Aileen L. Bergström, OT, PhD1,2, Lena von Koch, PT, PhD1,3, Magnus Andersson, MD, PhD3, Kerstin Tham, OT, PhD1 and Gunilla Eriksson, OT, PhD1,2,4
From the 1Department of Neurobiology, Care Sciences and Society, Division of Occupational Therapy, Karolinska Institutet, Huddinge, 2Department of Neuroscience, Rehabilitation Medicine, Uppsala University, Uppsala, 3Department of Neurology, Karolinska University Hospital, Stockholm and 4Department of Neuroscience, Research in Disability and Habilitation, Uppsala University, Uppsala, Sweden
OBJECTIVE: To explore and describe persons with stroke and their caregivers’ restrictions in participation in everyday occupations, i.e. occupational gaps, 3–6 months post-stroke, in relation to life satisfaction, combined life satisfaction, caregiver burden, perceived impact of stroke, and activities of daily living.
DESIGN: Cross-sectional study.
SUBJECTS: Persons with stroke and their caregivers (105 dyads).
METHODS: The Occupational Gaps Questionnaire, Life Satisfaction Checklist, Caregiver Burden Scale, Stroke Impact Scale and Barthel Index were used. Correlations were analysed with Spearman’s rank, and regression analyses used life satisfaction as the dependent variable.
RESULTS: At least one person in 86% of the dyads perceived restrictions in participation, with the most common gap in travelling for pleasure. Correlations were low between the numbers of occupational gaps and life satisfaction (R = –0.33, R = –0.31); however, life satisfaction accounted for occupational gaps both for persons with stroke and for caregivers. A greater number of occupational gaps were perceived in the dyads with combined low levels of life satisfaction compared with those with combined high levels of life satisfaction.
CONCLUSION: Participation in everyday occupations is related to life satisfaction even for caregivers of persons with stroke. The results of this study add to our knowledge about the stroke-caregiver dyad and will help to inform family-centred approaches within stroke rehabilitation.
Key words: stroke; occupational therapy; occupational gaps; dyads.
J Rehabil Med 2015; 47: 00–00
Correspondence address: Aileen Bergström, Department of Neurobiology, Care Sciences and Society, Division of Occupational Therapy, Karolinska Institutet, Alfred Nobels allé 23, SE-141 83, Huddinge, Sweden. E-mail: aileen.bergstrom@ki.se
Accepted Feb 9, 2015; Epub ahead of print Apr 16, 2015
INTRODUCTION
After having a stroke, persons often perceive restrictions in performing different activities in their everyday life (1) and often receive assistance from an informal caregiver (2). We have modified the definition of informal caregiver (shortened to “caregiver” in this paper) from Pearlin et al. (3), referring to a relative or friend who assists a person who is unable to provide for themselves. In their role, caregivers risk experiencing burden (4) and restrictions in life satisfaction (5) after their partner’s stroke.
The concept of participation has emerged as a central concern in rehabilitation theory and clinical practice (6), is associated with health (7) and is considered an important rehabilitation outcome (8). Mallinson & Hammel (9) defined participation as occurring at the intersection of what a person can do, wants to do, has the opportunity to do, and is not prevented from doing (9). The term “participation in everyday occupations” incorporates the term participation, as used in the World Health Organization’s terminology, with occupation. In this study occupation refers to activities in everyday life that are valued and meaningful for the individual (10). These activities of daily living include, but are not restricted to, occupations as vocations or employment, a common use of the term occupation. The concept of occupation used in this study refers more broadly to activities people need and want to do in general, such as household chores, leisure and social activities. Thus, the concept of participation combined with everyday occupations emphasizes the perceived “doing” and “wanting to do” of everyday activities. Participation in everyday occupations is affected in persons after stroke (11–13). However, there is limited knowledge regarding participation in general for caregivers of persons with stroke (14) and, more specifically, no knowledge about participation in everyday occupations. Furthermore, knowledge about the relationship between the 2 individuals in the stroke-caregiver dyad regarding their participation in everyday occupations after a stroke is lacking.
A dyadic perspective is supported in the results of qualitative studies showing that a stroke affects the everyday activities of the dyad with different patterns of mutual influence and interdependency (15, 16) and where activities in everyday life are enmeshed between the person with stroke and their caregiver (17).
Like participation, life satisfaction is a fundamental rehabilitation outcome (18) for both persons with stroke and their caregivers (19). There is an association between life satisfaction and participation in everyday occupations for persons with stroke (11, 12, 20), but this relationship has not been examined for caregivers. There is also a lack of knowledge regarding the relationship between life satisfaction and participation, not only related to the individual, but also within the dyad.
In previous studies, a dyadic perspective has been achieved by combining the life satisfaction of the 2 individuals (the person with stroke and their caregiver) (21–23). There is an association between a combined high levels of life satisfaction in the dyad, a lower level of caregiver burden and a self-perceived lesser impact of stroke one year post-stroke (21). However, there is a knowledge gap concerning the dyad’s combined life satisfaction and the relationship with participation in everyday occupations, which will be explored in this study.
It has been argued that a family-centred clinical approach is needed within stroke rehabilitation (24), focusing on the persons with stroke together with their caregivers (14, 19). To inform effective rehabilitation interventions with this focus, further research is needed into the perception of the 2 persons in the dyad of their participation in everyday occupations after stroke.
The aim of this study was to explore and describe the perceived participation in everyday occupations of persons with stroke and their caregivers, 3–6 months post-stroke, and to depict this in relation to their global life satisfaction, the dyad’s combined life satisfaction, caregiver burden, perceived impact of stroke and activities of daily living (ADL) ability.
METHODS
Participants
A multicentre study (Life After Stroke–II) provided the participants for the present, cross-sectional study. The multicentre study involved 280 persons diagnosed with a stroke (haemorrhagic or ischaemic) and their identified caregivers. The persons with stroke received treatment at a stroke unit initially, followed by rehabilitation, and were not more than 3 months post-stroke. Inclusion criteria for participants in the multicentre study were that they perceived difficulties in 2 or more ADL activities; had a need of personal or instrumental ADL interventions; had the ability to understand and follow instructions; and had no dementia diagnosis. All participants received information orally and in writing and consented to participate in the study (25).
The participants in the present study represent a subsample of the multicentre study. Inclusion criteria for the participants in the present study were that they had named a caregiver who consented to partake in the study, and that the person with stroke and their caregiver were residing together. Inclusion criteria also included that there was information regarding participation in everyday occupations and global life satisfaction, the 2 main variables of interest.
Procedure
At inclusion in the study, participant information was obtained from medical records and through assessments by research assistants (experienced occupational therapists). Participants were administered the Mini-Mental State Examination (MMSE) (26) to assess cognitive levels and the Barthel Index (BI) (27) to determine levels of ADL.
The National Institute of Health Stroke Scale (NIHSS) (28) for measuring stroke severity in the acute phase was recorded from the patients’ medical records. In cases where NIHSS scores were not available (approximately 10 patients), stroke severity was determined by the first author by extracting information concerning ADL ability in the acute stage from the medical charts and converting it into the Barthel Index scale. The BI scores (0–100) along with the NIHSS were then used to determine levels of stroke severity into mild (NIHSS 0–5/BI 50–100), moderate (NIHSS 6–14/BI 15–49), or severe (NIHSS 15–31/BI < 14) (29).
Data were collected 3 months after inclusion to the study, meaning that data collection could vary after the individual’s stroke between 3 and 6 months. This data collection is hereafter referred to as the 3-month data collection. The data were obtained from the person with stroke either in the clinic or in conjunction with a home visit in face-to face interviews by research assistants. For the caregivers, data were collected during the visit to the person’s home, or if the caregiver was not available, via a postal questionnaire to the caregiver, which was returned by post in a stamped envelope.
Assessments
The present study used the following self-reported assessments:
Occupational Gaps Questionnaire. The OGQ (20, 30, 31) measures participation in everyday occupations. The OGQ is a checklist with 28 different activities dealing with instrumental ADLs, work or work-related activities, leisure and social activities. For each activity, the person is requested to answer yes or no to the questions: (i) Do you perform the activity? and (ii) Do you want to perform the activity? This measures to what extent individuals perceive a discrepancy between what they want to do and what they actually do, and represents an occupational gap. There are 2 different types of gap: (i) when a person does an activity he/she does not want to do (not-want-to-do-gaps); and (ii) when a person does not do an activity that he/she wants to do (want-to-do-gaps). An optimal outcome is a low number of occupational gaps. Based on a study of a Swedish reference-sample (n = 771, age range 20–85 years), 4 or more occupational gaps indicate a restriction in participation for the age group included (age range 18–90 years) in the present study (32). Subjects who did not respond to 2 or more items were excluded as having incomplete OGQ data.
Life Satisfaction Checklist. The LiSat-11 (33) includes 11 items assessing global and domain-specific life satisfaction. The LiSat-11 uses a 6-step, ordinal, self-rating scale, ranging from: (1) “very dissatisfying” to (6) “very satisfying”. The first question concerning global life satisfaction was used.
In order to achieve a dyadic score, the first question concerning global life satisfaction was dichotomized. Scores of 5–6 were considered “satisfied” and scores 1–4 as “dissatisfied”. The developers of the checklist consider this a valid scale reduction (33) and this scale reduction has been used in other stroke studies (5, 30). We then linked the responses of the global life satisfaction question (either satisfied or dissatisfied) for the person with stroke with their caregivers’ to form a combined life satisfaction score for the dyad. We classified the dyad scores as both persons satisfied, both persons dissatisfied, or discordant (i.e. not in agreement). Studies focusing on dyads have used this method previously to combine life satisfaction after stroke (21, 22) and brain injury (23).
In addition to the above, the Stroke Impact Scale 3.0 (SIS) (34) was administered to the participants. The SIS aims at measuring the perceived impact of stroke and comprises 59 items in 8 different domains. The greater the domain score (0–100), the lesser the impact. In addition to the 8 domains, there is a scale of self-assessed recovery, where 100 represents fully recovered and 0 not recovered at all. Furthermore, there is a physical domain consisting of a composite score of the strength, hand function, mobility and ADL/instrumental activities of daily living domains (35).The present study used the physical domain score, the 4 remaining domains of the SIS (memory, communication, emotion and participation) and the SIS recovery scale.
In order to assess the subjective burden of assisting the person with stroke, the caregivers responded to the Caregiver Burden Scale (CBS) (36). The scale encompasses 22 items, dealing with the caregiver’s health, feelings of psychological well-being, social network, relations, physical workload, and environmental aspects. The questions are scored on a scale from 1 to 4; the higher the score (22–88), the greater the burden.
Data analyses
Descriptive statistics were used to report the characteristics of persons with stroke and their caregivers and the results of the OGQ, global life satisfaction from theLiSat-11, the SIS, the BI and the CBS. Differences in the numbers of occupational gaps in the persons with stroke and the caregivers in relation to combined life satisfaction were analysed with the Mann–Whitney U test. Correlations between: (i) global life satisfaction scores for the persons with stroke and their caregivers, and (ii) the number of occupational gaps for persons with stroke and for caregivers and results from their global life satisfaction (scores 1–6), the CBS, the different domains of the SIS and the BI at 3 months post-stroke were determined with Spearman’s rank correlation. The levels of correlation were based on Altman (37) and 0–0.25 was considered as “little if any correlation”; 0.26–0.49 as “low correlation”; 0.50–0.69 as “moderate correlation”; 0.70–0.89 as “high correlation”; and 90–1.0 as “very high correlation”.
Logistic regression analyses were performed with the global life satisfaction (high/low) of the person with stroke, and of the caregiver as dependent variables. Independent variables were the sum of gaps for the person with stroke, the sum of gaps for the caregiver, age and sex.
Statistical significance levels were set at p < 0.05 and confidence levels for calculating confidence intervals (CI) for proportions were set at 95%. Statistica (StatSoft Inc., version 10) was used to perform the analyses.
The study was approved by the regional ethics committee, Stockholm, Sweden.
RESULTS
A total of 105 caregiver dyads (210 persons) met the criteria and were included in the present study. Seventy-seven persons with stroke (73%) were men and the median age of persons with stroke was 70 years (range 46–90 years) (Table I). Eighty of the 105 caregivers (76%) were women and the median age of the caregivers was 68 years (range 18–88 years) (Table II).
Of the 280 persons with stroke comprising the multi-centre rehabilitation study population, 175 were not included in the present study. The mean age of these 175 persons was 73 years (range 36–94 years) and 91 (52%) were men. Ninety-nine persons (57%) did not specify a caregiver. Furthermore, 65 of the remaining persons were not residing with a caregiver, and 11 had incomplete OGQ or LiSat-11 data.
|
Table I. Characteristics of persons with stroke at study inclusion (3–6 months post-stroke) (n = 105) |
|
|
Characteristics |
|
|
Age, years, median (range) |
70 (46–90) |
|
Male/female, n (%) |
77 (73)/28 (27) |
|
Living conditions, n (%) |
|
|
Home or apartment |
105 (100) |
|
Civil status, n (%) |
|
|
Married or cohabiting |
103 (98) |
|
Single |
1 (1) |
|
Born in the country yes/no, n (%)a |
93 (89)/11 (10) |
|
Injury localization/hemisphere, n (%)b |
|
|
Left |
29 (28) |
|
Right |
44 (42) |
|
Other or unspecified |
22 (21) |
|
Stroke severity, n (%)c |
|
|
Mild |
39 (37) |
|
Moderate |
37 (35) |
|
Severe |
9 (8) |
|
Aphasia, n (%) |
|
|
No language impairment |
76 (72) |
|
Language impairment |
29 (28) |
|
Barthel Index, median (QR) MMSE, mean (SD)d |
75 (40) 25.1 (5.6) |
|
SIS recovery (0–100) mean (SD) |
35 (24.2) |
|
Employed yes/no, n (%)a |
28 (27)/76 (72) |
|
Education level, n (%) |
|
|
Elementary school |
38 (36) |
|
High school |
28 (27) |
|
College/university |
34 (32) |
|
Other |
5 (5) |
|
aValid for 104. bValid for 95. cValid for 85. dValid for 101. SD: standard deviation; QR: quartile range. |
|
|
Table II. Caregiver characteristics at study inclusion (3–6 months post-stroke) (n = 105) |
|
|
Characteristics |
|
|
Age, years, median (range)a |
68 (18–88) |
|
Male/female, n (%) |
25 (24)/80 (76) |
|
Education level, n (%)b |
|
|
Elementary school |
36 (34) |
|
High school |
33 (31) |
|
College or university |
25 (24) |
|
Other |
8 (8) |
|
Relationship to the person with stroke, n (%) |
|
|
Partner |
97 (92) |
|
Child |
4 (4) |
|
Sibling |
1 (1) |
|
Other |
3 (3) |
|
Caregiver Burden Scale median (range)a |
43 (22–77) |
|
Time spent with the person with stroke, n (%)c |
|
|
< 8 h/day |
8 (8) |
|
8–12 h/day |
11 (10) |
|
> 12 h/day |
81 (77) |
|
To what % do they know the person with stroke, n (%) |
|
|
55–89% |
8 (8) |
|
90–94% |
11 (10) |
|
> 95% |
86 (82) |
|
Global Life Satisfaction levels, median |
4 |
|
1 (not satisfied), n (%) |
1 (1) |
|
2 (not satisfied), n (%) |
7 (7) |
|
3 (not satisfied), n (%) |
12 (11) |
|
4 (not satisfied), n (%) |
39 (37) |
|
5 (satisfied), n (%) |
31 (29) |
|
6 (satisfied), n (%) |
15 (14) |
|
Hours per week of assistance, mean (SD) |
|
|
Personal ADLd |
4.3 (7.0) |
|
Instrumental ADLe |
9.8 (10.7) |
|
Other assistancef |
7.5 (14.2) |
|
Number of gaps (median, range) |
3.9 (3, 0–19) |
|
Participation restrictions (> 4 occupational gaps), n (%) |
49 (47) |
|
No participation restrictions (< 3 occupational gaps), n (%) |
56 (53) |
|
aValid for 104. bValid for 102. cValid for 100. dValid for 97. eValid for 98. fValid for 95. SD: standard deviation; ADL: activities of daily living. |
|
Number of occupational gaps perceived by persons with stroke, by their caregivers and in the dyad
Table III depicts the activities in the OGQ and the number of gaps perceived by persons with stroke and by the caregivers at the 3-month follow-up. Two persons with stroke and 8 caregivers had one missing item in the OGQ, whereas 4 caregivers did not respond to 2 items. The mean number of occupational gaps registered by persons with stroke was 7.9 (median 7, range 0–23) (Table IV) and by the caregivers 3.9 (median 3, range 0–19). Eighty-seven persons with stroke (83%) (CI ± 7.18) had 4 or more occupational gaps, whereas 49 of the caregivers (47%) (CI ± 9.55) had 4 or more gaps. The caregiver had more occupational gaps than the person with stroke in 15% (n = 16) (CI ± 6.83) of the dyads.
|
Table III. Reported occupational gaps for persons with stroke and their caregivers, (n = 105 dyads) |
||
|
Activity |
Persons with stroke n (%) |
Caregivers n (%) |
|
Instrumental ADL |
||
|
Grocery shopping |
35 (33) |
10 (10)a |
|
Cooking |
38 (36) |
17 (16)a |
|
Doing the laundry |
27 (26) |
12 (11)a |
|
Cleaning |
43 (41) |
26 (25) |
|
Performing light maintenance |
47 (45) |
18 (17) |
|
Performing heavy duty maintenance |
57 (54) |
16 (15)b |
|
Managing personal finances |
25 (24) |
10 (10)b |
|
Transportation |
43 (41) |
9 (9) |
|
Leisure activities |
||
|
Sports |
40 (38) |
32 (30)b |
|
Outdoor life |
47 (45) |
28 (27) |
|
Hobbies |
54 (51) |
17 (16) |
|
Cultural activities |
52 (50) |
33 (31)a |
|
TV/video/radio |
1 (1)a |
5 (5) |
|
Reading newspaper |
12 (11) |
2 (2)a |
|
Reading books or periodicals |
26 (25) |
7 (7) |
|
Writing |
29 (28) |
13 (12) |
|
Playing the lottery, crossword puzzles, etc. |
20 (19) |
11 (10) |
|
Playing computer games & surfing the net |
29 (28) |
12 (11)a |
|
Social activities |
||
|
Visiting partner/children |
0 (0)a |
1 (1) |
|
Visiting relatives/friends |
3 (3) |
2 (4)b |
|
Engaging in societies, clubs or unions |
28 (27) |
9 (9)a |
|
Participating in religious activities |
6 (6) |
7 (7) |
|
Visiting restaurants and bars |
37 (35) |
31 (30) |
|
Travelling for pleasure |
65 (61) |
47 (48)a |
|
Work or work-related activities |
||
|
Working |
30 (29) |
13 (12) |
|
Studying |
14 (13) |
7 (7)a |
|
Taking care of and raising children |
12 (11) |
4 (4)b |
|
Performing voluntary work |
12 (11) |
11 (10) |
|
a1 missing; b2 missing. ADL: activities of daily living. |
||
|
Table IV. Occupational gaps and level of life satisfaction for the persons 3–6 months post-stroke (n = 105) |
|
|
Characteristics for persons post-stroke |
|
|
Number of gaps, mean (median) [range] |
7.9 (7) [0–23] |
|
Participation restrictions (≥ 4 gaps) n (%) |
87 (83) |
|
No participation restrictions (≤ 3 gaps) n (%) |
18 (17) |
|
Global Life Satisfaction levels median, n (%) |
4 |
|
1 (not satisfied) |
5 (5) |
|
2 (not satisfied) |
8 (8) |
|
3 (not satisfied) |
16 (15) |
|
4 (not satisfied) |
32 (30) |
|
5 (satisfied) |
30 (29) |
|
6 (satisfied) |
14 (13) |
Both persons in 46 dyads (44%) (CI ± 9.49) perceived restrictions in participation in everyday occupations, whereas 41 persons with stroke (39%) (CI ± 9.33) perceived restrictions in participation in everyday occupations while their caregiver did not. In 90 dyads (86%) (CI ± 6.64) at least one person in the dyad experienced a restriction in participation in everyday occupations at the 3-month follow-up. Fig. 1 depicts the association between the number of occupational gaps perceived by the person with stroke and by the caregiver.
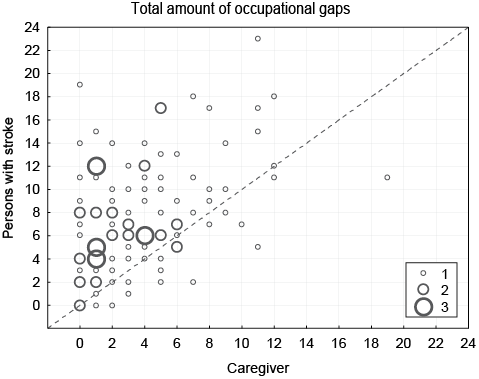
Fig. 1. Association between the numbers of occupational gaps perceived by persons with stroke and by caregivers.
Activities with the greatest number of occupational gaps
For persons with stroke, the greatest numbers of occupational gaps were in the activities of travelling for pleasure (61%), performing heavy-duty maintenance (54%), and hobbies (51%). For the caregivers, the greatest numbers of occupational gaps were in the activities of travelling for pleasure (48%), cultural activities (31%), and both sports and visiting restaurants and bars (30% each).
The predominant type of occupational gap for all activities for the person with stroke was when a person does not do an activity that he or she wants to do (want-to-do-gaps). That was also the predominant type of occupational gap for the caregivers, with the exception of 6 of the 8 instrumental ADL activities. For the activity cleaning, 22% of the caregivers did the activity, but did not want to do it. This type of gap was present for the caregivers in the following activities: cooking (14%), performing light maintenance (11%), doing the laundry (8%), grocery shopping (7%), and managing personal finances (6%).
Combined life satisfaction and occupational gaps in the dyad
Table V presents the results of the combined life satisfaction. Thirty-eight percent of the dyads had a low combined life satisfaction. There was a significantly lower number of gaps (p = 0.003) in persons with stroke in the dyads with combined high life satisfaction compared with those with combined low life satisfaction. This relationship was also true for the caregivers regarding the number of occupational gaps (p = 0.007) (Table V).
|
Table V. Combined life satisfaction and in relation to occupational gaps for persons with stroke and for the caregivers (n = 105) |
|||
|
Combined life satisfaction |
Dyads n (%) |
Occupational gaps for the person with stroke (median/QR/range) |
Occupational gaps for the caregivers (median/QR/range) |
|
High/high |
25 (24) |
5/6/0–17 |
5/3/0–11 |
|
Low/low |
40 (38) |
8.5/4.5/2–18 |
5/5/0–19 |
|
Person with stroke high/caregiver low |
19 (18) |
6/10/0–17 |
3/5/0–9 |
|
Person with stroke low/caregiver high |
21 (20) |
7/6/2–23 |
3/3/0–12 |
|
QR: quartile range. |
|||
Correlations with occupational gaps
The correlations were moderate between the number of occupational gaps for persons with stroke at 3 months and SIS memory domain (R = –0.56), SIS participation (R = –0.54), SIS physical functions (R = –0.5), as well as their self-rated recovery (SIS) (R = –0.53). The correlations were low between the number of occupational gaps for persons with stroke and their global life satisfaction (R = –0.33), and the correlations were also low between the number of occupational gaps for persons with stroke and the caregivers’ number of occupational gaps (R = 0.37) (Table VI and Fig. 1). There was little, if any, correlation in the level of global life satisfaction between the persons with stroke and their caregivers.
|
Table VI. Correlations of the persons with stroke and their caregivers global life satisfaction and the number of occupational gaps for persons with stroke and for the caregivers at the 3-month measurement (n = 105) (Spearman’s rank-order) |
||
|
R |
p |
|
|
Persons with stroke and their caregivers global life satisfaction |
0.201 |
0.03 |
|
Persons’ with stroke number of occupational gaps |
||
|
Caregivers occupational gaps |
0.372 |
< 0.001 |
|
Global life satisfaction |
–0.332 |
< 0.001 |
|
SIS physical functions |
–0.503 |
< 0.001 |
|
SIS memory |
–0.563 |
< 0.001 |
|
SIS communications |
–0.482 |
< 0.001 |
|
SIS emotions |
–0.472 |
< 0.001 |
|
SIS participation |
–0.543 |
< 0.001 |
|
SIS recovery |
–0.533 |
< 0.001 |
|
Barthel Index (3 months post-stroke) |
–0.482 |
< 0.001 |
|
Caregivers’ number of occupational gaps |
||
|
Caregiver Burden Scale |
0.382 |
< 0.001 |
|
Global life satisfaction (caregiver’s) |
–0.312 |
0.001 |
|
SIS participation |
–0.262 |
0.007 |
|
SIS recovery |
–0.211 |
0.02 |
|
SIS physical functions |
–0.211 |
0.02 |
|
Barthel Index |
–0.191 |
0.04 |
|
1R 0–0.25: little if any correlation; 2R 0.26–0.49: low correlation; 3R 0.50–0.69: moderate correlation (Altman, 37). |
||
Correlation between the number of occupational gaps for caregivers and the results of the CBS (R = 0.38) and their global life satisfaction (R = –0.31) were low (Table VI).
The results of logistic regression analysis with the dichotomized global life satisfaction of the person with stroke as the dependent variable showed that persons with stroke life satisfaction accounted for the persons with stroke occupational gaps (OR = 1.1, 95% CI 1.01–1.24, p = 0.03). However, no effect of caregivers occupational gaps on persons’ with stroke life satisfaction could be demonstrated (OR = 1.1, 95% CI 0.94–1.24, p = 0.30).
The results of the logistic regression analysis with the dichotomized global life satisfaction of the caregiver as the dependent variable showed that caregivers’ life satisfaction accounted for the caregivers’ occupational gaps (OR = 1.2, 95% CI 1.0–1.34, p = 0.04). However, no effect of the occupational gaps of persons with stroke on caregivers’ life satisfaction could be demonstrated (OR = 1.02, 95% CI 0.93–1.13, p = 0.64).
DISCUSSION
This is the first study of participation in everyday occupations of persons with stroke and their caregivers. The results showed that 83% of persons with stroke and 47% of their caregivers’ perceived restrictions in participation in everyday occupations, between 3 and 6 months post-stroke. Both persons in 44% of the dyads and at least 1 person in 86% of the dyads perceived restrictions in participation in everyday occupations. There were moderate correlations between the number of occupational gaps reported by the persons with stroke and their self-reported physical functions, memory, participation and recovery. These were rather expected results, since previous studies have found significant associations between the numbers of occupational gaps and participation, as measured by the SIS (11), and with motor impairment in persons after a traumatic brain injury (30).
There were low correlations between the numbers of occupational gaps and life satisfaction for both the persons with stroke and for caregivers, 3–6 months post-stroke. This was a somewhat surprising result, since a previous study (11) showed an association between global life satisfaction and occupational gaps 12 months post-stroke. However, the results of the regression analyses showed that life satisfaction accounted for occupational gaps for the individuals, for both the persons with stroke and for caregivers. With regards to understanding the relationships of participation and life satisfaction within the dyad, the results showed that neither the persons with stroke nor the caregivers’ life satisfaction accounted for the opposite person in the dyads’ occupational gaps. This indicates congruence between participation and life satisfaction within the individual, which has been shown in previous studies (11, 12, 20), but not within the dyad. Yet another way to understand the relationship between participation and life satisfaction within the dyad was to use the combined life satisfaction of the dyad. These results showed that persons with stroke and their caregivers in the dyads with combined low levels of life satisfaction had a greater number of occupational gaps compared with those with combined high levels of life satisfaction. Viewed from this perspective, the results indicate that there is a dyadic influence regarding life satisfaction on participation in everyday occupations. These results illustrate the complexity of achieving a dyadic perspective and emphasize the importance of future research in this area.
Using the combined life satisfaction to focus on the dyad as a unit, the present study found that 38% of the dyads were discordant regarding life satisfaction. Somewhat similar findings using the same life satisfaction measure were found in a Dutch study of couples 3 years post-stroke, where 40% of the couples were discordant (38) and in a Swedish study of couples 1 year post-stroke, where 43% were discordant (22), indicating that the results of the present study are in concordance with previous studies. The results of the Dutch study (38) found that the life satisfaction of the persons with stroke was significantly related to spouses’ life satisfaction. The present study shows little, if any, correlation of life satisfaction between the persons with stroke and their caregivers (see Table VI). These results may be difficult to compare, however, since the Dutch study (38) measured life satisfaction 3 years post-stroke, whereas the present study measured life satisfaction 3–6 months post-stroke.
The activity “travelling for pleasure” had the greatest number of “want-to-do gaps” for persons with stroke and their caregivers (61% and 48%, respectively). Travelling for pleasure appears to be a desired activity performed with ones’ significant other, and impacted by the sequel of stroke. This is supported by other studies reporting that the most frequent perceived problem reported by spouses to persons with stroke was going away on holiday (39) and that relatives’ expressed sorrow concerning the loss of travel (40). Possible cognitive, executive, or mobility issues after a stroke could make travelling a challenge. This in turn, could emphasize the caregiver role, making it difficult for both persons to realize the relative complex activity of travelling and accentuating the influence of a dyadic interaction.
The interactions between the person with stroke and their caregiver on participation in everyday life can be discussed from different angles. Firstly, participation in social activities, such as attending cultural activities and visiting restaurants and bars, activities that had a relatively large percentage of occupational gaps for both the persons with stroke as well as their caregivers, could be impacted by reciprocal relationships within the dyad. For example, if a person because of their stroke does not participate in a social activity that is usually done together with the dyad, the caregiver may chose not to participate because of fundamental changes in the meaning of doing the activity. Another possible dyadic interaction may have to do with changed balances in interdependencies in activities that are usually done together. An example of this might be a couple who are dependent on driving to carry out the shared chore of grocery shopping. The driver, due to the stroke, cannot continue driving; affecting the caregiver’s need to take on all of the driving, or, if this is not possible, forcing the termination of performing the activity in the same way. Future qualitative studies could provide a deeper understanding of the complexities of the interactions of the person with stroke and their influence on the participation and life satisfaction of the 2 persons within the dyad.
Most of the gaps for persons with stroke and for the caregivers were of the type “want-to-do gaps”. The findings showed that the greatest numbers of “want-to-do gaps” for the caregivers were in leisure and some social activities, which are in concurrence with the results of a literature review that found that increased responsibilities and a restriction in interpersonal relationships and leisure activities of the caregivers to persons with stroke affected their social participation (14). It is interesting to note that these findings in light of another finding regarding the type of gap where the caregivers performed activities they did not want to do. This type of occupational gap occurred in 6 of the 8 instrumental ADL activities and indicates that caregivers may perform mandatory activities at the expense of other activities, with a potential imbalance in their activity repertoire. Caregivers may need assistance in the balance of their everyday activities early after stroke so they can avoid jeopardizing their own health. Through identifying persons’ “not-want-to-do gaps”, the OGQ contributes unique information that may lead over and above the realm of participation in everyday occupations by capturing both negative and positive features of participation. These findings show the importance of having a balance in everyday activities and help inform the link with health and wellbeing (41). However, this area needs more research before suggestions can be made for clinical applications.
A moderate correlation between the number of gaps for persons with stroke and for the participation domain of the SIS was expected. A previous study (11) showed the association between the SIS participation domain and the number of occupational gaps, 1 year post-stroke. Both the OGQ and the SIS participation domain measure participation, although different types of participation. The participation domain in the SIS measures social functioning (42), whereas the OGQ measures participation in everyday occupations. Different underlying constructs in these 2 measures could explain the moderate correlation and may indicate that the OGQ gives a distinctive depiction of participation in everyday occupations.
An important finding of the current study is the relatively high numbers of persons (83%) experiencing occupational gaps 3–6 months post-stroke, despite rehabilitation interventions. This indicates the importance of both assessing and intervening regarding issues in participation in everyday occupations and providing effective interventions even after rehabilitation has ceased.
Study limitations
The present study was based on a rehabilitation sample and included participants because of their needs of ADL interventions, and because they lived together with their caregiver, making the results applicable to a percentage of the stroke population that is difficult to determine. Further research would benefit from studies at different time-points or longitudinal studies of this data, to illuminate the possible different stages of participation in everyday occupations after stroke. Moreover, qualitative studies would be beneficial in order to increase our knowledge concerning the dyads’ experiences of participation in everyday occupations.
Conclusion
The results of this study have 2 major implications. First, there is a need to assess participation in everyday occupations after stroke. Rehabilitation professionals may otherwise run the risk of missing pertinent issues in participation in everyday occupations that are of importance to the individual.
Secondly, rehabilitation professionals need to assess different constellations of persons affected by the stroke (i.e. the stroke-caregiver dyad). It is necessary to recognize individual occupational issues as they can differ between the persons in the dyad, but it is also beneficial to recognize shared occupational issues within the dyad. This dyadic and individual perspective may facilitate client- and family-centred interventions focused on the individual as well as on the dyad to achieve a balance in activities in everyday life and reduce occupational gaps through personalized support. However, research is necessary in this complex area regarding rehabilitation interventions with this perspective and their effectiveness in reducing the extent of occupational gaps.
ACKNOWLEDGEMENTS
Financial support was provided by the Health Care Sciences Postgraduate School at Karolinska Institutet. The regional agreement on medical training and clinical research (ALF) between Stockholm County Council and Karolinska Institutet, the Swedish Research Council (VR), the Swedish Council for Working Life and Social Welfare (FAS), RIKS-Strokeförbundet (The Swedish Stroke Association), Uppsala-Örebro Regional Research Council, the Doctoral School in Health Care Sciences at Karolinska Institutet, Strategic Research Program in Care Sciences and Funds at Karolinska Institutet.
REFERENCES

