Eugenio Maria Pistone, MSc1, Luca Laudani, PhD1,2, Gianluca Camillieri, MD3, Alessandra Di Cagno, PhD1, Gabriele Tomassi, MD1, Andrea Macaluso, MD, PhD1 and Arrigo Giombini, MD1
From the 1Department of Movement, Human and Health Sciences, University of Rome Foro Italico, Rome, Italy, 2Cardiff School of Sport, Cardiff Metropolitan University, Cardiff, UK and 3MESVA Department, University of L’Aquila, L’Aquila, Italy
OBJECTIVE: To assess the effects of adding a whole-body vibration protocol at optimal frequency (WBV-OF) to a traditional rehabilitation programme (TRP) early after anterior cruciate ligament reconstruction, on maximal strength and balance, in comparison with a traditional rehabilitation programme.
DESIGN: A total of 34 anterior cruciate ligament reconstructed patients with hamstring-tendon graft underwent either 4 weeks of WBV-OF training in addition to a traditional rehabilitation programme, or a traditional rehabilitation programme only, starting from the first month after surgery. Patients were assessed for maximal voluntary isometric strength during both knee extension and flexion and for balance on a force platform before, 1 month after treatment and at 3-month follow-up.
RESULTS: Strength symmetry of the knee flexor muscles improved in WBV-OF+TRP patients more than in TRP patients 1 month after treatment (mean 66% (standard deviation (SD) 15) vs 58% SD 13), and also at the 3-month follow-up (mean 77% (SD 15) vs 64% (SD 15)), with no differences in balance improvements between the groups.
CONCLUSIONS: Adding 4-weeks of WBV-OF to a traditional rehabilitation programme 1 month after surgery is effective in improving muscle strength of the knee flexor muscles. This early intervention may be incorporated into current rehabilitation to facilitate early strength recovery of anterior cruciate ligament reconstructed patients.
Key words: whole-body vibration; anterior cruciate ligament; knee; strength; balance.
J Rehabil Med 2016; 00: 00–00
Correspondence address: Luca Laudani, Cardiff School of Sport, Cardiff Metropolitan University, Cyncoed Road, Cardiff, UK, CF23 6XD. E-mail: llaudani@cardiffmet.ac.uk
Accepted Aug 22, 2016; Epub ahead of print Sep 28, 2016
INTRODUCTION
Anterior cruciate ligament (ACL) rupture of the knee is one of the most commonly diagnosed sports injuries (1). Surgical intervention is indicated to improve mechanical stability of the knee joint and for re-gaining pre-injury level of function (2). It has been reported that patients with ACL reconstruction show clinical deficits in postural control and knee strength, which may persist from 6 months to 4 years (3).
Nowadays, early rehabilitation treatment is recommended immediately after surgery. In the early phase of ACL reconstruction (ACLR) the traditional overload techniques of rehabilitation use an exercise intensity that is insufficient to increase neural drive and to stimulate muscle hypertrophy, because of graft protection. Traditional rehabilitation methods do not allow these problems to be overcome in the early stages, due in particular to the patient’s arthrogenic muscle inhibition (AMI), which is an ongoing reflex inhibition of the quadriceps muscle, leading to the inability to fully activate this muscle (4, 5).
The effectiveness of whole-body vibration (WBV) has been shown in previous studies to be an alternative and safe method for stimulating neuromuscular overload and may be incorporated into current neuromuscular rehabilitation programmes in order to speed up a return to full activity (6–9). Possible mechanisms for improving neuromuscular activation are the ‘’tonic vibration reflex’’ and adaptation of the higher cortex (10). The transmission of mechanical oscillations (30–50 Hz) to the body stimulates many biological systems. This, in turn, may lead to physiological changes at different levels, including stimulation of skin receptors, muscle spindles, joint mechanoreceptors, vestibular system, changes in cerebral activity and changes in neurotransmitter and hormone concentrations. It has also been shown that WBV affects muscle strength and power (6).
Several investigations have been carried out on the effects of WBV training on postural balance, in either healthy individuals (11), or sub-populations, such as elderly people (12), and patients with motor impairments due to stroke (13), cerebral palsy (14) or fibromyalgia (15). These studies present conflicting results, with some supporting its positive effects (11–13) and other showing no changes (16, 17). To our knowledge, there are few studies investigating the effect of WBV during early rehabilitation after ACL reconstruction (18–20) and there is still discussion regarding the time span until the start of the rehabilitation protocol after surgery, duration of the programme or the exercise intensity. The neuromuscular response to WBV has been demonstrated to depend on the type, frequency, amplitude and duration of the oscillator stimulus, as well as on the patient’s body position on the vibration platform (6). Among these factors, the vibration frequency appears to have an important role on the magnitude of the neuromuscular response. An optimal vibration frequency (OVF), which has been defined as the vibration frequency (Hz) at which maximal muscle activation occurs, is always advisable because it potentially produces greater effects on neuromuscular performance in less time (21–24).
The aim of this study is to compare the effects of an early WBV protocol at optimal frequency (WBV-OF), which was added to a traditional rehabilitation programme (TRP), vs a TRP, on maximal strength and balance, after ACL reconstruction. We hypothesized that the protocol with the addition of early WBV led to higher improvements in strength and balance than a TRP in the short term.
METHODS
Participants
From a total of 48 patients who were operated on for an ACL injury at San Giuseppe Hospital, Arezzo, Italy, between September 2014 and January 2016, 34 subjects participated in this open, prospective, randomized controlled study. Demographic and clinical data of the subjects are shown in Table I.
|
Table I. Participant characteristics in the traditional rehabilitation programme (TRP) and whole-body vibration protocol at optimal frequency (WBV-OF)+TRP groups at time 1 |
||
|
TRP n = 17 |
WBV-OF+TRP n = 17 |
|
|
Age, years, mean (SD) Stature, m, mean (SD) Mass, kg, mean (SD) Injury to surgery, days, mean (SD) Lysholm score, mean (SD) Meniscectomy, n |
27 (7) 1.76 (0.08) 73.3 (11.9) 6.5 (3.2) 61.0 (3.3) 5 |
29 (7) 1.75 (0.08) 73.0 (10.7) 6.4 (3.4) 61.7 (3.3) 4 |
|
SD: standard deviation. |
||
All patients enrolled in the study fulfilled the following inclusion criteria: ACL tear with or without concomitant meniscal injury; identical ACL reconstruction surgery by the same surgeon using an ipsilateral tripled semi-tendinosus graft with tightrope for femoral fixation and bioadsorbable interference screw BIORCI-HA for tibial fixation; all subjects had to be non-competitive athletes (Tegner level 9–10). Exclusion criteria were: (i) previous injuries and/or surgery of the knee and other joints of the ipsilateral and contralateral limb: serious cardiovascular or lung disease, pacemaker, acute hernia, discopathy, spondylolysis, severe diabetes, epilepsy, recent infections, that would limit rehabilitation exercise; (ii) no contraindication for performing WBV exercise as reported by Fu et al. (18); and (iii) previous WBV training.
Participants were randomly allocated by using a block randomization program (block size 2) in WBV-OF+TRP and TRP (17 and 17, respectively). The flow of participants is summarized in Fig. 1. This study was approved by the ethics committee of the University of Rome “La Sapienza” and carried out in accordance with the Declaration of Helsinki; explanations were given and informed consent was obtained from all volunteers for participation in the study.
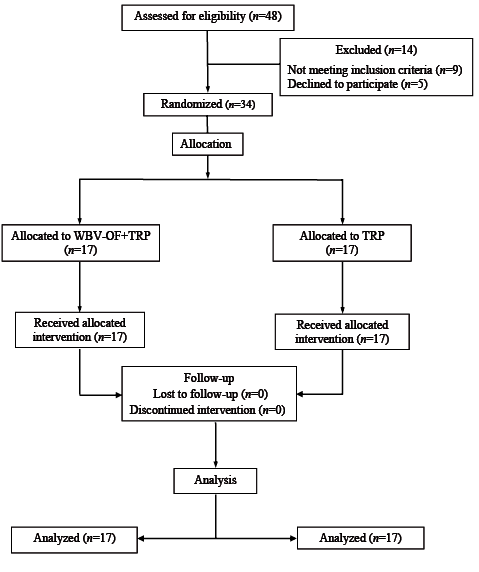
Fig. 1. Patients recruited for the study. WBV-OF: whole-body vibration protocol at optimal frequency; TRP: traditional rehabilitation programme.
Traditional rehabilitation protocol
Both the WBV-OF+TRP and the TRP group underwent the same conventional rehabilitation protocol that was used by the outpatient Physiotherapy Unit of the Institute of Sport Medicine and Science of Rome Italy, under the supervision of physical therapists 5 days per week for the first 3 months of their rehabilitation. Table II details the contents of the rehabilitation protocol. Briefly, the programme consisted of cryotherapy to reduce irritation of damaged tissue, passive motion, strengthening exercise, balance exercise and gait re-education, functional exercise and proprioceptive training. Every session lasted approximately 90 min. Initially, all patients were asked to wear a brace fixed in full extension immediately after surgery and to bear weight on the second day according to tolerance. From the third day, the brace was progressively unlocked up to 90° of knee flexion and kept for 3 weeks. During the first 2 weeks, the rehabilitation programme consisted of continuous passive motion (0–60° in the first week and 60–100° in the second week) and joint and muscle flexibility exercises together with neuromuscular electrical stimulations of the quadriceps, the hamstrings, and the calf muscles, and isometric straight leg rises, which were carried out until the end of the first month. In addition, muscle strengthening 3 times a week started in the fourth week post-surgery and lasted up to the 12th week post-surgery. Thus, the total duration of the rehabilitation programme was 12 weeks. In particular, open kinetic chain exercise of quadriceps, consisting of a seated knee extension within the range of motion of 90–40° with no external resistance starting at the fourth postoperative week, within 90–20° of knee extension at the fifth week, and within 90–0° of knee extension at the sixth week. In both groups the individual optimum intensity and amount of exercise was chosen according to the recommended standards of medical sports exercise (25). Bicycling was allowed for all patients of the 2 groups as soon as knee flexion of the reconstructed leg had reached 110°.
|
Table II. Traditional rehabilitation protocol after anterior cruciate ligament (ACL) reconstruction with tripled hamstrings graft |
||
|
Time |
Week |
Exercises |
|
Day 1–6 |
1 |
Pain control, ankle pumps |
|
Passive terminal knee extension (no hyperextension) |
||
|
Patella mobilization, active assisted knee flexion exercise (in a sitting position) |
||
|
Day 7–15 |
2 |
Manual scar mobilization |
|
Passive terminal knee extension |
||
|
Gait training, core stability exercises (3 × 10 reps) |
||
|
Active knee flexion/hamstring curl (4 × 10 reps) |
||
|
Proprioception and balance exercises |
||
|
Mini-squats (0–45°) with a forward trunk flexion (4×10 reps) |
||
|
Calf raises, strength leg raises (4 × 10 reps) |
||
|
Hip extension, abduction and adduction (3 × 10 reps) |
||
|
Day 16–23 |
3 |
Stationary bicycling when 110° knee joint flexion is reached |
|
Calf raises on a step (4 × 10 reps) |
||
|
Leg press in a device, leg curl in a device (4 × 10 reps) |
||
|
Water exercises |
||
|
Day 24–31 |
4 |
Active knee joint extension 90–40° (3 × 8–10 reps) |
|
Day 32–39 |
5 |
Active knee joint extension 90–20° (3 × 8–10 reps) |
|
Day 40–47 |
6 |
Active knee joint extension 90–0° with gradually increased external-resistance (3 × 8–10 reps) |
|
Day 48–61 |
7–8 |
Active short arc, terminal knee joint extension (no external weights 30–0°; 3 × 10 reps) |
|
Step ups and step down, 1-leg calf raises (4 × 10 reps) |
||
|
Lungs with weights, 1-leg raising from chair (4 × 10 reps) |
||
|
Squats in a device, 2-leg trampoline exercise (4 × 10 reps) |
||
|
Slide board, gait training steps |
||
|
Day 62–76 |
9–10 |
Overall active stretching, full-body strength training |
|
Functional training (jumping on the floor bilateral and single leg) |
||
|
Running on even surface, straight line, 1-leg trampoline exercises |
||
|
Reps: repetitions. |
||
Assessment of optimal vibration frequency
Prior to the experimental intervention, each subject WBV-OF+TRP was tested to identify their OVF. The participants stood barefoot on a vibratory platform (Nemes Double Vibe, Bosco System; OMP, Rieti, Italy) to eliminate any damping of mechanical oscillations that could be due to footwear. As shown in Fig. 2, participants were asked to maintain a static half-squat position with 60° of flexion at the knee joint (full extension: 0°), while distributing their weight mainly over the forefoot (Fig. 2a). A distance of 8 cm was set from the posterior edge of the platform to the heel’s subjects and 5 cm from the median line of the platform and the medial arch of the foot (Fig. 2b). Participants’ upper limbs were positioned with elbow flexed, forearms supinated and their hands just below a railing in front of them. The rationale for the parameter selection was based on several studies that have shown that WBV training with a knee flexion angle of 5–60° leads to beneficial effects on jump height, lower extremity muscle torque and flexibility (22).
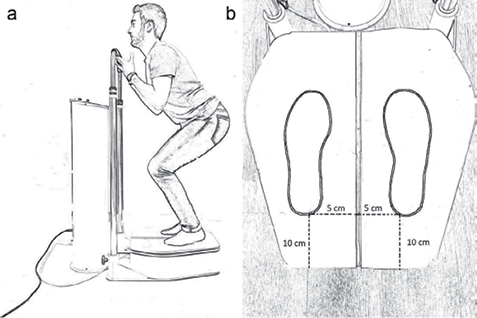
Fig. 2. Standardized (a) body and (b) feet positions maintained through the whole-body vibration sessions.
The vibration protocol for OF consisted of a continuous succession, with no pause, of the following vibration frequencies: 0 (no vibration), 20, 25, 30, 35, 40, 45, 50 Hz. The increase in frequency occurred in steps of 5 s with a total duration of 35 s of vibration preceded by 5 s on the static position without vibration. Throughout the exposure to vibration, the investigators made sure that the participants’ trunk did not lean laterally, the knee angle was held constant, which was checked with a goniometer, and the heels remained without contact with the platform. During the exposure to the WBV subjects were asked to report all sensations, both negative and positive, and were instructed to interrupt the test whenever discomfort was perceived. The peak-to peak amplitude of synchronous vertical oscillations was 2 mm. The vertical component of acceleration was measured using an accelerometer during the incremental test (Type ET-Acc-02, Bosco System Technologies, Rieti) placed in the middle of the vibration platform.
The neuromuscular activity (surface EMG; sEMG) was recorded on the vastus lateralis (VL) muscle of the dominant lower limb, during the execution of the vibration protocol. Two self-adhesive silver/silver chloride electrodes, with a diameter of 4 mm (Blue Sensor Ag/AgCl type NF-00-S/12, Ambu A/S, Ballerup, Denmark) were placed over the vastus lateralis muscle of both limbs with a 20-mm inter-electrode distance according to current recommendations (22). This muscle was considered to be representative of the knee extensors muscle group as in previous studies (22, 23, 26, 27). Before applying the electrodes, the skin was shaved and gently scratched with fine sandpaper. Medical adhesive tape and an elastic band were used to fix the sEMG cables on the skin in order to minimize any motion artefacts that could be encountered during the vibration. The sEMG cables included a pre-amplifier (gain: 1k) and a Butterworth band-pass filter (cut-off frequencies: 8–600 Hz). Signals were then full-wave root mean square (RMS) converted with an averaging time constant of 100 ms and then sampled at 100 Hz by a portable EMG system (MuscleLab 4020e, Ergotest Technology AS, Langesund, Norway), as described previously (23). Test-retest reliability of the sEMG measurements during the continuous incremental WBV protocol has been shown previously to be 0.90 (22).
Mean RMS was computed off-line for each frequency condition (0, 20, 25, 30, 35, 40, 45 and 50 Hz) as the mean value of a central 4-s window within the available 5 s. The RMS values of each WBV frequency from 20 to 45 Hz were then normalized for the RMS value obtained at 0 Hz and expressed as percentages (22). In all participants, the OVF was identified as the WBV frequency with the highest normalized RMS value for each limb. Median value of OVF was 35 Hz (interquartile range 30–45 Hz).
Experimental whole-body vibration protocol
The WBV-OF+TRP group undertook the vibration training in addition to the TRP from 1 month (T1) to 2 months (T2) after surgery. Participants were positioned on the vibration platform as described in the previous paragraph (Fig. 2). The patients were requested to attend 3 sessions per week for 4 weeks for a total of 12 sessions. The protocol was as follows: at week 4: the participants started undergoing 3 series of 1-min WBV bouts at OVF, with 1-min resting between the series; at week 5: 5 series of 1-min WBV bouts at OVF, with 1-min resting between the series; at week 6: 7 series of 1-min WBV bouts at OVF, with 1-min resting between the series; at week 7: 10 series of 1-min.WBV bouts at OVF, with 1-min resting between the series.
Outcome measurements
All patients were assessed for strength, balance and Lysholm Score before treatment, 1 month after surgery (time 1), after treatment, 2 months after surgery (time 2) and at a 3-month follow-up (time 3).
Strength testing. Each patient warmed up on either an exercise bicycle or a step for 5 min at a low resistance before performing the strength test. Participants were tested for maximal isometric voluntary contraction (MVC) of the knee extensor and flexor muscles in each limb (23, 26). During the test, the participants sat comfortably on a custom-made instrumented dynamometric chair, with their trunk erect. They were positioned so that a 90° angle was obtained at the knee joint. Force of the knee extensor and flexor muscles was recorded using a load cell connected to a computerized system unit (MuscleLab; BoscoSystem Technologies, Rieti, Italy). The MVC task consisted of an increase to a maximum in the force exerted by the leg muscles. The participants were able to follow their performance on the computer screen and were verbally encouraged to achieve a maximum and to maintain it for at least 2 s before relaxing. A minimum of 3 attempts was performed separated by 3 min, and that with the highest force value was chosen as the MVC. The participants were asked to make a further attempt if the MVC of their last trial exceeded that of previous trials.
Side-to-side symmetry was quantified for the MVC of the knee extensor and flexor muscles using the limb symmetry index (LSI) at T1, T2 and after 3 months from surgery (T3). For the ACL group, LSI was calculated as the ratio between the involved and the uninvolved limb expressed as a percentage (5).
Balance testing. Postural sway was measured for each foot during quiet standing at T1, T2 and T3. A pressure platform (ZEBRIS, model FDM; 60-Hz sampling frequency) was used to quantify the displacement of the feet centre of foot pressure (COP) with a 60 Hz sampling frequency. Test positions were as follows: (i) standing on 2 legs with eyes open; (ii) standing on 2 legs with eyes closed. Each test position was held for 20 s and repeated 3 times in a random order. Participants were allowed to rest for 60 s in between each test position. Subjects were asked to stand barefoot on the platform with arms crossed at their chest. During the trials with eyes open, participants focused on a target placed 2 m away. The confidence ellipse area of COP displacement was calculated and averaged over the 3 trials for each position, to be used in further analysis.
Lysholm score. A rating system (Lysholm Score) was integrated in this study to check patients’ symptoms, including locking, instability, pain, swelling, ability to climb stairs and squats. It is calculated by a 100-point scoring system and is one of the most often used scales for the assessment of psychometric parameters following knee joint surgery (28).
Statistical analysis
Statistical differences in strength symmetry parameters (LSI of MVC for the knee extensor and flexor muscles), balance measures (confidence ellipse area of COP during eyes open and closed standing) and the Lysholm Score were evaluated by a 2-way repeated-measures analysis of variance (ANOVA) with group (TRP and WBV-OF+TRP) as between-subjects factor and time (T1, T2 and T3) as within-subjects factor. Data were checked for normality and sphericity by the Mauchly test and, when a significant time×group interaction was found, a repeated-measures ANOVA was used to evaluate the significant differences between different times within each group. Unpaired t-tests were used to compare the groups on differences between post-tests and T1 (change scores) at T2 and T3. All analyses were performed using the Statistical Package for the Social Sciences (SPSS) statistical software package (version 20.0; Statistical Package for the Social Sciences, Inc, Chicago, IL, USA). A significance level of p < 0.05 was adopted.
RESULTS
Adherence to protocol
All patients enrolled in the study attended all of the 12 sessions of WBV-OF training.
Strength measures
LSI of knee extension MVC in the TRP and WBV-OF+TRP groups at times 1, 2 and 3 are shown in Fig. 3a. The ANOVA showed a main effect of time (F = 60.75, p < 0.001) on the LSI of the knee extension MVC, which increased to the same extent in both groups from time 1 to time 2 (p < 0.001) and from time 1 to time 3 (p < 0.001).
LSI of the knee flexion MVC in the TRP and WBV-OF+TRP groups at times 1, 2 and 3 are shown in Fig. 3b. The ANOVA showed a main effect of time (F=32.54, p < 0.001) and a significant time×group interaction (Table III) on the LSI of the knee flexion MVC. In the TRP group, the repeated-measures ANOVA showed a main effect of time (F=5.82, p < 0.05) and LSI of knee flexion MVC significantly increased from time 1 to time 3 (p < 0.05). In the WBV-OF+TRP group, the repeated-measures ANOVA showed a main effect of time (F=35.40, p < 0.001) and LSI of knee flexion MVC increased from time 1 to time 2 (p < 0.001), from time 2 to time 3 (p < 0.05) and from time 1 to time 3 (p < 0.001). Pair-wise comparisons showed that LSI of knee flexion MVC was higher in the WBV-OF+TRP than in the TRP group at time 2 (p<0.05) and at time 3 (p < 0.05).
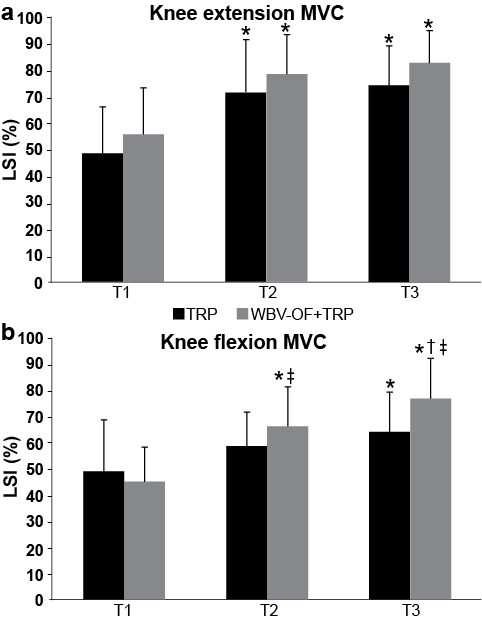
Fig. 3. Limb symmetry index (LSI) of (a) knee extension maximal isometric voluntary contraction (MVC) and (b) knee flexion MVC in the traditional rehabilitation programme (TRP) and whole-body vibration protocol at optimal frequency (WBV-OF+TRP) groups at times 1 (T1), 2 (T2) and 3 (T3). Data are expressed as means and standard deviation (SD). *Significantly different from T1; †significantly different from T2; ‡significant difference between TRP and WBV-OF+TRP groups.
Balance measures
During balance trials with eyes open (Fig. 4a), the ANOVA showed a main effect of time (F=4.21, p < 0.05) and a significant time×group interaction on the confidence ellipse area of COP (Table III). In the TRP group, the repeated-measures ANOVA showed a main effect of time on confidence ellipse area of COP (F=10.38, p < 0.001). In the WBV-OF+TRP group, the repeated-measures ANOVA showed a main effect of time on the confidence ellipse area of COP (F=4.06, p < 0.05). Pair-wise comparisons showed significant difference between TRP and WBV-OF+TRP participants for the confidence ellipse area of COP at time 3 (p < 0.001).
During balance trials with eyes closed (Fig. 4b), the ANOVA showed no significant main effect or interaction, although pair-wise comparisons showed significant difference between TRP and WBV-OF+TRP participants for the confidence ellipse area of COP at time 3 (p < 0.05).
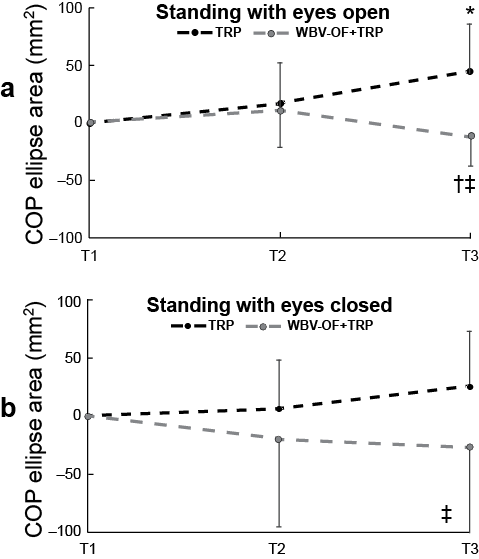
Fig. 4. Mean changes in confidence ellipse area of centre of foot pressure (COP) in the traditional rehabilitation programme (TRP) and whole-body vibration protocol at optimal frequency (WBV-OF)+TRP groups from time 1 (T1) to time 2 (T2) and time 3 (T3) during standing with (a) eyes open and (b) closed. Data are expressed as means and SD. *Significantly different from T1; †significantly different from T2; ‡significant difference between TRP and WBV-OF+TRP groups.
Lysholm score
The ANOVA showed a main effect of time (F=760.74, p < 0.01) and a significant time×group interaction (Table III). Pair-wise comparisons showed that change in Lysholm Score from time 1 was higher in the WBV-OF+TRP than in the TRP group at both time 2 (mean 11.5 (standard deviation (SD) 2.8) and +7.0 (SD 2.7), respectively; p < 0.001) and at time 3 (23.7 (SD 3.4) and 16.3 ± 3.1, respectively; p < 0.001).
|
Table III. Summary of the significant time × group interactions alongside with the pairwise comparison results |
|||||||||||
|
Time × group interaction |
Between-group comparisons |
||||||||||
|
T1–T2 |
T2–T3 |
T1–T3 |
|||||||||
|
F |
p-value |
F |
p-value |
F |
p-value |
F |
p-value |
||||
|
LSI of knee flexion MVC |
4.17 |
0.02 |
0.15 |
0.69 |
5.95 |
0.02 |
0.91 |
0.34 |
|||
|
COP ellipse area (eyes open) |
12.32 |
0.00 |
6.11 |
0.01 |
0.59 |
0.44 |
0.33 |
0.56 |
|||
|
Lysholm score |
26.28 |
0.00 |
8.93 |
0.00 |
48.80 |
0.00 |
21.84 |
0.00 |
|||
|
LSI: limb symmetry index; MVC: maximal isometric voluntary contraction; COP: centre of foot pressure; T1: 1 month; T2: 2 months; T3: 3 months from surgery. |
|||||||||||
DISCUSSION
In this study, for the first time, ACL reconstructed patients who carried out a 4-week WBV training protocol at optimal frequency, starting as early as 1 month after surgery, in addition to a TRP, improved muscle strength of the knee flexor muscles and their Lysholm score more than a matched control group undergoing only a TRP and maintained their greater improvements at the 3-month follow-up. No changes were observed in static balance between the 2 groups after the end of the treatment, thus rejecting the second part of our hypothesis.
Strength measures
Inter-limb symmetry in isometric MVC significantly increased in the 2 groups following the 4 weeks of training (either WBV-OF+TRP or TRP only), and also in the following 4 weeks (TRP in both groups), both during knee extension and flexion, but there was a greater increase in the group who underwent WBV-OF with respect to the TRP group only during knee flexion. It is likely that the position of patients on the vibration platform with weight distribution on the forefoot was effective to give a stimulus of high magnitude in both the hamstring and the ankle plantar-flexor muscles, which are known to contribute to the overall force output during knee flexion MVC (11). The results of our study cannot be directly compared with the results of others investigating the effects of WBV in ACL reconstructed patients because of differences in WBV protocols, strength measurements and surgical techniques. For example, Bershin et al. (20) reported no differences in the improvement of isometric strength of knee flexor muscles after 11 weeks between a protocol consisting of WBV with additional loads, with respect to a traditional rehabilitation protocol. Therefore, it is likely that adding WBV to TRP is more effective than substituting traditional rehabilitation only with WBV. In addition, the clinical population of Bershin et al. (20) was composed of ACL patients reconstructed with patellar-tendon autograft technique, whilst our participants underwent a hamstring tendon autograft technique. Fu et al. (19) compared 8 weeks (twice the duration of our protocol) of conventional rehabilitation or additional WBV therapy starting 1 month after surgery, performed with a single-bundle hamstring approach. Moreover, the authors carried out isokinetic assessments of muscle strength in both knee extensor and flexor muscles, but these outcome measures were performed 3 and 6 months postoperatively, thus making comparisons with our data difficult. Although isokinetic evaluation is 1 of the most common methods for strength testing in ACL patients and has a high reproducibility, it should be underlined that isokinetic movements cannot be performed maximally in the first 2–3 months of recovery after ACL reconstruction, as in our study, and do not reflect functional movements of daily living (29). On the other hand, maximal isometric strength is the maximal force that can be measured in humans (27) and recent findings suggest that isometric assessments following ACL reconstruction show construct validity and sensitivity for monitoring recovery of muscle function comparable to those of isokinetic evaluations (30).
Suggested mechanisms of strength adaptations
Based on previous findings suggesting that WBV would increase muscle activity via the stretch reflex pathway (11), it is reasonable to argue that the enhanced muscle activity in the ACL-reconstructed limb may reflect either an increased excitatory inflow or a decreased inhibitory inflow to the net sum of neural influences acting on the stretch reflex pathway of the knee flexor muscles. In healthy individuals, it has been suggested that providing a vibratory stimulus at the optimal frequency is essential in order to fully maximize the excitatory inflow to motoneurons and, hence, to have a positive effect on the neuromuscular system (7, 22). OVF in ACL-reconstructed patients was in the range 30–45 Hz, which is similar to what has been reported in ACL-injured patients and healthy individuals (7, 22). In ACL-reconstructed patients, vibrating at optimal frequencies may have specifically targeted neuromuscular mechanisms underlying muscle weakness by maximizing the stretch reflex contribution to the overall motor output (7).
Balance measures. The present results do not provide evidence for acute enhancement in balance in WBV-OF+TRP with respect to the TRP after the treatment. This is in contrast with previous studies on the effects of a WBV treatment in ACL patients (18, 19). Such discrepancy might be due to a significant heterogeneity among the studies in the type of balance testing procedures and in the timing of the WBV treatment period with respect to surgery. While, in the previous studies, balance was measured with a Biodex system, which required participants to maintain balance despite a gradually decreasing level of stability due to platform oscillations, in our study participants were asked to simply stand as still as possible on a pressure plate. It might be argued, hence, that the static nature of our balance test would not be sensitive enough to reveal acute improvements in balance ability immediately after the WBV treatment. In addition, there are noticeable divergences in the timing of WBV treatment introduction and, in turn, of balance test delivering across the studies. In Moezy et al. (18), all participants undertook a 4-week WBV treatment starting 3 months after surgery. In Fu et al. (19), participants undertook a 8-week WBV treatment starting 1 month after surgery and were therefore tested for balance after 3 months from surgery. In our study, participants of the WBV-OF+TRP group showed better static balance scores compared with those of the TRP group when evaluated after 3 months from surgery. Overall, hence, these results would suggest that any improvement in balance would become evident after a minimum of 3 months postoperatively.
Lysholm score
The assessment of the subjective rehabilitation progress via Lysholm Score showed that both groups improved, but there were greater improvements in patients who underwent WBV-OF+TRP than patients who underwent TRP only both at the second and third postoperative assessments. This trend is consistent with the improvements in isometric strength of the knee flexor muscles, thus confirming the beneficial effects of adding WBV to TRP.
Intervention safety and compliance
This training programme has been proved to be effective as early as 1 month after surgery. All the patients in the WBV-TRP showed 100% compliance with the WBV training and expressed hope that the protocol could be continued.
Limitations
This study has several limitations that need to be addressed; the limited number of patients, lack of a placebo control group, patients not being blinded, a longer follow-up and lack of objective evaluation of the effects of WBVT on the graft. Further well-conducted prospective randomized controlled studies are needed to address these factors. In addition, testing normal distribution and sphericity have low power in studies with a small number of participants.
Conclusion
This study demonstrated that early WBVT starting one month postoperatively is an effective method to strengthen knee flexor muscles in the lower limb compared with traditional methods that usually aim at one muscle group, with no side-effects and without compromising knee stability. The WBVT group displayed better muscle strength, Lysholm score than the TRP group. WBVT might be an important part of a whole rehabilitation programme, after ACL reconstruction surgery. We suggest incorporating it into current neuromuscular rehabilitation programmes in order to facilitate recovery, starting from 1 month postoperatively.
REFERENCES

