Vanja E. Nyberg, RPT, PhD1, Mehmed Novo, MD, PhD1 and Bengt H. Sjölund, MD, DMSc2
From the 1Department of Rehabilitation Medicine, Community Medicine and Rehabilitation, Umeå University, Umeå, Sweden and 2Department of Public Health, University of Southern Denmark, Odense, Denmark
OBJECTIVES: To determine whether coping profile changes after rehabilitation, assessed with the Multidimensional Pain Inventory (MPI), can predict which persons disabled by chronic musculoskeletal pain will be in receipt of sick leave benefits in the long term.
METHODS: Study of MPI data from 2,784 patients (709 men and 2,075 women) collected from the Swedish Quality Register for Pain Rehabilitation (SQRP) before and at the end of rehabilitation and compared with independent sick leave data for 1 year later.
RESULTS: After rehabilitation there was a significantly decreased share of Dysfunctional profiles (DYS) among both men (44% before, 31% after) and women (39% before, 26% after), but an increased share of Adaptive Coper profiles (men 15% before, 24% after, women 14% before, 24% after). The number of patients on full-time sick leave decreased significantly among men (from 57% to 46%) and women (from 57% to 50%). Persons with a DYS profile after rehabilitation had a low probability of having no or part-time sick leave.
CONCLUSION: The number of persons with DYS profiles decreased after rehabilitation. Those with other profiles had less full-time sick leave 1 year later than those with DYS profiles, indicating that leaving the DYS profile is a positive prognostic sign long-term. Furthermore, the gender differences observed suggest the need to tailor rehabilitative strategies differently for men and women.
Key words: chronic musculoskeletal pain; disability; sick leave benefits; rehabilitation; Multidimensional Pain Inventory.
J Rehabil Med 2014; 46: 00–00
Guarantor’s address: Vanja Nyberg, Umeå University, Rehabilitation Medicine, Building 9A, SE-901 87 Umeå, Sweden. E-mail: vanja.nyberg@rehabmed.umu.se
Accepted May 13, 2014; Epub ahead of print Aug 22, 2014

This article has been fully handled by one of the Associate Editors, who has made the decision for acceptance, as the Editor-in-Chief is a co-author.
Introduction
Disability due to chronic pain includes negative social consequences in the form of increased sick leave (approximately 30% of all sick leave in Sweden) (1), activity limitations and reduced participation in society (2). The economic costs of chronic pain in Sweden were estimated at around 9.9 billion € in 2006 (1). Chronic pain also results in substantial problems, such as depression, anxiety, fatigue, and difficulties in maintaining relationships (3). Thus, there is a need to provide effective and evidence-based rehabilitation for these conditions. Controlled studies show that cognitive-behavioural-oriented multidisciplinary rehabilitation has a positive impact, particularly in terms of functioning on activity levels, but the effect on working ability varies (1, 4, 5). However, a recent meta-analysis based on 5 studies from Scandinavia verified the evidence for a clinically relevant effect of multidisciplinary interventions on return to work (6).
Whereas the prevalence of pain in the Scandinavian population is approximately the same among men and women (7), as confirmed by a recent European survey by Breivik et al. (8) (56% women reporting pain vs 52% women in the population), Bergman and his co-workers (9), in a large epidemiological study of musculoskeletal pain, found that females have an increased risk of chronic widespread pain. Furthermore, in a study examining 1,400 consecutively referred patients for pain management, two-thirds were women (10). This difference in prevalence between men and women may be due to sample differences, e.g. normal population vs patients. Several studies have reported gender differences with respect to various pain-related items in patients with chronic pain (11). Gender differences have also been reported to have a major influence on the results of treatment of patients with chronic musculoskeletal pain (12, 13), although some have found no gender difference in treatment outcome (14).
The Multidimensional Pain Inventory (MPI) (15) is a widely used questionnaire for describing chronic pain and its consequences, exploring the various dimensions involved in the experience of chronic pain (16, 17). In addition, the MPI has proven clinically useful in identifying specific psychosocial profiles or patterns of response among individuals with chronic pain. The MPI is a self-report questionnaire that yields 9 empirically derived scales: Pain severity, Interference, Life control, Affective distress, Social support, General activity, and 3 scales measuring the patient’s perception of the responses by significant others to displays of pain and suffering: punishing, solicitous and distracting responses. From these scales, using the algorithm calculated according to the multivariate discriminate model, 3 primary psychosocial coping profiles have been derived by Turk & Rudy (17): Dysfunctional (DYS) patients with high pain impact, affective distress, and severe functional limitations; Interpersonally Distressed (ID) patients with poor social support by their significant others in response to pain; Adaptive Coper (AC) patients with low pain impact and high levels of functional activity. In addition to the primary patient subtypes, patient profiles can be classified as “non-prototypic” under certain conditions: Hybrid profiles are those that share features with more than one prototypic subtype; Anomalous profiles are those that are significantly different from all 3 prototypic MPI group profiles; and Unanalyzable those that are missing more than 2 of the scale scores used to assign them to a cluster.
Some earlier studies have shown that having a DYS profile is associated with a higher level of sickness absence and disability pension compared with those with AC or ID profiles (18, 19).
In a previous registry study (20) we found that individuals who reported a decrease in MPI scales scores for the scales “Pain severity” and “Interference” immediately after the pain rehabilitation programme decreased their risk of being on full-time sick leave one year later. The present exploratory study was carried out to analyse whether changes in MPI profiles for participants, which occurred during the rehabilitation programme were associated with changes in the sick leave situation one year later, and if gender influenced these changes.
Material and Methods
Data collection
The present study was a retrospective observational register study carried out on national data collected for auditing purposes in the Swedish quality registry for pain rehabilitation (SQRP) (21). During the monitoring period (2003–2007), MPI data from consecutive SQRP questionnaires before and after varying rehabilitation measures were collected from 8,509 patients (2,558 men and 5,951 women). Patients were assessed at 19 pain rehabilitation units across Sweden. We chose the year 2007 as the end-point to make possible a reasonable comparison with individual sick leave data from the Swedish Social Insurance Agency Central Registry one year after completed rehabilitation, since sick leave regulations in Sweden changed in 2008, introducing new sick leave time period limitations.
Participants
All patients included in the study had chronic musculoskeletal pain with symptom diagnoses only. They were referred for rehabilitation from their general practitioner or from an organ specialist, usually an orthopaedic surgeon or a rheumatologist. At the rehabilitation units, the patients were examined by multidisciplinary assessment teams to assess whether entering a pain rehabilitation programme was feasible. The team consisted of a physical and rehabilitation medicine (PRM) or Public Health physician, a licensed physiotherapist, a social worker and, usually, a cognitively-behaviourally oriented psychologist; sometimes an occupational therapist. A total of 2,865 patients (746 men, 2,119 women) were assessed as being able to benefit from cognitive-behaviourally oriented multidisciplinary pain rehabilitation of 3–6 weeks’ duration aimed at improving work ability. However, one of the rehabilitation units underwent changes in its organization and did not collect SQRP questionnaires at the end of the rehabilitation programme. This unit with 81 patients (37 men, 44 women) was omitted from the analysis. Thus, 2,784 patients (709 men, 2,075 women) were included in this study.
Outcome variables and analyses
Software (MPI Software, version 3.0) developed by Rudy (22) was used to classify patients’ MPI responses into the profiles. This software determines, based on complex mathematical rules, whether an individual’s set of MPI scale scores are similar to any of the MPI profiles (17). In the SQRP, a Swedish translation of the original MPI was used, since this registry was initiated prior to publication of Bergström et al.’s work (21, 23). However, part III was omitted from the analysis described here (cf. 23).
The Swedish social insurance covers every permanent resident who lives or works in Sweden. It provides financial protection for persons with a disability arising from work injury, illness and old age, as well as for families and children. The prerequisites for the granting of sick leave benefits are: (i) having a disease or injury; and (ii) that this causes a reduction in work ability. If so, financial protection can be drawn as one-quarter, half, three-quarters or full sick leave benefits, depending on the extent to which the person is unable to work. The data concerning all financial benefits are collected in the Swedish Social Insurance Agency Central Registry. Thus, we had the opportunity to use independent individual register data on sick leave benefits for all study participants precisely before the start of and one year after completing a pain rehabilitation programme by aligning the 2 sets of data via the civil registration numbers (21). According to Swedish social security regulations, participation in a rehabilitation programme has the aim of improving or maintaining existing working ability. Therefore we constructed a dichotomous variable: those who had 100% sick leave benefits classified as being on full-time sick leave (FSL), with an odds ratio set at 1, and those with no or part-time sick leave (NSL) benefit, with an odds ratio set at 0. This division was considered reasonable, since it represents the dividing line between not working at all and working part- or full-time.
Statistical analysis
Data analysis was conducted using the Statistical Package for Social Sciences (SPSS, version 18.0) for Windows.
Logistic regression analysis was used to analyse whether changes in MPI profiles might predict which of the persons disabled by pain would be on sick leave benefits 1 year after completing a pain rehabilitation programme. This statistical model was used to predict the probability that having NSL will occur as a linear function of changes in MPI profiles. The results of the logistic regression analyses were presented as odds ratios, i.e. the ratio between odds that an event will occur compared with the odds that the event will not occur. A 95% confidence interval was set as the critical level at or below which the results would be considered statistically significant.
This study was approved by the Regional Ethics Review Board in Umeå (Dnr 2010-168-31 M).
Results
Non-respondents
Out of the 2,784 patients registered in the SQRP MPI data from 2,296 persons (557 men, 1,739 women) could be collected both before and after a completed cognitive behavioural multidisciplinary rehabilitation programme. Thus, the response rate was 2,296/2,784 = 82%. Table I shows that more women than men participated in the rehabilitation programme, and more women than men were respondents. There were also significantly more women than men with university education among the respondents. There was no significant difference between men and women or the respondents and non-respondents with regard to their sick leave situation, while more women among the non-respondents were outside the labour market.
|
Table I. Comparison between respondents and non-respondents at the start of a rehabilitation programme. χ2 test (Mann-Whitney U for age) n = 2,784 |
|||||||||
|
Respondents, n = 2,296 |
Non-respondents, n = 488 |
||||||||
|
Men |
Women |
pa |
|
Men |
Women |
pb |
pc |
pd |
|
|
Gender (%) |
24.3 |
75.7 |
< 0.001 |
31.3 |
68.9 |
< 0.001 |
< 0.001 |
< 0.001 |
|
|
Age, year, mean (SD) |
39.6 (9.2) |
38.7 (9.3) |
0.077 |
38.3 (9.3) |
37.7 (9.0) |
0.543 |
0.129 |
0.064 |
|
|
Education (%) |
|||||||||
|
Primary school |
20.4 |
18.1 |
18.9 |
13.7 |
|||||
|
Secondary upper school |
67.1 |
62.8 |
66.2 |
65.1 |
|||||
|
University |
12.5 |
19.1 |
0.002 |
14.9 |
21.2 |
0.141 |
0.716 |
0.145 |
|
|
Labour market status (%) |
|||||||||
|
Employed/employee |
67.6 |
68.3 |
70.7 |
65.0 |
|||||
|
Unemployed |
28.2 |
25.6 |
27.2 |
25.6 |
|||||
|
Student |
1.9 |
3.4 |
1.4 |
5.0 |
|||||
|
Outside labour market |
2.3 |
2.7 |
0.224 |
0.7 |
4.4 |
0.037 |
0.596 |
0.162 |
|
|
Sick leave situation (%) |
|||||||||
|
No sick leave |
25.5 |
22.5 |
28.9 |
27.4 |
|||||
|
Part-time sick leave |
17.6 |
20.5 |
20.4 |
17.0 |
|||||
|
Full-time sick leave |
56.9 |
57. 0 |
0.188 |
50.7 |
55.6 |
0.533 |
0.387 |
0.098 |
|
|
Coping profiles (%) |
|||||||||
|
DYS |
43.6 |
39.4 |
41.7 |
38.6 |
|||||
|
ID |
25.0 |
33.0 |
24.5 |
31.3 |
|||||
|
AC |
14.9 |
13.9 |
18.7 |
14.7 |
|||||
|
Unanalyzable |
9.3 |
4.4 |
9.4 |
9.1 |
|||||
|
Hybrid |
6.6 |
7.6 |
5.0 |
6.5 |
|||||
|
Anomalous |
0.50 |
1.7 |
< 0.001 |
0.7 |
1.6 |
0.542 |
0.895 |
0.030 |
|
|
ap-value between men and women, respondents; bp-value between men and women, non-respondents; cp-value between respondents and non-respondents, men; dp-value between respondents and non-respondents, women. DYS: Dysfunctional Profiles; ID: Interpersonally Distressed; AC: Adaptive Coper. |
|||||||||
Compared with men, more women had an ID profile. Among the non-respondents there were no significant differences compared with respondents regarding the MPI profiles among men. However, fewer women had an ID profile and there were more Unanalyzable subjects among non-respondents compared with respondents.
MPI profiles
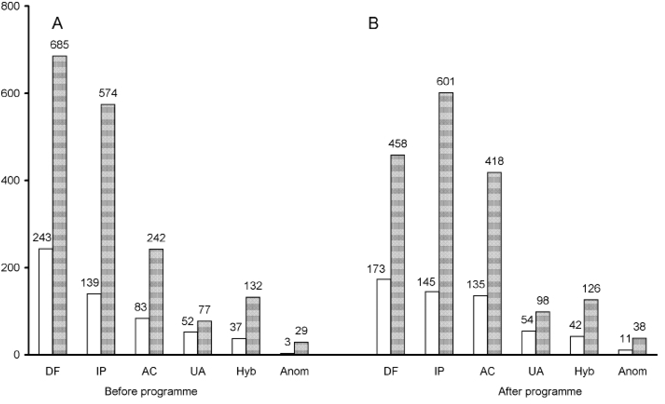
After a pain rehabilitation programme (Fig. 1), there was a significantly decreased share of DYS profiles among both men (243 patients before compared with 173 after (44% and 31%, respectively)) and women (685 and 458 (39% and 26%)) as well as an increased share of AC profiles (men 83 (15%) to 134 (24%) and women 242 (14%) to 418 (24%)). There were no changes in the shares of other MPI profiles (Fig. 1). Significantly more women than men showed an ID profile both before and after the rehabilitation programmes. An opposite distribution was noted among those with Unanalyzable profiles.
In the further analyses we used only the patients with “prototypic” MPI profiles: DYS, ID and AC. The main reason for this was that there were too few observations in the other 3 profiles to enable meaningful statistical analysis. We carried out a separate analysis of hybrids, and found that 90% of patients with a hybrid profile before rehabilitation moved to all 3 prototypic profiles after rehabilitation (among men/women 35/25% moved to DYS, 38/30% to ID and 16/32% to AC, respectively).
Fig. 1. Multidimensional Pain Inventory (MPI) profiles among men (white bars) and women (grey bars) (A) before and (B) after a multidisciplinary pain rehabilitation programme, given as total number of patients. Men n = 557, women n = 1,739; actual numbers inside the boxes. DYS: Dysfunctional; ID: Interpersonally Distressed; AC: Adaptive Coper; UA: Unanalyzable; Hyb: Hybrid; Anom: Anomalous.
Sick leave
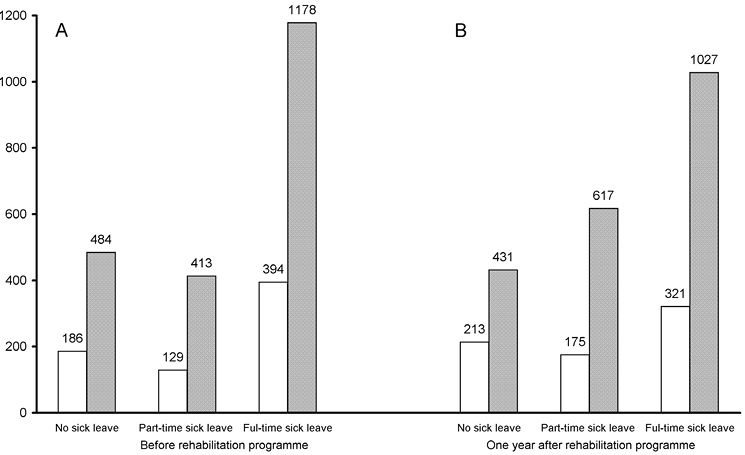
Fig. 2 shows that one year after a completed programme (B), the number of persons on full-time sick leave (FSL) had decreased significantly, both among men, from 394 (56%) to 321 (45%) and women, from 1178 to 1027 (56% to 49%, respectively). At the same time the number of women on part-time sick leave (PSL) had increased from 413 (20%) to 617 (30%), but the number who had no sick leave (NSL) also decreased somewhat, from 484 (23%) to 431 (20%, p < 0.029). Among men, the level with NSL remained unchanged after the programme (30% vs 26% before, n.s.), while the level of those with PSL increased from 129 (16%) to 175 (27%; p < 0.001).
Fig. 2. Number of patients with indicated levels of sick leave (A) just before and (B) 1 year after a multidisciplinary pain rehabilitation programme. Men: white bars, women: grey bars. Total number of patients, men n = 709, women n = 2,075, actual numbers inside the boxes.
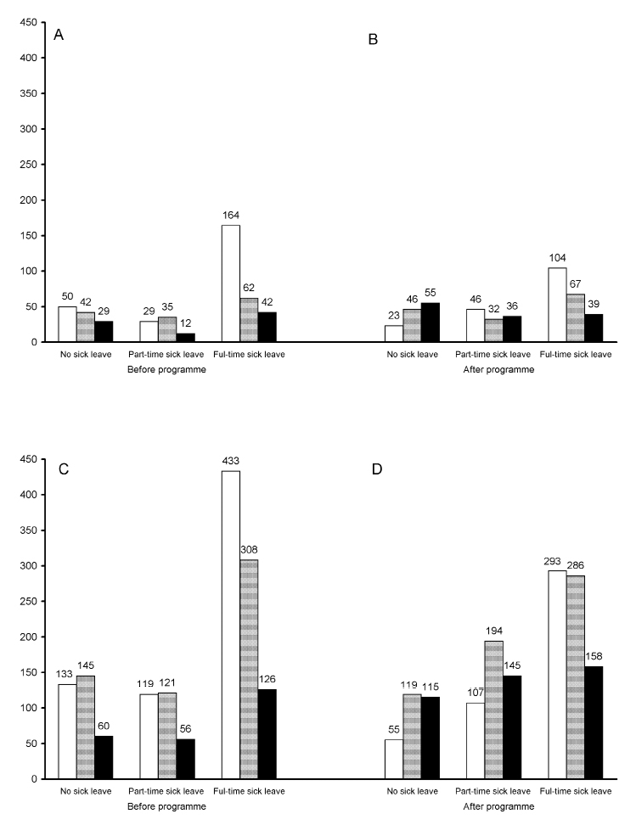
The analysis illustrated in Fig. 3 was carried out to show the distribution of MPI profiles in different sick leave groups before vs after rehabilitation. In general, the DYS profile was underrepresented after the programme among those with NSL 1 year later, while it was correspondingly overrepresented among those with FSL, compared with those with AC profiles in particular. However, the association between the level of sick leave and ID profile was relatively stable, at least among men. In women this profile was overrepresented among those who had either part-time or full-time sick leave.
Fig. 3. Multidimensional Pain Inventory (MPI) profiles (A, C) just before and (B, D) after completing a multidisciplinary pain programme among men (A and B) and women (C and D), respectively, in relation to levels of sick leave one year later. Bars represent MPI profiles: Dysfunctional: white bars, Interpersonally Distressed: light grey bars, Adaptive Coper: dark grey bars. Total number of patients n = 2,296, actual numbers inside the boxes.
Changes in MPI profiles
As shown in Table II, those who had a DYS profile before the programme to a large extent moved into other profiles during the programme. This is particularly the case for women, who moved mainly to the AC profile. The number of AC profiles among men was fairly stable, whereas it decreased among women. The number of ID profiles was relatively stable, although 15% of them moved to AC after rehabilitation.
|
Table II. Changes in the Multidimensional Pain Inventory (MPI) profiles after a pain rehabilitation programme among men and women. Number of patients. p-value, calculated by χ2 test, was < 0.001 for all changes |
|||||
|
Patients with MPI profile |
|||||
|
Determined before programme n |
Determined after programme |
||||
|
DYS |
ID |
AC |
|||
|
Men |
|||||
|
DYS |
212 |
127 |
37 |
48 |
|
|
ID |
113 |
14 |
76 |
23 |
|
|
AC |
68 |
11 |
7 |
50 |
|
|
Total |
393 |
152 |
120 |
121 |
|
|
Women |
|||||
|
DYS |
598 |
319 |
115 |
164 |
|
|
ID |
502 |
57 |
375 |
70 |
|
|
AC |
215 |
35 |
45 |
135 |
|
|
Total |
1,315 |
411 |
535 |
369 |
|
|
Total |
|||||
|
DYS |
810 |
446 |
152 |
212 |
|
|
ID |
615 |
71 |
451 |
93 |
|
|
AC |
283 |
46 |
52 |
185 |
|
|
Total |
1,708 |
563 |
655 |
490 |
|
|
DYS: Dysfunctional profiles; ID: Interpersonally Distressed; AC: Adaptive Coper. |
|||||
The results of multivariate logistic regression with sick leave one year after rehabilitation as the dependent variable are shown in Table III. There were gender differences regarding MPI profile changes after attending a rehabilitation programme with respect to the possibility of an improved sick leave situation, i.e. having no or part-time sick leave.
|
Table III. Results of logistic regression analysis presented as odds ratio (OR) and 95% confidence interval (95% CI) for having Not Full-time Sick Leave (NSL) after a work ability improving pain rehabilitation programme among men and women. Those who were Adaptive Copers (AC) before and remained AC after the programme were used as a reference with OR set at 1 |
|||||
|
Men (n = 398) |
Women (n = 1,320) |
||||
|
n (%) |
OR (95% CI) |
n (%) |
OR (95% CI) |
||
|
AC-AC |
51 (13) |
1.00 |
135 (10) |
1.00 |
|
|
AC-DYS |
12 (3) |
1.04 (0.24–4.48) |
35 (3) |
0.33 (0.16–0.72) |
|
|
AC-ID |
7 (2) |
0.97 (0.17–5.61) |
46 (3) |
0.82 (0.41–1.66) |
|
|
DYS-DYS |
128 (32) |
0.24 (0.12–0.48) |
316 (24) |
0.27 (0.18–0.41) |
|
|
DYS-ID |
37 (9) |
0.17 (0.06–0.42) |
116 (9) |
0.49 (0.30–0.82) |
|
|
DYS-AC |
47 (12) |
0.69 (0.29–1.62) |
170 (13) |
0.66 (0.41–1.05) |
|
|
ID-ID |
78 (20) |
0.60 (0.28–1.29) |
374 (28) |
0.53 (0.35–0.80) |
|
|
ID-DYS |
14 (4) |
0.39 (0.12–1.31) |
57 (4) |
0.29 (0.15–0.56) |
|
|
ID-AC |
24 (6) |
1.40 (0.44–4.50) |
71 (5) |
0.90 (0.49–1.65) |
|
|
DYS: Dysfunctional; ID: Interpersonally Distressed profile. |
|||||
Among men, those who remained with a DYS profile or moved from a DYS profile to an ID profile were associated with a significantly (4–5 times) lower probability; (OR 0.24–0.17) of having NSL. Among women, each combination in which moving into a DYS profile was involved after a completed pain rehabilitation programme, was associated with a considerably lower probability (2–5 times) of having NSL one year later. In contrast, those with a DYS profile or those with an ID profile that changed to an AC profile after the programme had an odds ratio of up to 1.6 of having NSL. Also, those with an ID profile who remained in the same profile had a lower probability of having NSL, although this association was of lower magnitude than for those with a DYS profile.
Discussion
This study confirms previous observations (19, 24) that persons with DYS profiles have higher levels of sick-leave compared with those with AC or ID profiles. The DYS profile is characterized by high pain severity, high interference, high affective distress, low life control and low activity level. Moreover, those persons appear to have sub-optimal coping strategies compared with persons with the AC profile (17).
The main results of our study are that moving into an AC profile nearly normalized the risk of having NSL one year after a rehabilitation programme, and that persons staying with or moving into a DYS profile at that point in time had a low probability of improving his/her sick leave situation.
Furthermore, although this study is not an effect study and we rely on observational data, though at a considerable volume, it appears that the current cognitive behavioural pain rehabilitation programmes in Sweden decreased the level of full-time sick leave one year later. This decrease resulted in an increase in part-time sick leave rather than an increase in having no sick leave; however, part-time sick leave is considered an appropriate transition from a period of sickness to work (cf. 25).
Our results suggest that rehabilitation programmes performed at the units participating in the SQRP have an insufficient effect on one-quarter of the persons with a DYS profile. Junghaenel et al. (26) have found that patients with a DYS profile engage in more catastrophizing and overt pain behaviour. These authors suggest that such patients may benefit from interventions that guide them toward decreasing pain catastrophizing, not only using cognitive restructuring, but also by learning more adaptive means of communicating their pain experience and desire for support. There should thus be more emphasis on such psychological components of the programmes used. A related problem is that there is a lack of adequately trained psychologists with a cognitive-behavioural background in Sweden, thus some programmes use psychotherapists after short training.
An ID profile was also associated with a varying chance of improving the sick leave situation, in particular among women. The ID profile is characterized by low levels of perceived support from significant others. Bergström et al. (23) have found a substantially weaker negative correlation between perceived support from significant others and punishing responses for men compared with women. It has also been indicate (26) that the difference between patients with ID and DYS profiles is vague and there are no differences between these 2 profiles on a global measure of psychological distress.
Regarding the persons with an AC profile before rehabilitation, approximately 15% changed to either DYS or ID profiles after the programme, a less favourable outcome, since these profiles were usually associated with a higher risk of sick leave. Taken together with the gender differences observed, these results indicate that more care should be taken in individualizing the rehabilitation programmes offered.
Gender issues
McCracken (27) suggested that both solicitous and punishing responses from significant others were negatively associated with acceptance of pain, i.e. that social influences can play a role in patients’ engagement in activity with pain present and their willingness to have pain without trying to avoid or control it. Moreover, the empirical evidence demonstrates a strong and consistent relationship between marital satisfaction and psychological distress in pain samples (28). Spouse responses are associated with pain outcomes and marital satisfaction appears to have an indirect link with pain severity through the effect of these spouse responses. Thus, the rehabilitation of ID patients should perhaps have more focus on improving the coping of both patients and family.
Some women who had no sick leave before the programme developed part-time sick leave afterwards. Boonstra et al. (29), in a study of pre-treatment expectations of rehabilitation outcomes, found that women were more likely than men to expect that the treatment would better enable them to accept that they could no longer do what they were able to previously. Thus, if the patients own expectations were fulfilled during the programme it might result in women gaining a better insight and acceptance of their decreased capacity, which in turn might even lead to insight that sick leave is necessary, albeit part-time and for a short time period, in order to maintain full-time working ability in the longer term. Women also expected that they would have fewer problems with household activities after treatment (29). On the other hand, men were more likely than women to expect that the treatment would enable them to cope better with being a spouse. This issue is often associated with the distribution of domestic work between spouses. In this case, it can be supposed that women choose to take more responsibility for domestic work by means of part-time sick leave. However, this strategy can, of course, be disadvantageous for women long term.
We did not find any previous study that has documented the distribution of the MPI profiles among both genders. Some studies report gender as a variable when they describe the population included in the study, but they do not report the results about MPI profiles separately for each gender (19). Our study did not find any statistically significant differences in the distribution of profiles between men and women, with the exception of the ID, where women dominated. However, this may not be a real gender difference. The proportion of men who had an Unanalyzable profile was significantly larger than among women. An explanation for this could be that there were significantly more men (9%) than women (5%) without a spouse or significant others, which is the main characteristic of this profile.
Study limitations
This study was carried out on a Swedish population with chronic musculoskeletal pain, which might make generalizing the results difficult. However, Rudy (22) has used several studies from Sweden (30, 31) as part of the normative data in the MPI Software, version 3.0. Thus, we considered that the results presented in this study would be comparable with results from other MPI studies. Furthermore, the Swedish Quality Registry for Pain Rehabilitation includes approximately 80% of pain management care programmes in Sweden, from the public as well as the private sector, making it possible both to obtain large data samples and to follow changes over time. Further strengths of this study were that the response rate was proportionately high (82%) and included a large number of men.
One explanation for the proportionally high response rate might be that the initial and post-programme questionnaires were collected during the time when the participants were in a position of dependence on the programme staff, although it was stressed (according to ethical research norms), that completing the questionnaire was voluntary and would not influence the therapy. Nevertheless, it cannot be entirely excluded that there was a bias towards indicating desired results by the patients when completing the questionnaires. However, it would be difficult to systematically “trick” a complex questionnaire like that of the MPI.
The results of the multivariate logistic regression presented in Table III should be considered with caution, since the wide confidence intervals in the analyses indicates a low statistical power, especially with regard to gender differences.
Another difficulty might be whether the MPI profiles are inherently stable over time. This has been examined by Broderick et al. (32), who found that up to one-third of fibromyalgia patients not undergoing intervention changed their MPI profiles within a 2–4-week period. It is debatable whether these results are representative of chronic pain patients seeking treatment, since the patients in Broderick’s study (32) were recruited through advertising, which had a low response rate. Furthermore, a systematic relationship like the one found in the present study is extremely unlikely to be caused by random instability.
The aim of the present study was not to estimate the effect of the rehabilitation programmes performed at the units included in the SQRP or to analyse the factors and mechanisms that lead to change in the MPI profiles. Although all units state that their programmes are based on the behaviourally oriented programme developed by Fordyce (33) with cognitive aspects (34) and elements of acceptance psychotherapy (35), it was not possible to obtain detailed and meaningful data about the exact content and volume of these programmes from the various units participating in the SQRP.
Conclusion
The cognitive behavioural pain rehabilitation programmes currently used in Sweden changed the MPI profiles of participants in this study in a systematic fashion. A change to an AC profile following the rehabilitation programme improved the sick leave situation one year later, whereas a change to a DYS profile after the programme, compared with those with AC and ID profiles, was associated with a 4–5 times lower chance of improving the sick leave situation 1 year after a rehabilitation programme, i.e. long-term; in particular among women. Our findings suggest the need to tailor rehabilitative strategies differently for men and women.
ACKNOWLEDGEMENTS
Supported by the Swedish National Board of Health and Social Welfare (grant no: 51-6065/2004).
The authors would like to thank Arlene Johnston for her excellent review of the English manuscript.
References

