Roland Stock, MSc1, Gyrd Thrane, MSc2,3, Torunn Askim, PhD4,5, Gunn Karlsen, MSc3, Eli Langørgen, MSc1, Anne Erichsen, MSc6, Ragna Gjone, MSc7 and Audny Anke, MD, PhD3,8
From the 1Department of Physical Medicine and Rehabilitation, Trondheim University Hospital, Trondheim, 2Department of Health and Care Sciences, University of Tromsø, 3Department of Rehabilitation, University Hospital of North Norway, Tromsø, 4Department of Neuroscience, Norwegian University of Science and Technology, 5Department of Physiotherapy, Sør-Trøndelag University College, Trondheim, 6Department of Clinical Services, Oslo University Hospital, Oslo, 7Vestfold Hospital Trust, Clinic Physical Medicine and Rehabilitation, Tønsberg and 8Department of Clinical Medicine, University of Tromsø, Tromsø, Norway
OBJECTIVE: To investigate to what degree patients adhered to a modified constraint-induced movement therapy protocol, and to explore factors associated with the results.
DESIGN: Prospective follow-up of the intervention arm in a randomized controlled trial.
SUBJECTS: Twenty-four patients within 28 days after stroke.
METHODS: The protocol specified 180 min of treatment/day for 10 days. Therapy schedules were used to calculate the time spent in shaping, task practice and transfer package, as well as movement quality, perceived exertion and treatment progression.
RESULTS: The participants spent a mean of 91.3% of the intended time for treatment. Time spent practicing tasks was 30 min less than the intended 150 min, whereas slightly more time than intended was spent on the transfer package. Of the time spent in shaping, 33% was spent in pure activity. The remainder was used on feedback, task set-up, and rests. Adherence was positively associated with treatment progression (r = 0.74) and negatively associated with age (r = –0.65). Women were less likely to use the mitt (r = –0.55).
CONCLUSION: Overall adherence was good; however, time spent in motor activity was only one-third of total treatment time. The parameters in the constraint-induced movement therapy protocol should be individually adjusted early after stroke.
Key words: stroke; constraint-induced movement therapy; adherence; rehabilitation.
J Rehabil Med 2015; 00: 00–00
Correspondence address: Roland Stock, Department of Physical Medicine and Rehabilitation, Trondheim University Hospital, Vådanveien 39, NO-7024 Trondheim, Norway. E-mail: roland.stock@stolav.no
Accepted May 20, 2015; Epub ahead of print Aug 24, 2015
INTRODUCTION
During the last 20 years, constraint-induced movement therapy (CIMT) has evolved as a treatment aiming to improve upper-limb function in patients after a stroke (1). The feasibility of the high-intensity treatment has been questioned by patients and therapists (2–5). Although several meta-analyses (6–9) have found evidence that CIMT applied during the chronic phase is effective, the effect in the early phase after stroke is uncertain (10), and there is limited information about adherence to the treatment (11, 12).
The standard protocol, developed by Taub (1), defines CIMT as 6 h/day of task-specific training during 10 consecutive work-days, and wearing a constraint on the less impaired upper extremity for 90% of waking hours. The protocol distinguishes between adaptive task practice (shaping) and standard task practice (13, 14). An additional component, the transfer package, was added later to transfer activities learned in the therapy to daily life at home (14–17). Adherence to the treatment protocol has been assessed in a sample of patients from the Extremity Constraint Induced Therapy Evaluation (EXCITE) study. The results showed that patients attended a daily supervised therapy session for 6.4 h, but spent only 4 h practising. The training included both shaping and standard task practices of equal duration; however, the investigators did not provide further information (11, 12).
Many modified versions of the treatment (mCIMT) have been developed. These vary in training intensity, the use of constraints, and/or other aspects of the standard protocol (18–27); however, only a few studies have assessed the effect of mCIMT in the early phase after stroke (18, 19, 21, 22, 24). The different results in the trials lead to an uncertainty with regard to the effect of mCIMT in the early phase (10). To better understand the variations in the results and to assess the feasibility of mCIMT applied early after stroke, adherence to the treatment protocol, and the intensity of training (e.g. the amount of pure activity) should be thoroughly assessed. It is also possible that certain baseline characteristics, such as age or sex, can contribute to the understanding of adherence.
The results from the Norwegian constraint-induced therapy multisite trial (NORCIMT) were published recently. The NORCIMT study assessed the effect of a modified CIMT protocol for patients in the early phase, i.e. less than 28 days after stroke. The intervention showed a beneficial effect on arm motor activity and dexterity immediately after the intervention, which was no longer significant after 6 months (28). More knowledge about the adherence to the treatment protocol applied in this study will probably give a better understanding of the temporary effect.
The primary aim of the present study was to investigate to what degree the patients included in the intervention group of the NORCIMT study adhered to the treatment protocol. The secondary aims were to investigate: (i) the associations between treatment time variables and perceived exertion after the training sessions, treatment progression, and quality of movement (QOM); and (ii) whether patients’ age, sex, time since stroke, or motor function influenced adherence to components in the protocol.
METHODS
Design overview
This prospective study assessed patient adherence to the treatment applied in the intervention group of the NORCIMT trial. Details about this single-blinded, multi-centre, randomized controlled trial have been reported previously (28).
Setting and participants
The participants were recruited from 5 Norwegian hospitals: the University Hospital of North Norway, Trondheim University Hospital, Oslo University Hospital, Vestfold Hospital, and Telemark Hospital. Inclusion criteria were: stroke more than 5 days and less than 26 days before enrolment, less than 28 days since stroke at the start of the treatment, either first stroke or second stroke without detectable arm weakness after the first stroke, modified Rankin Scale 0–2 points before admission, persistent unilateral arm or hand paresis (Scandinavian Stroke Scale arm motor function 2–5 points or hand motor function 2–4 points), the ability to lift 2 fingers with the forearm pronated on the table or to extend the wrist at least 10° from fully flexed position, Mini-Mental State Examination score of more than 20 points (or more than 16 points in combination with expressive aphasia), and ability and willingness to sign informed consent. Exclusion criteria were modified Rankin Scale more than 4 points, large hemi-spatial neglect (more than 2 cm on the Line Bisection Test), life expectancy less than 1 year due to other illnesses (e.g. cardiac, malignancy), prior injury or condition in the affected upper extremity that limited use before the stroke, and other neurological conditions affecting motor function. The North Norway Regional Committee of Medical Ethics and the Commission of Privacy Rights at the University Hospital of North Norway reviewed and approved the study (REK NORD 39/2008).
Intervention
The participants who were randomly assigned to the intervention group underwent a modified CIMT programme within 28 days post-stroke. Patients received treatment in 4 rehabilitation centres. In this study, the training records of the patients assigned to the modified CIMT group were used to evaluate patient adherence to the treatment protocol, which was based on the protocol described by Morris et al. (14, 29). Table I summarizes the different treatment components and the adjustments made for the NORCIMT trial. The patients took part in a daily 3 h programme over 10 consecutive working days. Up to 150 min of the treatment was allocated to task training, i.e. shaping (120 min) and standard task practice (30 min). Shaping tasks were characterized by short duration, high number of repetitions, systematic feedback on performance, and successively increasing task difficulty. At least 6 shaping tasks, each consisting of 10 repetitions, were conducted each day. Unlike in the original protocol (14), the therapists were allowed to introduce new exercises if an appropriate exercise could not be found in the bank of shaping tasks. The selected tasks had to be challenging, and, where possible, the difficulty of the shaping tasks was adjusted to a score of 3 (movements were slow or were only made with some effort) on the shaping QOM scale (29). The intended time for standard task practice (more continuously performed activities of longer duration with less frequent feedback, such as writing, ironing clothes, playing the piano, etc.) was 30 min. As part of the transfer package and treatment planning, patients’ usual daily activity patterns were assessed to obtain an overview of daily living activities, interests, hobbies, and habits. We used Goal Attainment Scaling (GAS) to encourage patients to formulate 3 goals related to daily activities (30). The goals set during this procedure formed the basis for choosing activities during task practice and home skill assignment.
In addition, a modified version of the behavioural contract was developed and named “Agreement to participation in treatment”. The contract included a list of activities with and without use of a constraining mitt (up to 90% of waking hours). The daily application of the other parts of the transfer package, i.e. Motor Activity Log, home diary, home skill assignment, and daily schedule, was performed according to the principles of Morris et al. (14). The therapists responsible for the intervention attended a 4-day training programme to familiarize themselves with the study procedures.
|
Table I. Components of constraint-induced movement therapy used in the Norwegian constraint-induced therapy multisite trial (NORCIMT) and modifications from the protocol described by Morris et al. (14) |
||
|
Component |
Modifications in NORCIMT |
Intended duration in NORCIMT |
|
Task practice |
150 min |
|
|
Shaping |
At least 6 shaping tasks per session. New shaping tasks adjusted to functional level allowed. Preferred level of difficulty (quality of movement = 3) |
120 min |
|
Standard task practice |
Goal Attainment Scaling was the basis for choosing tasks |
30 min |
|
Transfer package |
30 min in treatment setting |
|
|
Motor Activity Log |
All 30 questions on the first and last day, alternating 15 questions on the other days |
|
|
Home diary |
None |
|
|
Behavioural contract |
Shorter text, less formal |
|
|
Home skill assignment/ home practice |
None |
30 min outside the treatment setting |
|
Daily schedule |
None |
|
|
Constraint |
||
|
Mitt restraint |
No fingers with firm plastic material on the volar side. One size fits both right and left hands |
90% of 16 waking h (14.4 h or 864 min) |
Measure of adherence
The therapist in charge of the CIMT therapy recorded the starting and stopping time of each shaping/standard task practice session and other treatment components in the daily schedules and used the values to calculate the duration of total treatment time and time spent in shaping exercises, standard task practice, transfer package, and other activities. Longer systematic rest breaks and other activities not directly related to the treatment were excluded from the calculation of total treatment time. For each shaping task, a journal was created that specified the QOM, number of trials, and duration (in s) of each trial. Based on this information, pure shaping activity time (time spent exclusively on activity without rest, feedback, documentation, and set-up) was calculated. The QOM was rated by the therapists, in 0.25 intervals from 0 (no movement) to 5 (normal movement) (29). Task set-up, such as the placement and types of objects used, was recorded in the shaping journal. To facilitate feedback on treatment performance, feedback parameters (e.g. performance time, number of repetitions during a specified time, or reaching distance) was chosen for each set of shaping tasks. After repetition of each task, patients immediately received feedback on their performance. The results were recorded in the shaping journal. Progression parameters were applied, i.e. if performance had increased during the last 5 tasks compared with the preceding 5 tasks, difficulty level was increased. When choosing progression parameters, only 1 aspect (placement, size, weight, or form of a manipulated object) of the task set-up could be changed. The patients recorded the time spent each day on the home skill assignment, using a separate form. Deviations from mitt use during the treatment were recorded, and the home diary was used to calculate the self-reported mitt use outside the therapy setting. Both home skill assignments and the home diary were reviewed jointly by the therapist and the patient each day to strengthen the accuracy of reporting. When the type of activities during home skill assignments, but not the duration, was recorded by the patient, the time was estimated based on the expected minimum number of minutes to carry out the activity. The Borg Scale (31) was used to record perceived exertion after the shaping activities (score 6–20), with a higher score indicating a higher degree of exertion.
Patient characteristics
Age, sex, time since stroke, and the Fugl-Meyer Motor Assessment Score (FMA) were recorded prior to treatment. The FMA measured motor function of the upper extremity (score 0–66), with a higher score indicating better motor function (32).
Statistical analysis
Normally distributed data were presented as mean and standard deviation; non-normally distributed data as median and interquartile range; categorical variables as proportions and percentage. The Shapiro–Wilk test was used to test normality for all treatment variables. Change in treatment duration between days was assessed using paired t-test. To analyse the associations between treatment time variables and patient characteristics as well as treatment parameters, several linear regression analyses were performed with the mean value of total treatment time as well as individual treatment time components, time spent in home exercise, and mitt use as dependent variables. The independent variables that were possibly related to treatment time variables were patient characteristics (age, sex, days post-stroke, and FMA upper extremity score), and treatment parameters (Borg Scale, QOM score, and progression parameters). The association between these variables and the dependent variables were first examined using correlation analyses. Next, for each dependent variable age and sex, as well as possible associations with p-values < 0.1 were included in a linear stepwise multiple regression model. Because of the small sample size, a maximum of 3 independent variables could be included in the model at the same time, and predictors were entered into the model using the forward method. The variable with the lowest p-value was entered first. The next variables were entered singly; only variables with a p-value below 0.05 were included in the final model. Variance inflation factor was used to examine multi-collinearity (a value ≤ 10 was regarded as acceptable) of the independent variables. The residuals were examined to check the model assumptions. SPSS for Windows, version 18, was used to perform all analyses. The level of significance was set at p ≤ 0.05.
RESULTS
The characteristics of the 24 included patients are shown in Table II. Time from onset of stroke to commencement of treatment ranged from 7 to 32 days, with one patient exceeding the 28 days prescribed in the inclusion criteria. The results for the FMA score of the upper extremity ranged from 21 to 62 points.
|
Table II. Participant characteristics (n = 24) |
|
|
Characteristics |
|
|
Age, years, mean (SD) |
65.3 (8.0) |
|
Female, n (%) |
5 (21) |
|
Ischaemic stroke, n (%) |
23 (96) |
|
Right hand affected, n (%) |
10 (42) |
|
Dominant hand affected, n (%) |
16 (67) |
|
Fugl-Meyer Motor Assessment Score upper extremity, median [IQR] |
53.5 [43–59] |
|
Days since stroke, mean (SD) |
16.6 (7.2) |
|
SD: standard deviation; IQR: interquartile range. |
|
Completed treatment sessions
In total, 2 patients withdrew from the study: one on the second day of treatment and another after 8 days (Fig. 1). The data from the first patient were excluded from further analysis, because the patient withdrew before all parts of the treatment were introduced. This patient expressed frustration with the complexity and intensity of the treatment. The second patient withdrew for unknown reasons. Two patients finished their treatment early (1 and 3 days) due to public holidays. Another patient dropped out for 1 treatment day for unknown reasons. These 3 patients missed 5 treatment days in total. When combined with the 12 days from the patients who withdrew, a total of 223 possible treatment days were included, which corresponded to 92.9% (223/240) of the possible sessions completed (the data were based on participating patients, varying from 20 to 23 during the 10 treatment days). Additional missing values from these possible sessions for the other parts of the treatment were 4.5% for the QOM scale, 2.7% for the Borg Scale, 2.4% for mitt use, and 7.3% for home skill assignment. Three patients reported only which home exercises they performed, without specifying how much time they spent on the exercises each day.
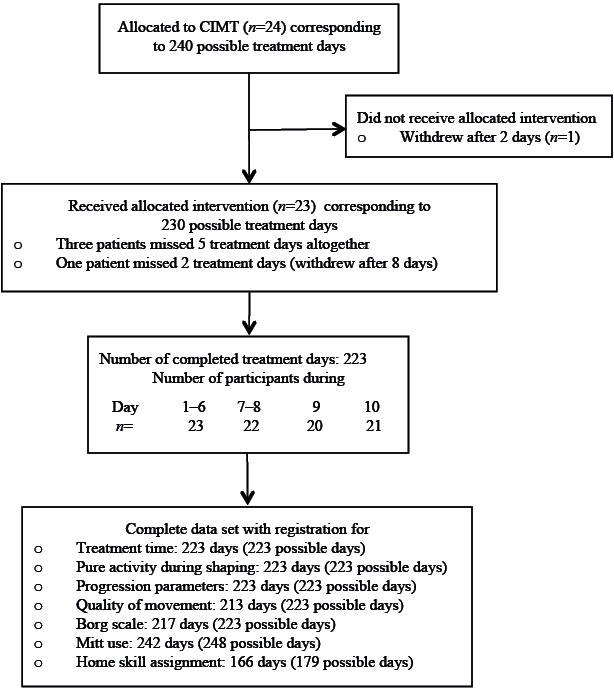
Fig. 1. Completed treatment sessions and missing treatment component and parameter values. Mitt use: 12 days (including weekend), last day excluded because no mitt use after treatment session. Home skill assignment: 8 days (day 2–9).
Duration of the constraint-induced movement therapy treatment
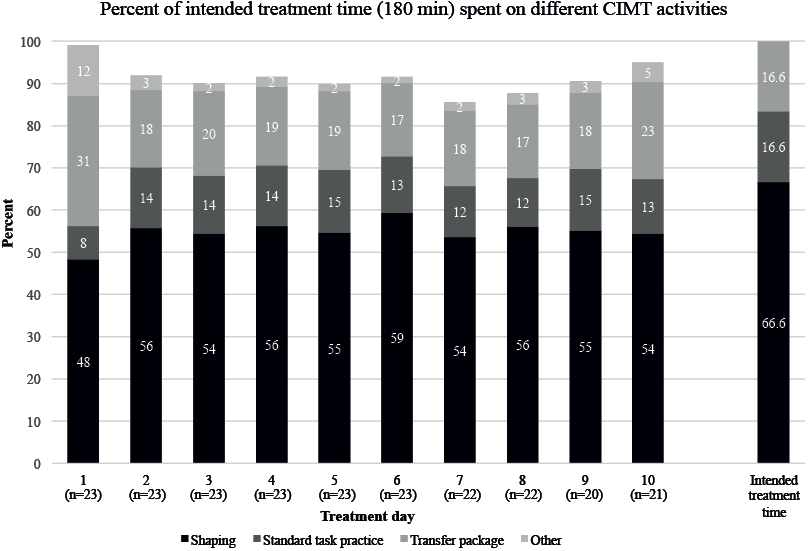
Fig. 2 illustrates the duration of the different CIMT activities as a percentage of 180 min treatment time during the course of the 10 treatment days. The mean daily treatment time was 164.4 min (SD 18.8) or 91.3% of the intended 3 h total treatment time. The range of daily treatment time was 131–186 min. Total daily treatment time did not change significantly (p = 0.08) from the first to the last treatment day. The patients spent 82.2% (mean 98.6 min; SD 15.8 min) of the intended time in shaping activities (120 min intended), 77.3% (mean 23.3 min; SD 11.3 min) in standard task training (30 min intended), and 120.3% (mean 36.1 min; SD 13.0 min) on the transfer package (30 min intended). A mean of 6.4 min (SD 9.5) were spent on activities such as administration of GAS and the Borg Scale. More minutes were devoted to the transfer package during the first treatment day (mean 55.7 min; SD 16.6 min; p < 0.001) and last treatment day (mean 41.4 min; SD 11.0 min; p < 0.001) compared with days 2–9 (mean 32.9 min; SD 6.8 min).
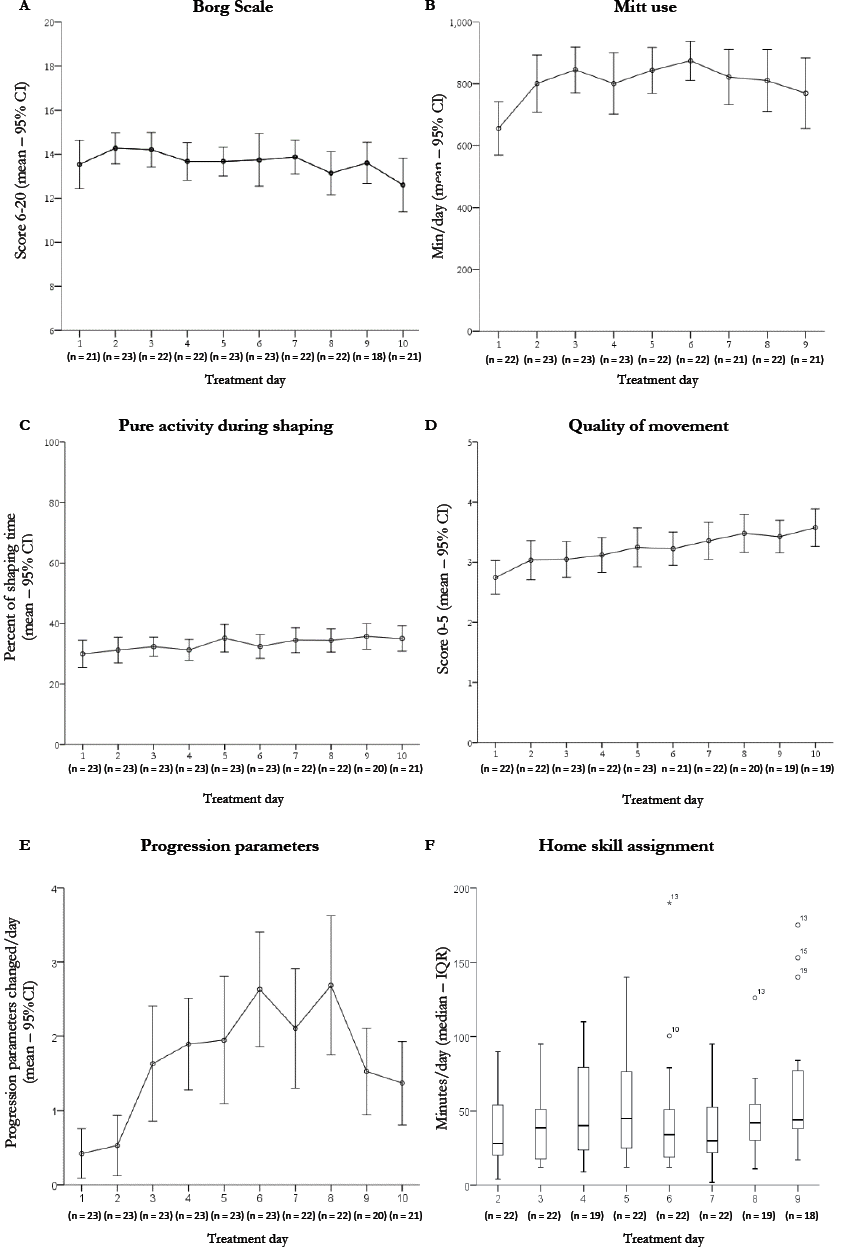
Details of treatment parameters during the 10 treatment days are presented in Fig. 3. Mean Borg score was 13.5 (SD 1.6). Mean mitt use was 12.1 h/day (SD 2.4 h), which made up 75.6% of waking hours. During the treatment days, the patients wore the mitt for 13.0 h/day (81.3% of waking hours), and 8.4 h/day (52.5% of waking hours) during the weekend. Mean mitt use for women was 10.7 h/day (SD 1.9 h), compared with 13.7 h/day for men (SD 2.0 h). One patient was unable to use the mitt during the last 6 days because of eczema. A mean of 32.5 min (SD 8.4 min) were spent on pure activity during shaping, which comprised 33.0% of the total time spent in shaping. Time spent exclusively in motor activity, i.e. pure shaping activity and continuously performed standard task practice, was 55.8 min of 180 intended min (34% of total treatment time). The mean QOM score during the treatment period was 3.4 (SD 0.6), and the mean number of progression parameters changed per day was 1.6 (SD 1.6). The median time spent on home exercise was 39.0 min (interquartile range (IQR) 22–72), ranging from 12 to 155 min.
Regression analyses
In the correlation analyses, the following relationships were noted (p < 0.1), with 1 of the treatment time variables: age was negatively associated with standard task practice (r = –0.65; p < 0.001); female sex was positively associated with transfer package (r = 0.42; p = 0.047) and negatively with mitt use (r = –0.55; p = 0.007); FMA was negatively associated with total treatment time (r = –0.40; p = 0.057) and transfer package (r = –0.45; p = 0.03); QOM (r = –0.47; p = 0.023) was negatively associated with total treatment time; and number progression parameters changed per day was positively associated with total treatment time (r = 0.74; p < 0.001), shaping time (r = 0.41; p = 0.049), and transfer package (r = 0.52; p = 0.011). The results of multiple regression analyses are shown in Table III. Treatment time was positively associated with treatment progression and negatively associated with age, and women were less likely to use the mitt. The models explain 13–52% of the variability in the dependent variables.
|
Table III. Final models of multiple regression analyses for predicting treatment time (min) |
|||||
|
Total treatment time Beta (95% CI) |
Shaping Beta (95% CI) |
Standard task practice Beta (95% CI) |
Transfer package Beta (95% CI) |
Mitt use Beta (95% CI) |
|
|
Demographics |
|||||
|
Age (years) |
ns |
ns |
–0.6 (–0.96 to –0.30) |
ns |
ns |
|
Sex (female) |
ns |
ns |
ns |
6.7 (0.97–12.5) |
–178.2 (–301.8 to –54.6) |
|
Treatment parameters |
|||||
|
Progression parameter |
12.4 (7.2–17.5) |
4.0 (0.01–8.0) |
ns |
4.6 (1.46–7.74) |
ns |
|
Adjusted R-squared |
0.52 |
0.13 |
0.40 |
0.38 |
0.27 |
|
Beta: linear regression coefficient; CI: confidence interval; ns: non-significant. Home exercises showed no significant associations with any of the independent variables and therefore were not included in the table. |
|||||
DISCUSSION
The main finding from the present study was that patients who attended a 3-h CIMT programme within 4 weeks of stroke tended to have a high adherence rate with only some deviations from the treatment protocol. Notably, only about one-third of the treatment time was spent exclusively in motor activity. Furthermore, older age was associated with less time spent in standard task practice. While women spent significantly less time using the mitt than men, they spent significantly more time on transfer package. Treatment progression was positively associated with total treatment time.
Adherence to shaping
A surprising finding was that pure activity during shaping was only 33% of total shaping time. However, the EXCITE trial also acknowledged that their estimate of daily practice time was inflated, because they included non-practice components such as set-up, feedback and brief rests (11). We do not know if the results in our study reflect the nature of shaping, or if the low values are due to the fact that patients need more rest early after stroke than in the chronic phase (11).
The high variation in the patients’ pure activity may indicate that some patients did not tolerate the training intensity well. Birkenmeier et al. (33) showed that subjects with chronic stroke were able to achieve more than 300 repetitions (3 tasks × 100 repetitions) during a 1-h session with high repetition training. The duration of treatment was 78% of the scheduled time. Although this initially seems more efficient than our study’s reports of pure activity during shaping, different methods of calculating activity during training make it difficult to compare pure activity during shaping in our study with Birkenmeier’s reports of activity during high-repetitive training. Nevertheless, it is reasonable to assume that the chronic patients in the high-repetitive training had a higher amount of pure activity and more repetitions compared with the shaping part of our treatment. On the other hand, our patients were encouraged to improve their performance and work as hard as they could during each set of shaping tasks. The high intensity of each set of tasks may have increased the need for rests between the 60–70 sets of shaping tasks, usually consisting of several repetitions. The mean change of 1.6 progression parameters per day, the successive improvements in QOM during the course of the treatment, and the simultaneously stable Borg values measured after shaping exercises reflect the progressive and demanding nature of our tasks.
It is possible that a more distributed application of CIMT (e.g. fewer hours of training per day over a longer period (18) or splitting up the training into 2–3 sessions per day interspersed with longer rest periods) could increase the pure activity time and might be a more effective therapy.
Other aspects of adherence
The number of withdrawals from our study seems to be comparable to studies in both the chronic (34) and the early phase after stroke (19, 22). As other comparable studies (11, 12) did not provide information about all included patients, this makes it difficult to compare data about completed treatment sessions. In contrast to our study, the EXCITE trial reported that patients spent more than the intended time in treatment; however, since they included activities not related to the treatment, accurate comparison is difficult. Regarding mitt use, another study conducted in patients early after stroke (mean 38 days) reported that a constraint was used during nearly 90% of waking hours, as intended (22). A possible explanation for our lower compliance might be that patients in our study began training earlier after stroke. A possible explanation of the hitherto unobserved sex difference in mitt use could be that women spend more time in bimanual housekeeping activities and removed the mitt during these activities. One patient withdrew from our study due to frustration with the treatment. Myint et al. (22) also reported that patients withdrew from their study owing to frustration with using the mitt. Some patients may consider the strict protocol involving mitt use, treatment contract, and home exercise assignments to be “too constraining”. Surveys (2, 4) have confirmed patients’ concerns about mitt use and treatment intensity. Providing detailed information to patients before treatment initiation about the demanding nature of the treatment seems to be crucial to avoid unnecessary frustration and withdrawal.
There was considerable variation among participants with regard to the total task practice time. However, the variability may not be due to the fact that our patients were training early after stroke; the EXCITE trial also reported considerable variations in daily training times in the sub-acute and chronic post-stroke phases (11).
Clinical implications of age and treatment progression
The negative association between standard task practice and age may indicate that older patients need more time for shaping exercises and have less time left for the subsequent standard task practice. The results imply that older patients may benefit more from shorter training durations. The positive association between total treatment time and the number of progression parameters changed per day could be explained by the perception of success and motivational aspects. Progression parameters make treatment progression more obvious and more explicit than verbal feedback alone. Giving feedback on treatment progression and structuring the training so that progression will be more obvious to both patient and therapist may help increase patient motivation and adherence to CIMT training.
Study limitations and strengths
Although we believe our sample was sufficient to highlight the important features of CIMT, a larger sample would permit wider generalization of the results. Another limitation of our study is that several parts of the transfer package were based on self-reported data and may have been swayed by over-reporting. The Borg Scale is frequently used to measure perceived exertion, especially in relation to strength and endurance training; however, there is some doubt as to whether it accurately captures exertion during high-intensity exercise after stroke (35). Additional information about the patients’ subjective experiences with the treatment would have strengthened our results. The study setting required some additional time spent on data registration to be able to give a detailed description of the therapy; however, our impression is that this additional registration did not appreciably bias the registered treatment times. On the contrary, we consider the thorough description of all details and the inclusion of all patients treated with CIMT in an early post-stroke setting to be a strong point for this study. Another important point of the present study is the accurate recording of the time spent in pure activity. Typically, information about the intensity of training in CIMT studies is the intended treatment time, and only 2 studies have reported the actual duration of the treatment (11, 12).
Conclusion
This study showed good overall adherence to a modified CIMT programme; however, the time spent in task practice was less than intended. Pure activity time comprised only one-third of the intended total treatment time. Future CIMT research should focus on which organization or structuring of training yields the best adherence and functional benefit. In particular, the impact of shaping vs standard task practice and the role of the transfer package should be further investigated. Lastly, consideration should be given to whether treatment protocols should be modified according to patients’ age, sex, and stage after stroke. In addition, the impact of adherence and motivation on outcome should be further investigated.
ACKNOWLEDGEMENTS
The authors would like to thank all the co-workers who contributed to this trial: Bent Indredavik for giving critical advice on planning and designing the study; Martin Vatshaug for collating the data for the study and for being responsible for ensuring the quality of data; all therapists and other hospital staff for taking part in providing the treatment, recruitment, and baseline examinations; and all the patients who participated in the study. The study was supported by the Northern Norway Regional Health Authority. The funding sources had no influence on the analysis.
REFERENCES

