Afton M. Koball, PhD1, Julia Craner, PhD2, and Jeannie Sperry, PhD2
From the 1Department of Behavioral Health, Gundersen Health System, La Crosse, WI and 2 Department of Psychiatry and Psychology, Mayo Clinic, Rochester, MN, USA
OBJECTIVE: To examine the impact of weight status on physical and psychological outcomes of patients enrolled in a comprehensive pain rehabilitation programme.
METHODS: Participants (n = 314; mean body mass index 30.34) were administered measures of pain perception, depression, and physical functioning. Analyses included (Group: healthy weight, overweight, obese) × 2 (Time: admission, discharge) mixed-model analysis of variance (ANOVA) models for variables of interest.
RESULTS: All 3 groups of participants evidenced improved pain severity [F(1,311) = 228.94, p < 0.001], pain interference [F(1,311) = 305.93, p < 0.001], pain catastrophizing [F(1,311) = 318.78, p < 0.001], depression [F(1,311) = 191.21, p < 0.001], and physical functioning [F(1,278) = 156.12, p < 0.001] from pre- to post-treatment. No impact of weight status on treatment outcomes emerged. Patients with obesity had lower physical therapy performance scores at both pre- and post-treatment [F(2,278) = 5.98, p = 0.003]; however, results suggested a similar magnitude of physical improvement across all weight ranges.
CONCLUSION: Regardless of weight status, patients achieved improvement in physical and psychological functioning following comprehensive pain rehabilitation. The multidisciplinary nature of this intervention probably resulted in improvements for all patients, including those of higher weight.
Key words: obesity; chronic pain; pain management; rehabilitation.
J Rehabil Med 2016; 48: 632–635
Correspondence address: Afton M. Koball, Behavioral Health, Gundersen Health System, 54601 La Crosse, WI, USA. E-mail: amkoball@gundersenhealth.org
Accepted Apr 14, 2016; Epub ahead of print Jun 16, 2016
INTRODUCTION
The prevalence of obesity and chronic pain has been on the rise for several decades, with approximately 30% of US adults meeting criteria for each condition (1, 2). Perhaps not surprisingly, this association has long been documented. For example, in a recent study, nearly 40% of individuals with obesity also reported chronic pain (3). Another survey of over 1 million respondents found a correlation between obesity and daily pain experiences, with those at the highest weight (body mass index; BMI > 40) experiencing 254% more pain than normal weight counterparts (4). The mechanisms of this relationship are not entirely understood, but are multifactorial, and may include: mechanical and structural factors, metabolic and inflammatory factors, depression, sleep, and lifestyle/behavioural factors (5).
Interventions to manage obesity and chronic pain generally focus on one condition or the other, yet may have reduced efficacy because of a lack of more comprehensive focus. In other words, chronic pain may reduce the efficacy of weight loss interventions, and treatment of chronic pain may be hindered by excess weight (6). One recent study compared outcomes from programmes targeting obesity only (i.e. a behavioural weight management programme; BWM), chronic pain only (i.e. a pain coping skills training; PCST), or obesity + chronic pain (i.e. BWM + PCST) with standard care (7). Results indicated that participants randomized to the BWM + PCST group experienced greater improvements in experience of pain, physical and psychological disability, and weight loss compared with the other groups. Another study comparing the impact of cognitive behavioural pain treatment on patients experiencing low back pain found that obese patients had poorer treatment response (8). Similarly, prior research suggests that weight loss interventions are associated with improved functional status and pain severity among individuals with joint pain (6), and should be considered among first-line interventions for chronic pain.
The goal of the current study was to ascertain the impact of weight status on physical and psychological outcomes of patients enrolled in a comprehensive pain rehabilitation programme. Based on the study by Somers et al. (7) and given that this programme focuses on helping individuals learn to manage chronic pain more effectively (i.e. no behavioural weight management component), it was hypothesized that individuals at higher weight would experience diminished programme benefits.
METHODS
Study participants
Study participants (n = 314; mean age 47.9 years, 67% women) were enrolled in a 3-week comprehensive pain rehabilitation programme at the Mayo Clinic, Rochester, MN, USA. Participants recruited for the study included 404 consecutively enrolled patients from the end of 2013 to 2014 for whom BMI data was collected. Of these, 323 completed the programme, and 314 had complete data, which is how we selected the final sample. Mean BMI was 30.34 (78 normal weight, 85 overweight, 151 obese). Participant characteristics are described in Table I. Ethical clearance was given by the Institutional Research Review Board.
|
Table I. Participant characteristics (n = 314) |
|||
|
|
Healthy weight n = 78 |
Overweight n = 85 |
Obese n = 151 |
|
Body mass index, mean (SD) Age, years, mean (SD) Sex, n (%) Men Women Marital status, n (%) Married Single Separated Divorced Widowed |
22.3 (1.5) 43.2 (14.8)a
19 (24.4) 59 (75.6)
42 (53.8) 24 (30.8) 1 (1.3) 10 (12.8) 1 (1.3) |
27.5 (1.5) 47.4 (15.0)
34 (40.0) 51 (60.0)
56 (65.9) 17 (20.0) 3 (3.5) 7 (2.4) 2 (2.4) |
37.1 (5.8) 51.2 (12.5)
47 (31.1) 104 (68.9)
115 (76.2)b 19 (12.6) 1 (0.7) 7 (8.2) 2 (1.3) |
|
Racial/ethnic group, n (%) Caucasian Asian American American Indian/Alaska Native Other/Chose not to disclose |
74 (94.9) 3 (3.8) 0 1 (1.3) |
81 (95.3) 0 2 (2.4) 2 (2.4) |
143 (94.7) 1 (0.7) 0 7 (4.7) |
|
Opiate use on admission, n (%) Daily morphine equivalence on admission, mean (SD) |
40 (51.3)
96.2 (98.0) |
54 (63.5)
80.7 (57.6) |
88 (58.3)
86.4 (81.0) |
|
Duration of chronic pain, years, mean (SD) |
11.7 (9.9) |
9.4 (9.4) |
11.1 (10.9) |
|
aResults of a 1-way ANOVA indicated that healthy weight patients were younger on average compared with other groups, F(2,311) = 8.84, p < 0.001. bPatients in the obese group were more likely to be married, χ2 (n = 314) = 11.94, p = 0.003. SD: standard deviation. |
|||
Patients were eligible to participate in the pain rehabilitation programme if they met the following criteria: (i) clinically-significant pain (e.g. fibromyalgia, arthritis/joint pain, headache), (ii) pain-related distress/impairment, (iii) psychological factors associated with pain presentation, (iv) symptoms not intentionally produced. Exclusion criteria included: (i) cancer-related pain, (ii) active substance abuse, (iii) suicidality, (iv) active manic or psychotic symptoms requiring a higher level of care.
Intervention
The goal of the programme was to move patients away from “treating” chronic pain (e.g. with opioid medication or seeking out multiple medical procedures) to “managing” chronic pain more effectively utilizing improved coping resources and re-engagement in life activities. The programme consisted primarily of group intervention led by a multidisciplinary team of professionals in pain medicine, physical therapy, occupational therapy, psychology, psychiatry, pharmacology, biofeedback, and nursing. Patients attend the programme for 40 h per week on an outpatient basis. More specific programme details are available from the corresponding author.
Measures
Participants completed computer-based survey measures as part of the admission and discharge process. Physical performance measures were recorded by physical therapists.
West Haven – Yale Multidimensional Pain Inventory (WHYMPI) (9). This 52-item measure assesses dimensions related to pain and functioning. In the current study, the pain severity and pain interference subscales were used. Scores range from 0 to 6. Research suggests good reliability and validity of this measure (9).
Pain Catastrophizing Scale (PCS) (10). The PCS is a 13-item scale assessing the tendency to respond to pain with catastrophic thinking. Total scores range from 0 to 52. Evaluations of this measure have indicated good test-retest and internal consistency reliabilities, as well as high correlations with measures of pain and negative affect (10).
Center for Epidemiological Studies Depression Scale (CESD) (11). The CESD is a widely used 20-item measure of depression in the past week. Total scores range from 0 to 60. Research supports good internal consistency and test-retest reliability for this measure (12).
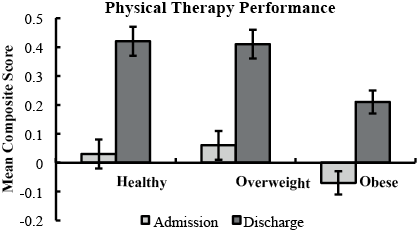
Physical therapy performance. In order to evaluate overall improvements in physical therapy performance, a composite score was developed from therapist-rated performance on the following standardized tasks: Loaded Reach (measured in distance), 5-Minute Walk (distance), and 50-Foot Walk (time). Psychometric evaluation of these measures has indicated good inter-rater reliability, test-retest (within-session) reliability, and moderate correlation with self-reported disability (13). For the current analyses, raw test scores were transformed to z-scores, with discharge z-scores adjusted for performance on admission, and then combined to create a summary measure for the 3 tests (see Fig. 1).
Statistical analysis
Data were analysed using a series of 3 (Group: healthy weight, overweight, obese) × 2 (Time: admission, discharge) mixed-model analysis of variance (ANOVA) models. Given that the categorization of groups (i.e. healthy weight, overweight, obese) resulted in unequal sample sizes, analyses were also conducted using Overall and Spiegel’s method 2 adjustment. Due to group differences in age and marital status (see Table I), these were also accounted for in analyses. However, inclusion of these variables or adjustment due to sample sizes did not impact the significance or interpretation of any findings. Accordingly, these were not included in final analyses in favour of a more parsimonious model. Outliers on all measures were Winsorized to reduce the impact of extreme scores in the database, using a criterion of z-score ± 3.29 for each group.
RESULTS
Pain severity (WHYMPI)
Results indicated a main effect of time F(1,311) = 228.94, p < 0.001, ƞp2 = 0.48. Participants endorsed significantly improved pain severity upon discharge (mean 3.1 (standard deviation (SD) 1.3)) compared with admission (mean 4.3 (SD 1.0)). There was not a main effect of group, F(2,311) = 1.53, p = 0.22, or time×group interaction F(2,311) = 0.66, p = 0.52.
Pain interference (WHYMPI)
As above, there was a significant main effective of time F(1,311) = 305.93, p < 0.001, ƞp2 = 0.50, with participants in all groups reporting decreased pain-related interference at discharge (mean 3.4 (SD 1.2) vs 4.6 (SD 1.0)). There was not a main effect of group, F(2,311) = 2.36, p = 0.10, or time×group interaction F(2,311) = 1.30, p = 0.28.
Pain catastrophizing
Analyses revealed a significant main effect of time, F(1,311) = 318.78, p < 0.001, ƞp2 = 0.51. Consistent with the pattern of results described above, participants reported decreased pain catastrophizing at discharge (mean 13.6 (SD 9.3)) compared with admission (26.2 (SD 11.5)), and there was not a main effect for group, F(2,311) = 0.08, p = 0.92, or time × group interaction, F(2,311) = 0.78, p = 0.46.
Depression (CESD)
There was a significant main effect for time, F(1,311) = 191.21, p < 0.001, ƞp2 = 0.38, indicating that overall, patients reported improved mood at discharge (mean 20.1 (SD 6.1) vs 26.4 (SD 7.9)). As before, there were no between-group differences, including main effect of group, F(2,311) = 0.13, p = 0.88, or time×group interaction, F(2,311) = 2.56, p = 0.08.
Physical therapy performance
Results indicated a main effect of time F(1,278) = 156.12, p < 0.001, ƞp2 = 0.36, indicating that participants in all groups had mean improvements in objectively-measured physical functioning at discharge (0.3 (SD 0.5)) compared with admission (–0.01 (SD 0.5)). There was also a main effect of group, F(2,278) = 5.98, p = 0.003, ƞp2 = 0.04, indicating that patients in the obese group had lower physical therapy performance scores at both time-points. However, there was not a time × group interaction F(2,278) = 1.36, p = 0.26, suggesting that a similar magnitude of improvement was observed across all 3 groups.
DISCUSSION
Patients who experience comorbid obesity and chronic pain are at high risk of poor psychological and physical functioning without proper intervention. Previous research has suggested that pain management interventions alone may not be optimally beneficial for patients also experiencing excess weight (6, 7). Results from the current study indicated that, contrary to the original hypotheses, all participants, regardless of weight status (e.g. normal weight, overweight, obese), can achieve improvements in pain perception, depression, and physical functioning following participation in a comprehensive pain rehabilitation programme that includes physical reconditioning. While results did suggest that participants with obesity had lower physical functioning at both pre- and post-treatment, they made improvements at the same level as patients of lower weight, suggesting similar programme benefits regardless of weight.
Results from this study highlight the benefits of comprehensive pain management programmes on patient functioning, by indicating that a variety of individuals with potential contraindications to treatment (e.g. obesity) can experience physical and psychological improvements in functioning. This is in agreement with previous studies, which have found improvement in outcomes with comprehensive pain rehabilitation programmes (14). These results provide an important addition to the literature on comorbid obesity and chronic pain by informing practitioners about the benefits of multidisciplinary treatment for comorbid conditions. Strengths of this study included utilization of a large sample size and examination of both subjective (self-report psychological functioning and pain perception) and objective (physical therapy functioning) outcomes. Furthermore, this study is the first to our knowledge to directly test the impact of weight on patient outcomes after participation in pain rehabilitation programming, and provides evidence of the strong benefit that these programmes have for patients experiencing chronic pain.
Providers often struggle with knowing how to appropriately treat those experiencing comorbid pain and obesity, and specifically knowing which condition to focus on first. Many may inadvertently believe that treating 1 condition will appropriately resolve the other. Research on patients with chronic pain who undergo bariatric surgery highlights this dilemma, as a recent study suggested that 77% of patients who used opiate medication for pain management pre-surgery, continued to use it post-surgery, and in fact, the majority of patients increased their amount of opioid use (15). Weight loss alone is clearly not sufficient to manage chronic pain, and management of pain alone does not adequately target factors important in weight management (7).
Limitations to this study include a relatively homogenous sample (95% Caucasian, 67% women) which may limit generalizability to more diverse samples. In addition, while previous research has focused on those experiencing joint pain and osteoarthritis (6, 7), patients in the current sample included heterogeneous chronic pain conditions, which may have impacted outcomes. It is also important to note that findings from this study may have, in large part, been observed due to the incredibly comprehensive nature of this programme in particular, as it may not be representative of other pain management programmes (e.g. outpatient weekly cognitive behavioural therapy (CBT)). Participants in this study received 1 lesson on basic nutrition in relation to management of chronic pain from a registered dietician and participated in daily physical therapy activities that increased their level of physical activity and caloric expenditure. While no programming specific to behavioural weight management was given, the cognitive behavioural nature of the intervention, along with an emphasis on physical activity, probably created some overlap in traditional pain management intervention and behavioural weight loss programming. For example, patients received group therapy classes focusing on stress management, goal-setting, planning ahead for barriers to physical activity, and mind-body interventions (e.g. yoga, meditation). Unfortunately, in this study, participant weight was only assessed at admission; thus, we cannot rule out the possibility that participants lost weight over the course of the intervention, and that this may have moderated the improvements they experienced. However, given that the programme is three weeks in duration, it is unlikely that weight loss would have been substantial enough to account for the majority of the physical and psychological gains.
Overall, results from this study support the continued implementation of comprehensive programming for comorbid conditions, and suggests the multi-factorial benefits of pain rehabilitation for individuals of all weight ranges. However, this result may not apply to chronic pain treatment programmes with less comprehensive approaches or lower dose of intervention (e.g. weekly outpatient treatment), warranting further research on this topic.
REFERENCES

