Michele Maiers, DC, MPH, Corrie Vihstadt, MOm, LAc, Linda Hanson, DC and Roni Evans, DC, MS, PhD
From the Wolfe-Harris Center for Clinical Studies, Northwestern Health Sciences University, Bloomington Minnesota, USA
OBJECTIVE: To explore perceptions of spinal manipulative therapy and exercise among adults aged 65 years and older with chronic neck pain.
DESIGN: Mixed methods study embedded within a randomized clinical trial.
Subjects/Patients: Interviews were conducted with 222 of 241 randomized clinical trial participants. They had a mean age of 72.2 years and they had neck pain of moderate severity and of 6 years mean duration.
METHODS: Semi-structured interviews were conducted at the completion of the 12 week intervention phase, during which participants received spinal manipulative therapy and exercise interventions. Interviews explored determinants of satisfaction with care, whether or not therapy was worthwhile, and what was liked and disliked about treatment. Interviews were recorded and transcribed; content analysis was used to identify themes within responses.
RESULTS: Participants placed high value on their relationships with health care team members, supervision, individualized care, and the exercises and information provided as treatment. Change in symptoms did not figure as prominently as social and process-related themes. Percpetions of age, activities, and co-morbities influenced some seniors’ expectations of treatment results, and comorbidities impacted perceptions of their ability to participate in active care.
CONCLUSION: Relationship dynamics should be leveraged in clinical encounters to enhance patient satisfaction and perceived value of care.
Key words: elderly; neck pain; qualitative; satisfaction.
J Rehabil Med 2014; 46; 00–00
Correspondence address: Michele Maiers, Northwestern Health Sciences University, 2501 W 84th St, Bloomington, MN 55337, USA. E-mail: mmaiers@nwhealth.edu
Accepted May 26, 2014; Epub ahead of print Sep 22, 2014
Introduction
Patients’ perceptions and the individual experience of care are important factors in determining the value of an intervention in health care (1, 2). Patient-centeredness “responsive to individual patient preferences, needs, and values” is one of 6 dimensions of quality and value in healthcare identified in a seminal report by the Institute of Medicine (3). This concept has been expanded by the Institute for Healthcare Improvement, which specifically identifies patient satisfaction as a system metric for quality improvement (4). Patient satisfaction and an individual’s opinion of what makes an intervention worthwhile may uniquely influence health care expenditures (5) and possibly models of care delivery in the future.
Understanding perceptions of care among individuals with spine-related pain and disability is of increasing importance. The impact of these conditions, including soaring costs, (6, 7, 8) has become a topic of global interest (9). Of particular concern is the prevalence of neck pain (NP) among senior citizens, 20% of whom report NP monthly (10). Often associated with other health complaints and poor self-rated health (11), NP additionally presents a threat to independence and functional capacity in a rapidly growing demographic (12, 13). The magnitude of these concerns underscores the need to consider what determines value among seniors receiving treatment for NP. Identifying the facets of a clinical encounter that contribute to a positive therapeutic experience may enhance compliance and clinical outcomes (14).
This study used mixed methods to explore perceived value of 3 treatment approaches among seniors with chronic NP: spinal manipulative therapy with home exercise, supervised rehabilitative exercise plus home exercise, and home exercise alone. Domains drawn upon to elucidate value include satisfaction with care, whether or not therapy was worthwhile, and what was liked and disliked about treatment.
Methods
The parent randomized clinical trial (RCT) (Clinical trials registry number: NCT00269308) included individuals 65 years of age and older with chronic NP who were community dwelling and independently ambulatory. Participants were randomized to receive 12 weeks of i) spinal manipulative therapy (delivered by chiropractors) with home exercise, ii) supervised rehabilitative exercise (delivered by exercise therapists) plus home exercise, or iii) home exercise alone (delivered by either a chiropractor or exercise therapist). Demographics and clinical characteristics were recorded at baseline. Patient self-report outcomes were measured at baseline and 4, 12, 26, and 52 weeks post-randomization. Biomechanical outcomes were measured at baseline and week 12. Individual qualitative interviews were conducted at the conclusion of the intervention phase (week 12). A detailed description of the study design, data collection, and treatment interventions has been reported (15), as has the results of the trial (16). This study was granted approval from the institutional review boards of all participating institutions and all individuals provided written informed consent before enrollment.
Interventions
Home exercise (HE) was individually instructed during 4, 45–60 min sessions with an exercise therapist or a chiropractor. Participants received reassurance that movement and exercise are good for their neck, even if they experience discomfort or have an arthritic condition. To reinforce the message to stay active, participants were given instructions for simple daily exercises designed to improve neck and back range of motion, trunk strength and endurance, and overall balance and coordination (15). Participants were issued written and illustrated descriptions of each exercise, and a diary to record their exercise progress. Exercises were tailored to the individual patient’s level of ability and were reviewed for form and degree of challenge during sessions 2 through 4.
In addition, participants were given information about how to manage their NP, including self-care for pain management (e.g., the use of ice and heat), postural instructions, and practical demonstrations of proper body mechanics for activities of daily living, all performed with patient participation.
Spinal manipulative therapy with home exercise (SMT+HE) combined manual treatment, delivered by chiropractors, with the home exercise program (above). Manual treatment included spinal manipulation, mobilization and flexion-distraction therapy, with light soft tissue massage as indicated to facilitate the manual therapy (17). The technique and force applied was modified to accommodate the age and physical condition of the study participant. The number and frequency of treatments was determined by the treating chiropractor, with a maximum of 20 visits.
Supervised rehabilitative exercise plus home exercise (SRE+HE) expanded upon the home exercise program (above) with 20 additional, 1-h sessions supervised by an exercise therapist. Each session began with a light aerobic warm up, consisting of 10–15 min on a stationary bicycle, treadmill, or elliptical trainer. The remainder of the hour was spent performing exercises similar in nature to those in the HE program, focused on stretching, strength, endurance, and balance. Participants performed high repetitions of assigned low load exercises, under the individualized guidance of exercise therapists who closely monitored form, modified exercises, prescribed progressions, and provided encouragement over the course of 12 weeks.
Qualitative interviews
Supplementary qualitative methods were employed as an extension to the core quantitative study, as a means to illustrate and provide depth of meaning when interpreting quantitative study results (18). A pragmatic mixed methods approach (19) was used. Narrative data were considered in the context of a post-positivist interpretive framework, as multiple study participants informed a range of perspectives and no singular reality. Interviews asked participants to reflect on the care they received in the study. Participants were assured confidentiality, encouraging them to speak freely and without risk to their relationship with the study or university (20). Permission was obtained from each participant to audio-record the interview session.
A semi-structured interview schedule of open-ended questions and standardized probes was administered to all consenting participants (Table I). Eight members of the study team conducted the interviews in private clinic rooms and adhered to best practices in guiding interviews and probing techniques (21). The first question asked participants to reflect on their response to a question they answered in the week 12 self-report questionnaire: “Overall, how satisfied are you with the care you have received for your neck pain in the study so far?” (15) Subsequent questions asked participants if they felt their treatment was worthwhile, and why, as well as what they did and did not like about the care they received in the study. Interview questions used standardized study language familiar to patients when referring to the interventions. For example, spinal manipulative therapy was called “chiropractic care”. Supervised rehabilitative exercise was qualified with “the exercises you did here (at our clinic)” when clarification was needed to distinguish it from the home program.
|
Table I. Interview schedule |
|
|
Question number |
Question |
|
1. |
When we asked, “Overall, how satisfied are you with the care you received in the study?” what things did you take into account when deciding how satisfied you were? |
|
2.a |
When we asked you overall how much your back/neck pain has changed, what things did you consider when answering that question? |
|
3. |
What did you like the best about the a) home exercise program you had in the study? When applicable, b) exercise therapy/chiropractic treatments you had in the study? |
|
4. |
What did you like the least about the a) home exercise program you had in the study? When applicable, b) exercise therapy/chiropractic treatments you had in the study? |
|
5. |
Overall, did you feel like the care you had in the study was worthwhile? (If “yes”) Why was it worthwhile? (If “no”) Why wasn’t it worthwhile? |
|
aQ2 is analyzed separately and will be reported elsewhere. |
|
Data were kept in a secured area, including a locked filing cabinet for paper-based data and a password protected web-based database system for electronic audio and transcribed Microsoft Word files. Research staff transcribed the interviews. A quality assurance check was performed on all interviews to compare transcripts to the original recorded interviews, ensuring accuracy of the transcription. Interviews were imported into NVivo® v 9.2 (QSR International Pty Ltd, Victoria, Australia) for analysis.
Analysis
Descriptive statistics were used to describe participants’ demographic and baseline clinical characteristics.
Content analysis drew on both deductive and inductive approaches (22) to identify themes representing participants’ responses to each question (23). A codebook, which was initially informed by data from qualitative interviews conducted by the authors (MM and RE) in similar populations (24– 27), was added to or modified by MM and CV while conducting this analysis. Prior to reading interview transcripts, MM and CV identified their assumptions and biases: themes elicited from an elderly neck pain population will mirror those from a general neck pain population, be influenced by age and co-morbidities, include psychosocial wellbeing which may be uniquely important to this group, reflect stoicism about pain, and skew in a positive direction with regard to whether treatment was “worthwhile.”
Interviews were read and coded independently. They were discussed after two blocks of 5 and then after subsequent blocks of 10 to reach consensus on coding of themes. A dynamic approach to the codebook was taken, iteratively expanding and revising the themes and definitions as new ideas were introduced in the interviews (23). Responses that were suggested or “led” by the interviewer were not coded. Any themes that arose in response to a previous question and were added by the participant out of order were coded to the question that the comment pertained to. Quality assurance checks were conducted by RE and LH on a random 10% of interviews; all identified discrepancies were revisited and resolved by MM and CV. The frequency of interviews containing each theme was quantified and representative patient quotations were identified (28, 23). Themes were organized thematically in NVivo to explore and illustrate relationships among themes (29).
Results
Of the 241 participants in the RCT, qualitative interviews were collected on 222 individuals. Reasons for not participating include not attending the week 12 follow-up appointment (n = 13), time constraints (n = 3), declined to be interviewed (n = 2), and death (n = 1). Participants’ mean age (standard deviation (SD)) was 72.2 years (5.4); 47% were female. Median duration of NP was 6 (14.4) years, with a mean pain rating of 5 (SD 1.4) on a scale of 0–10. Demographic and baseline clinical characteristics of this cohort were not different from the total sample in the parent trial (16).
Determinants of satisfaction
The most common determinant of satisfaction was interaction:
“Everyone was always courteous, kind, friendly…willing to answer any questions. I never felt that I was being hurried out… Sometimes you think, ‘oh goodness gracious I’ve got to hurry because they want to get rid of me.’” SMT + HE 11909
Exercise recommendations, supervision and individualization, information, perceived treatment effect, and change in neck pain were also common determinants of satisfaction (Table II). Interaction figured least prominently in the HE group. In contrast, supervision and individualization was mentioned nearly twice as often by those in the SRE+HE group:
“They go over exactly what you’re doing so when you get home, you did it exactly the way you were told.” SRE + HE11468
Despite standardizing the amount and type of advice delivered during the home exercise sessions received by participants in all three groups, information was identified as a determinant of satisfaction most often among in the HE group.
Other determinants of satisfaction noted less frequently include the mechanics of appointment management, whether treatment met their expectations, additional changes in health or well-being, and various aspects of the care delivered.
|
Table II. Most common determinants of satisfaction |
|||||
|
Theme |
Definition |
Group |
|||
|
SMT + HE n = 75 |
SRE + HE n = 75 |
HE n = 72 |
Total n = 222 |
||
|
Interaction |
Personal exchange with staff or providers, attributes of personnel (e.g., attitude, personality, demeanor) |
50 |
58 |
33 |
141 |
|
Exercise recommendations |
Including exercises in general, specific exercises mentioned, and components of exercise program (e.g., information regarding exercise) |
20 |
28 |
22 |
70 |
|
Supervision and individualization |
Oversight by provider; care tailored to meet the needs of the individual (e.g., modifications, accommodations) |
13 |
25 |
10 |
48 |
|
Information |
Information exchanged (e.g., cause, prevention, prognosis) |
8 |
11 |
24 |
43 |
|
Perceived treatment effect |
Perceived treatment effect relating to “change” or “progress”, not otherwise specified |
17 |
13 |
9 |
39 |
|
Change in neck pain |
Includes severity, frequency, quality (e.g., pain, achiness, throbbing, burning, stiffness) specific to the neck area |
12 |
4 |
16 |
32 |
|
SMT + HE: spinal manipulative therapy with home exercise; SRE + HE: supervised rehabilitative exercise plus home exercise; HE: home exercise. |
|||||
Worthwhile care
At 94% (n = 208), the majority of participants considered study treatment worthwhile:
“I’m planning on living to be a hundred years old. I’ve got to take care of this old bod!” SMT + HE 12824
Only 4% (n = 9) said it was somewhat worthwhile, and 2% (n = 5, all in the HE group) said it was not. Among those who felt it was not worthwhile, explanations included unmet expectations of treatment, a lack of discipline to comply with exercise treatment, an increase in neck pain, and lack of perceived treatment effect.
“I got a small amount of results and put in an awful lot of effort.” HE 11870
There was general consistency between groups in the frequency of individual themes, which are collectively displayed in Fig. 1. Self-efficacy figured prominently, cited by 43 participants (24 of whom were in the SRE + HE group):
“I was doing something for myself…being 74 years old, I guess you don’t think that you can get any better, you’re just old. I found out that I can do something…I was able to improve myself.” SRE+HE 10489

Perceived treatment effect was also common (n = 34), in addition to change in NP (n = 31), and strength and motion (n = 28).
Expectations (n = 30) were also commonly referred to when determining what made treatment worthwhile. Twenty-three of these comments were focused on future expectations, including a desire to maintain exercise habits after the study to prevent future deterioration and an expectation to continue improving after the study’s conclusion. Eight compared pre- and post-treatment expectations in terms of the therapeutic encounter itself and anticipated changes in perceived treatment effect:
“I don’t necessarily have to baby my neck…I had been told by a doctor, ‘Well, eventually as you get older it will just go stiff’…I found that was a bunch of malarkey.” SRE + HE 12040
Other changes in health or wellbeing, the experience of participating in a research study, and various aspects of the care delivered were themes additionally indicated by a minority of participants.
Most liked feature of treatment
While participants offered a wide variety of responses to what they liked best, the vast majority identified a core set of themes. While there was wide agreement among individuals within treatment groups of what was liked best, there were notable differences between themes identified for each modality used (Table III). Interaction was noted as a favorable aspect of chiropractic care by 56% (n = 42) in the SMT + HE group, and as a favorable aspect of supervised exercise by 41% (n = 31) in the SRE + HE group, but as a favorable aspect of home exercise by only five individuals (one of whom was in the HE group).
“[Provider] was very encouraging…she could be my granddaughter. I appreciated that she was nice to an old lady.” SRE + HE 10756
|
Table III. Most liked feature of treatment |
||
|
Treatment received |
||
|
Chiropractic care (n = 75) |
Supervised rehabilitative exercise (n = 75) |
Home exercise (n = 222) |
|
Interaction (n = 42) Perceived treatment effect (n = 25) Ancillary therapies (n = 24) |
Supervision/individualization (n = 36) Interaction (n = 31) General exercise recommendations (n = 19) |
General exercise recommendations (n = 62) Convenience (n = 55) Specific exercises (n = 42) Strength/motion (n = 32) |
Twenty-four in the SMT+HE group cited ancillary treatments such as massage (n = 21) and a moist hot pack (n = 5) as the most liked feature of treatment. Those in the SRE+HE group noted exercise recommendations (n = 19), specifically the variety of exercises (n = 6) and being offered progressively difficult maneuvers (n = 5) in the supervised exercise component of their care as the most liked feature of treatment.
The home exercise program was a part of treatment for participants in all three groups (n = 222). Twenty-eight percent (n = 62) identified specific components of the program as being the thing they liked best about receiving the HE intervention, including the exercises themselves, information regarding exercise, and instructional materials:
“The little diagrams, the pictures to help me remember, and then the checklist that I could go to each day to make sure that I had [them] done.” SMT + HE 10164
The convenience of doing the HE program at one’s own pace and on one’s own schedule was identified by 25% (n = 55) as the most liked feature. Perceived change in strength or motion (n = 32) and the compulsion to have the discipline to create an exercise habit (n = 35) were similarly noted by participants as the most liked feature of the HE program.
Specific exercises were identified by 19% (n = 42) of participants as “best liked,” and included neck strengthening maneuvers done in flexion and extension against resistance using rubber tubing (n = 22), and stretching (n = 12).
Least liked feature of treatment
As was the case with features of treatment best liked, least liked themes varied widely between different modalities used in study treatment (Table IV). Of interest, “nothing” was indicated as being disliked about chiropractic care by 57% (43/75) of those in the SMT + HE group, about supervised exercise by 39% (29/75) of those in the SRE+HE group, and about home exercise by 17% (37/222) by all participants.
|
Table IV. Least liked feature of treatment |
||
|
Treatment received |
||
|
Chiropractic care (n = 75) |
Supervised rehabilitative exercise (n = 75) |
Home exercise (n = 222) |
|
Nothing (n = 43) Dose (n = 10) Manipulation/ mobilization (n = 8) Side effects (n = 7) Transportation/ commute (n = 6) |
Nothing (n = 29) Specific exercises (n = 20) Challenge (n = 17) Side effects (n = 6) |
Specific exercises (n = 84) Habit/ discipline (n = 65) Nothing (n = 37) Challenge (n = 33) Side effects (n = 27) |
With regard to the specific exercises identified by 84 participants as the least liked part of the home exercise program, the one most commonly referenced by participants was also identified as one that was liked best: neck strengthening against resistance, using rubber tubing (n = 30). Balance exercises (n = 16) were also cited as “least-liked” for their perceived difficulty or lack of relevance:
“There were a couple of exercises that, at first I was so frightened of really…I kept thinking I was going to topple over.” SRE + HE 9146
Specific exercises in the supervised exercise component of care were mentioned less frequently in the SRE + HE group (n = 20) as being the “least-liked,” and included squats (n = 5) and neck strengthening maneuvers using rubber tubing (n = 4). Among those who reported dose as something they liked least about chiropractic treatment, some felt there were too many treatments, while others wished for a higher dose in terms of frequency and duration of visit:
“I think ten minutes is a very small time…I spend more time for driving than I spend here.” SMT + HE 11777
Of particular note, side effects were noted as something they liked least about chiropractic treatment by 7/75 (9%) of participants in the SMT+HE group, about supervised exercise by 6/75 (8%) in the SRE + HE group, and about home exercise by 27/222 (12%) by all participants. These side effects commonly included muscle soreness and increases in neck and joint pain.
Influencing factors
Several themes arose across interview questions that influenced the direction or strength of other responses (30), and may be unique to an elderly population. Co-morbidities, mentioned by nearly a quarter of all participants (n = 50), were cited as limiting improvement or creating difficulty performing exercises. Those most frequently mentioned included shoulder, hip and knee pain, cardiovascular disease, and arthritis:
“I’ve been having so much trouble with my knee that it kind of affects everything.” HE 11960
Age was another influencing factor, cited by 22 participants. Age was used to provide context around their condition or progress (e.g., “I am 77 years old…”), as justification (e.g., “for my age”), and as impacting prognosis (e.g., “as I get older”).
Activities of daily living were used to qualify the responses of 13 participants. House and yard work like raking leaves and shoveling snow, computer use, and “helping the wife,” were all cited as hindrances to improvement.
Interestingly, 7 participants used language that implied a degree of stoicism toward pain, typically when framing discussion about difficulty performing exercises or side effects experienced during study treatment:
“Some of the exercises are more strenuous on a specific person than others. I guess I’m not a person that gives in to complaining…” SRE + HE 8332
Discussion
When considering responses to interview questions in aggregate, several consistent themes emerge to inform what factors influence participants’ perception of value. These influencing factors can be categorized into 3 primary domains: how care was delivered, what care was provided, and which results were felt to be of value (see Fig. 2). These can be further distilled into 3 main concepts to increase the perceived value of an intervention. The first concept focuses on interpersonal dynamics. In one regard, this is expressed by the value that patients place on the relationships they develop with members of a health care team. It is additionally demonstrated by how valued they feel as an individual patient, as demonstrated by providers who tailor treatment to meet their unique needs. Providers may wish to capitalize on these and similar findings, emphasizing relational dynamics in clinical encounters to enhance patient satisfaction and patients’ perceived value of care (31, 32). In these ways, relationships can be leveraged to optimize active care and the transfer of information from provider to patient. This may aid in attaining desired treatment effects, which likely include improvement in pain, functional ability, and self-efficacy. Providers should be aware that age and activity may influence seniors’ expectations of treatment results and that co-morbidities can impact both expectations of results and how seniors perceive their ability to participate in active care.
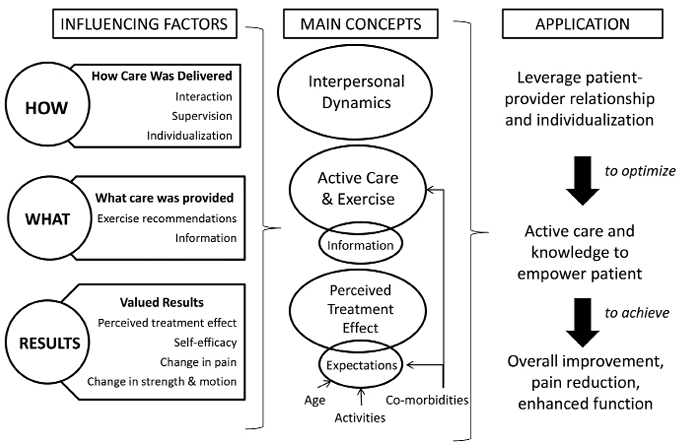
Fig. 2. Influence of perceived value on chiropractic care and exercise interventions.
Among this cohort, change in symptoms did not figure as prominently as social and process-related themes. This is an emerging observation in qualitative musculoskeletal research (33, 34), although not identified specifically among an elderly population to date. It is possible that seniors grow to accept pain and other physical limitations as they age and over the course of chronic conditions like musculoskeletal pain (35). As a result, they may place greater importance on psychological or social benefits of treatment, like interaction and self-efficacy, as was noted in response to liked features and what made treatment worthwhile.
Several influencing factors were noted in the interviews. Concomitant co-morbidities and age were referred to as immutable barriers to improvement; this is consistent with what has been reported previously in the literature (36, 37). Stoicism was also noted in some interviews, as participants emphasized that despite clinical symptoms they continue on with daily activities and don’t allow pain to impact their life. Stoicism is a consistent theme emerging from research of elderly with chronic pain and is often identified as a contributor to the decision not to seek health care (38). In this sample, we noted a sense of determination and independence in spite of limitations secondary to their NP condition.
Results from this study may be transferable (39) to other elderly, community dwelling populations. Sampling in the parent RCT targeted a wide range of communities in and around a metropolitan area (15). Compared to other qualitative research, the relatively large sample size may increase the external validity of our findings. Further, the recurrence of interaction, exercise recommendations, supervision, and self-efficacy as prominent themes suggest a shared perception of experience among this group of seniors, which may be generalizable to a broader audience.
These study findings are limited by a lack of triangulation with members of the interviewed cohort. The intentions of participants were not verified against our interpretation of interviews. Member checks were not conducted due to the gap of time between when the interviews took place (at the end of each participant’s intervention phase, over the course of 3 years) and when analysis was done (after all study data had been collected). Additionally, it is possible that other seniors, with other pain conditions and receiving care in different environments, may have different responses. We also hypothesize that the perception of value was influenced by receiving care at no cost within the context of this study. A fee-for-service encounter may elicit other responses.
Design differences in this study’s treatment groups resulted in varying degrees of provider interaction, which likely contributed to differences observed in participant responses to interview questions. During the 12-week intervention, those in the HE group attended 4 treatment visits; the mean number of visits in the SMT + HE group and SRE + HE group were 15.1 (range 5–19) and 16.6 (range 0–19), respectively. This study was designed as a pragmatic trial; therefore, no attempt was made to control for the amount of time or attention received in treatment. As a result, interaction as a theme may have been overrepresented by those in more time-intensive treatment groups (i.e., the SMT + HE group and SRE + HE group). Supervision and individualization were commonly identified themes among those receiving supervised exercise.
In conclusion, interviews can be powerful tools for adding a depth of understanding to patient perspectives and outcomes, as well as providing insight into the experience of health care. Interaction, supervision, and exercise in general were commonly valued components of conservative care for NP among this group of seniors. Clinical focus on these components of musculoskeletal care may enhance the therapeutic management of an important and growing population.
“I feel that I’m on the road to being a lot stronger and in the long run…better health. I don’t want to ever be considered disabled. You know, as you get older [voice breaks] that could possibly happen.” SRE + HE 8373
Acknowledgments
This research was funded by the U.S. Department of Health and Human Services (HHS), Health Resources and Services Administration (HRSA), Bureau of Health Professions (BHPr), Division of Medicine and Dentistry (DMD) under grant number R18HP01425, Chiropractic and Exercise for Seniors with Neck Pain. The content and conclusions of this manuscript are those of the authors and should not be construed as the official position or policy of, nor should any endorsements be inferred by the U.S. government, HHS, HRSA, BHPr, or the DMD.
References

