing One Leg Eyes Closed. |
|||
Discussion
In this study, neck pain intensity and CROM correlated with DHI and CROM also correlated with one balance measure. Neither neck pain intensity nor CROM per se were significantly influenced by vestibular rehabilitation. This was despite the fact that balance performance and self-perceived dizziness handicap was improved by vestibular rehabilitation for this group of patients, as reported previously (7).
The power calculation gave a sample size of 40 persons, which we were not able to include, due to practical reasons. When discussing the results of this study, the small sample size and the total number of 11 drop-outs has to be considered. Since there are more improvements in the intervention group (flexion and VAS as well as rotation and total CROM) than in the control group (only rotation and total CROM), albeit not statistical significant, we suspect that a study with a larger sample size might support the findings in our study. Patients with WAD are exposed to stressful situations due to the whiplash trauma (26), which makes them a vulnerable group. One might assume that dizziness as an additional symptom increases this vulnerability, which might explain the considerable amount of dropouts in the intervention group. Drop-outs could also be explained by the fact that some patients realized their need for a broader intervention, addressing other symptoms besides dizziness.
The improvement in mobility in flexion for the intervention group may partly be explained by a better posture (27). Vestibular rehabilitation probably improved orientation and the ability to stabilize gaze during motion/gait with less need for a flexed posture. This could also explain the relative reduced extension after intervention, since a changed posture could impact on the proportion between flexion-extension. Still, this cannot explain the whole improved flexion performance. However, when dizziness and balance deficits are reduced the neck can be moved more freely. In addition, 4 of the patients had been dizzy since 6 months after the accident. This type of dizziness might be due to sensory mismatch, since other dizziness measures were negative. Sensory mismatch might develop due to increased sensitivity (1).
To control for bias the same test protocol was used for all patients, with the same person performing all the measures (blinded to the randomization), and with an independent person performing the randomization procedure and the intervention. During the actual period we did not control for other interventions besides the intervention in the study. The patients were not explicitly asked to stop other treatments, medication or physiotherapy, which means treatment as usual could continue.
The main focus of this study was to elucidate the role of vestibular rehabilitation for patients with WAD, addressing symptoms of neck pain and mobility deficits. As shown in a previous study, balance performance and self-perceived dizziness handicap can be improved by vestibular rehabilitation (7), and this has also been demonstrated by others (28). The correlation between neck pain, CROM and DHI suggest that pain and dizziness probably interacts, giving comorbidity, with prerequisites for the symptoms to enhance each other. Since neck pain correlated both with DHI total, as well as with DHI emotional and physical, the results elucidate the importance of decreased neck pain for the experience of self-perceived dizziness handicap among patients with WAD. The significant mild correlation between decreased CROM and tandem standing also elucidates the importance of good mobility for postural control, as previously shown (29). The correlation between neck pain and dizziness both advocate further studies of the interaction between postural control and neck pain among patients with WAD, as well as consideration of both these symptoms in clinical practice. In addition, the combination of vestibular rehabilitation, therapies for reducing neck pain, normalizing range of motion and promoting sensorimotor control within clinical reasoning require further research (28).
In conclusion, neck pain intensity and CROM did not seem to be influenced by vestibular rehabilitation among this group of patients. Importantly, the programme did not appear to increase pain or decrease neck motion, as initially thought. Neck pain intensity and CROM correlated with self-perceived dizziness handicap, and CROM also correlated with one balance measure.
References

