Mia Forslin, MSc1,2, Anders Kottorp, PhD3,4, Marie Kierkegaard, PhD1,5 and Sverker Johansson, PhD1,5
From the 1Division of Physiotherapy, Department of Neurobiology, Care Sciences and Society, Karolinska Institutet, 2Rehab Station Stockholm, Solna, Sweden, 3Department of Occupational Therapy, University of Illinois at Chicago (UIC), Chicago, USA, 4Division of Occupational Therapy, Department of Neurobiology, Care Sciences and Society and 5Functional Area Occupational Therapy & Physiotherapy, Karolinska University Hospital, Stockholm, Sweden
OBJECTIVES: To translate and culturally adapt the Acceptance of Chronic Health Conditions (ACHC) Scale for people with multiple sclerosis into Swedish, and to analyse the psychometric properties of the Swedish version.
SUBJECTS: Ten people with multiple sclerosis participated in translation and cultural adaptation of the ACHC Scale; 148 people with multiple sclerosis were included in evaluation of the psychometric properties of the scale.
METHODS: Translation and cultural adaptation were carried out through translation and back-translation, by expert committee evaluation and pre-test with cognitive interviews in people with multiple sclerosis. The psychometric properties of the Swedish version were evaluated using Rasch analysis.
RESULTS: The Swedish version of the ACHC Scale was an acceptable equivalent to the original version. Seven of the original 10 items fitted the Rasch model and demonstrated ability to separate between groups. A 5-item version, including 2 items and 3 super-items, demonstrated better psychometric properties, but lower ability to separate between groups.
CONCLUSION: The Swedish version of the ACHC Scale with the original 10 items did not fit the Rasch model. Two solutions, either with 7 items (ACHC-7) or with 2 items and 3 super-items (ACHC-5), demonstrated acceptable psychometric properties. Use of the ACHC-5 Scale with super-items is recommended, since this solution adjusts for local dependency among items.
Key words: acceptance; measurement; multiple sclerosis; Rasch; questionnaire; scale; Acceptance of Chronic Health Conditions Scale.
J Rehabil Med 2016; 00: 00–00
Correspondence address: Sverker Johansson, Division of Neurology R54, Karolinska University Hospital, Huddinge, SE–141 86 Stockholm, Sweden. E-mail: sverker.johansson@ki.se
Accepted Aug 22, 2016; Epub ahead of print Sep 28, 2016
INTRODUCTION
Multiple sclerosis (MS), a chronic neuroinflammatory and neurodegenerative disease, is the leading cause of neurological disability in younger adults (1). The course of the disease is unpredictable, it progresses over time and causes a wide range of disabilities (2) with potentially profound effects on many areas of life (3).
People with MS (PwMS) experience decreased health-related quality of life (HRQoL) compared with the general population and compared with those with other chronic conditions (4). This is also evident early in the course of the disease, when the level of disability is low (5). Even though the physical dimensions of HRQoL deteriorate over time for most PwMS, psychological dimensions can remain stable or improve (6, 7). Studies indicate that acceptance of the condition is associated with better quality of life (QoL) in PwMS (8–10). This could have implications for interventions intended to improve QoL (11, 12). However, it is unclear when and in what way acceptance can be used to improve QoL, and to what extent it is essential for experiencing better QoL in MS.
To measure acceptance in chronic health conditions, the Acceptance of Chronic Health Conditions (ACHC) Scale was developed by Stuifbergen et al. (13). This scale is based on the experiences of persons living with MS and represents a view in which the chronic condition is one of many characteristics of a person’s life and not necessarily the defining characteristic (13). To accept a condition in this view does not imply passive resignation or absence of efforts to improve one’s situation. Instead it supports the notion of being able to integrate the chronic condition into one’s life and, through this, being able to focus on what can be changed rather than on what cannot be changed; that is to say, being diagnosed with a chronic condition.
The ACHC Scale (13) consists of 10 items scored on a 5-category Likert rating scale (Table I). Four items are positively worded, and 6 negatively worded. The ratings are summed; in the summation of the score the positively worded items are coded in reverse. A high total sum score indicates a high level of acceptance, whereas a low sum score indicates a low level of acceptance. The psychometric properties of the scale were found to be satisfactory using classical test theory approach (13).
|
Table I. Acceptance of Chronic Health Conditions Scale, original version |
|
Items |
|
1. I feel I’ve come to terms with my MS. |
|
2. I’d give all the money I have to get rid of my MS. |
|
3. I think of my MS as a curse. |
|
4. I can’t conquer MS, but I can adapt to it. |
|
5. My fondest dream is that I’ll awaken some morning without my MS. |
|
6. Having a disease like MS is just part of life. |
|
7. My MS is a major focal point in my life. |
|
8. I spend a lot of time wondering why I have MS. |
|
9. I think of my MS as just a part of who I am. |
|
10. I think a lot about what my life would be like without MS. |
|
Response categories on a Likert rating scale |
|
1 = Strongly Agree |
|
2 = Agree |
|
3 = Not Sure |
|
4 = Disagree |
|
5 = Strongly Disagree |
|
MS: multiple sclerosis. |
To be able to measure acceptance of chronic health conditions in a Swedish context, with the intent to further explore the value of acceptance in MS, a valid and reliable measurement tool is needed. The aims of this study were therefore to translate and culturally adapt the ACHC Scale for PwMS into Swedish, and to analyse the psychometric properties of the Swedish version.
METHODS
Participants and procedures
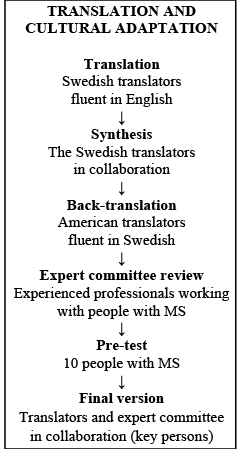
Translation and cultural adaptation of the ACHC Scale were performed in steps (Fig. 1) based on recommended guidelines (14, 15). In the first step, the scale was translated from English into Swedish independently by 3 translators of Swedish origin, who then agreed on a synthesis of the 3 versions. In the next step the synthesis was back-translated into English by 2 independent translators of American origin. All the translators were competent in both the source and target languages. Notes were made throughout the translation process describing aspects taken into consideration during the translation. In the next step an expert committee reviewed all the translations and the notes taken by the translators. The expert committee was comprised of health professionals with extensive experience in outpatient and inpatient care of PwMS. The review focused on similarity between the original and the Swedish version of the ACHC Scale concerning conceptual, experiential, operational and idiomatic equivalence. The expert committee produced a revised Swedish version of the ACHC Scale, which was then used in the pre-test, the final step of the translation and cultural adaptation. In the pre-test, 10 PwMS (Table II) filled in the expert committee’s Swedish version of the ACHC Scale while they reflected on each item, the scale as a whole and the instructions for the scale. After completing the scale, the PwMS were informed of the view of acceptance that the scale intended to reflect. They were then asked whether the items, in their view, represented the intention of the scale. Some final revisions of wording were made based on the pre-test, and then the final version was decided upon.
Fig. 1. Translation and cultural adaptation into Swedish of the Acceptance of Chronic Health Conditions Scale.
|
Table II. Demographic and clinical characteristics of the 10 persons with multiple sclerosis who in the pre-test reflected on the Swedish version of the Acceptance of Chronic Health Conditions Scale |
|
|
Characteristics |
|
|
Sample, men/women, n |
2/8 |
|
Age, years, range |
28–66 |
|
Living with partner, n |
7 |
|
< 65 years of age, n |
9 |
|
Working full-time or part-time (persons < 65 years of age) , n |
3 |
|
Movement ability, n |
|
|
Walking without difficulty/with difficulty |
5/2 |
|
Driving wheelchair without difficulty/with difficulty |
2/3 |
|
Bedridden |
1 |
|
Years since diagnosis, range |
1–28 |
For the purpose of evaluating the psychometric properties of the Swedish version of the ACHC Scale, it was included in the data collection of a 10-year follow-up of a previously described study of an MS cohort in Stockholm, Sweden (16, 17). For data collection at baseline 10 years previously, those PwMS were eligible who were scheduled for an outpatient appointment with senior neurologists at an MS Centre; a total of 219 PwMS were included, and, of these, 200 were followed for 2 years. For the 10-year follow-up, the 200 PwMS were re-identified, of these 155 PwMS were included after giving informed consent. Data collection took place at the MS centre or through a home visit, according to the preference of the participant. A research physiotherapist was present during data collection, guiding the participant through the test battery. In a few cases, data was collected via post and telephone.
Data collection in the 10-year follow-up was performed through structured interviews, with a wide range of standardized instruments focusing on various aspects of disabilities known to commonly occur in MS, and the ACHC Scale. Out of the 155 PwMS included in the 10-year follow-up, 148 PwMS (Table III) completed the ACHC Scale. Reasons for not completing the scale were either being not capable of doing so (n = 6) or choosing not to due to language difficulties (n = 1).
In the present study data from the 10-year follow-up on the following variables was used: sex, age, time since diagnosis, and disease severity as determined by the Expanded Disability Status Scale (EDSS; 18). In addition, data on the ACHC Scale was used.
|
Table III. Demographic and clinical characteristics of the sample of people with multiple sclerosis who completed the Acceptance of Chronic Health Conditions Scale for analysis of psychometric properties |
|
|
Sample, n |
148 |
|
Women, n (%) |
98 (67) |
|
Age, years, mean/median (min–max) |
52/55 (30–84) |
|
< 65 years of age, n (%) |
116 (79) |
|
Working full- or part-time (persons < 65 years of age), n (%) |
59 (51) |
|
Disease severity, n (%) |
|
|
EDSS normal, 0 |
4 (3) |
|
EDSS mild, 1–3.5 |
61 (41) |
|
EDSS moderate, 4–5.5 |
18 (12) |
|
EDSS severe, 6–9.5 |
64 (44) |
|
Years since diagnosis, mean/median (min–max) |
23/20 (11–52) |
|
EDSS: Expanded Disability Status Scale. |
|
The study was approved by the Regional Ethical Review Board in Stockholm.
Statistical analysis
Psychometric properties of the ACHC Scale were analysed using WINSTEPS Rasch analysis software (19). Compared with an analysis using the classical test theory approach, an approach using the Rasch model can increase the information regarding a scale’s properties (20, 21). In the Rasch model, the ordinal data pattern across items can be converted into interval measures if the empirical data meets certain criteria of validity and reliability (20). An introduction to Rasch analysis can be found in dedicated articles and textbooks (20–23). As a generic rating scale is used across all items in the ACHC Scale, the Andrich Rating scale model was chosen for analysis, assuming that the rating scale functions in the same manner across items. In the evaluation of the psychometric properties of the ACHC Scale in this study, an earlier established stepwise procedure (Table IV), described in detail elsewhere (24), was used. In addition, an item-person map was used to assess how well the items targeted the participants in the present study (22).
|
Table IV. Overview of the analytic process of the Rasch analysis |
|||
|
Step |
Psychometric property |
Statistical approach |
Criteria |
|
1 |
Rating scale functioning |
Mean measures for each step category and threshold on each item should advance monotonically (20) |
z-values < 2.0 in outfit mean square (MnSq) values for step category calibrations (25) |
|
2 |
Internal scale validity: Item goodness-of-fit |
Item goodness-of-fit statisticsa (26) |
Infitb MnSq values ≤ 1.4 and z-value < 2.0 (27, 28) |
|
3 |
Internal scale validity: unidimensionality |
Principal component analysis of the residuals (29) |
≥ 60 % of total variance explained by first component (i.e. acceptance) (30) Any additional component explains < 5% of the remaining variance of residuals after removing first component (30) |
|
4 |
Person-response validity |
Person goodness-of-fit statistics |
Person goodness-of-fit infit values ≤ 1.4 and z-value < 2.0 (27, 28) ≤ 5% of sample fails to demonstrate tolerable goodness-of-fit values (27) |
|
5 |
Person-separation reliability |
Person-separation index (31) |
≥ 1.5 for group use and ≥ 2.5 for individual use (20) |
|
6 |
Internal consistency |
Cronbach’s alpha coefficient |
≥ 0.7 for group use and ≥ 0.85 for individual use (20) |
|
7 |
DIFc |
Mantel-Haenszel statistic (32) |
p < 0.01 with Bonferroni correction (32) No more than 1 item, or 5% of items, is allowed to demonstrate DIF (28) |
|
aIn presence of item misfit, misfitting items were successively excluded until no misfit appeared. bIn this study the infit values were used in the analysis since they are considered to be more sensitive to item performance and more informative when exploring internal scale validity than the outfit values (33). cRegarding sex, age, time since diagnosis and disease severity determined by the Expanded Disability Status Scale (EDSS; 18). Age and time since diagnosis were categorized in 2 groups based on the median in the cohort, and the EDSS scores were categorized based on illness severity, EDSS mild and EDSS moderate/severe. DIF: differential item functioning. |
|||
Finally, in order to ensure that the 7-item version was the most optimal valid version of the ACHC scale, an additional Rasch approach to validate the ACHC scale was used: as local independence of items is an underlying assumption within the Rasch model, an initial exploration of the residual correlations between the initial 10 ACHC items was calculated. We decided that item clusters with correlations exceeding 0.2 above the mean item residual correlations should be grouped into so called “super-items” and may then be re-evaluated towards the similar criteria. This additional approach will reveal whether the original item deletion generated the most optimal solution for the ACHC scale, or if the item deletion was biased by local dependence among items.
RESULTS
Translation and cultural adaptation
The Swedish version of the ACHC Scale was considered to be a satisfactory equivalent to the original version in all of the aspects of equivalence reviewed. The concept of acceptance in the original version of the scale was equivalent to how acceptance can be viewed in a Swedish context. However, in the expert committee, acceptance was viewed as a complex concept that can be interpreted in different ways. In the pre-testing, the PwMS confirmed that the definition of acceptance used in this study was represented in the scale, but that acceptance could also be viewed in other ways. The PwMS also indicated that there may be a difference between emotional and intellectual acceptance, and that acceptance may change over time, as it is challenged by every exacerbation as well as other demanding life events. It was a belief in both the expert committee and among the PwMS that acceptance, as defined in this study, is important to well-being in PwMS, which is consistent with what is conveyed in the original description of the scale.
The conceptual and experiential equivalence were most challenged in item #3, in which the expression “curse” was used, and in items #6 and #9 where the expression “just a part of” was used. First, it was considered in the expert committee review whether the use of the word “curse” in the original version could be an expression of a more religious foundation in the original culture than in the Swedish culture. The expert committee concluded that it was probably more a matter of finding a corresponding idiomatic expression. Secondly, the items with the expression “just a part of” were found to be somewhat provocative by the PwMS, because some felt that the expression tended to diminish the consequences of MS. Even though this could have to do with different views of acceptance and experiential background in the respective cultures, the difference was considered negligible. Thus, conceptual and experiential equivalence was thought to have been achieved.
There were some difficulties in relation to operational equivalence: the labelling and the layout of the rating categories, and item #4. Both the expert committee and the PwMS were concerned about the middle rating category, “not sure”, whether “not sure” implies that you do not know, or whether it is an alternative in the middle of “agree” and “disagree”. In item #4 both the PwMS and the expert committee pointed out the possibility of agreeing with 1 part of the item, for example: “I can’t conquer MS”, but not the other, “but I can adapt to it”, which could make the item difficult to respond to. Despite these difficulties, the ACHC Scale was thought to operate in a similar manner in a Swedish context, as in the original context. In addition, both the expert committee and the PwMS considered the ACHC Scale to cover an aspect of having MS that was not usually addressed by the Swedish healthcare services.
Idiomatic equivalence between the original and the final Swedish version of the ACHC Scale was considered to have been achieved during the translation process. In 3 items a different expression was used in the Swedish version, due to different ways of expressing the intended meaning in the original version. These items were: item #1 with the expression “come to terms with”; item #3, “curse”; and item #7, “focal point”. Most items in the scale were considered by the expert committee to be expressed in English based on spoken language. In the translation from the original into Swedish this was sought to be conveyed, while the back-translations were expressed in more formal English. These differences were discussed and resolved both in the expert committee review and the review after the pre-testing, in order to assure idiomatic equivalence.
Psychometric properties of the Swedish version
The Rasch analysis demonstrated the most favourable psychometric properties in a solution, including 7 of the 10 items in the ACHC Scale; key points leading to this result are presented step by step below and in Table V.
|
Table V. Psychometric properties of the different item solutions of the Acceptance of Chronic Health Conditions (ACHC) Scale (Swedish version), overview of the analytic process |
|||||
|
ACHC-10 |
ACHC-9 Item #9 excluded |
ACHC-8 Items #9 and #4 excluded |
ACHC-7 Items #9, #4 and #6 excluded |
ACHC-5 (including 2 items and 3 super-items) |
|
|
Rating scale functioning |
All items met criteria Outfit MnSq z-value ranged from 0.77 to 1.30 |
All items met criteria Outfit MnSq z-value ranged from 0.73 to 1.39 |
All items met criteria Outfit MnSq z-value ranged from 0.74 to 1.42 |
All items met criteria Outfit MnSq z-value ranged from 0.83 to 1.63 |
All items met criteria Outfit MnSq z-value ranged from 0.60 to 1.86 |
|
Internal scale validity: Item goodness-of-fit |
Item #9 failed to meet criteria, infit MnSq was 1.75 and z-value was 5.6 |
Item #4 close to not meet criteria, infit MnSq was 1.29 and z-value was 1.9 |
Item #6 failed to meet criteria, infit MnSq was 1.42 and z-value was 3.0 |
All items met criteria |
All items met criteria |
|
Internal scale validity: Uni-dimensionality |
First component failed to meet criteria, explaining 48.7% of total variance Second component failed to meet criteria, explaining 14.0% |
First component failed to meet criteria, explaining 57.3% of total variance Second component failed to meet criteria, explaining 10.8% |
First component failed to meet criteria, explaining 58.7% of total variance Second component failed to meet criteria, explaining 9.2% |
First component met criteria, explaining 63.6% of total variance Second component failed to meet criteria, explaining 9.0% |
First component met criteria, explaining 91.1% of total variance Second component met criteria, explaining 2.7% |
|
Person-response validity |
8.1% of sample failed to meet criteria |
8.1% of sample failed to meet criteria |
6.8% of sample failed to meet criteria |
6.8% of sample failed to meet criteria |
4.8% of sample failed to meet criteria |
|
Person-separation reliability |
Met criteria for group use, person separation index 1.6 |
Met criteria for group use, person separation index 1.9 |
Met criteria for group use, person separation index 1.9 |
Met criteria for group use, person separation index 2.0 |
Met criteria for group use, person separation index 1.73 |
|
Internal consistency |
Met criteria for group use but not individual use, Cronbach’s alpha coefficient 0.80 |
Met criteria for group but not individual use, Cronbach’s alpha coefficient 0.84 |
Met criteria for group but not individual use, Cronbach’s alpha coefficient 0.84 |
Met criteria for individual use, Cronbach’s alpha coefficient 0.85 |
Met criteria for group but not individual use, Cronbach’s alpha coefficient 0.76 |
|
Differential item functioning (DIF) |
Item #2: easier to agree with for women than men (p <0.01) Item #7: easier to agree with for men than women (p < 0.01) |
||||
In the first step, the functioning of the rating scale was evaluated. The 5 category generic rating scale met the criteria for acceptable rating scale functioning. Categories 4 and 5 were more commonly used; Categories 2 and 3 were the least used.
In the second step, item goodness-of-fit to the Rasch model was analysed. Items were excluded when demonstrating misfit. In the analysis, item #9 demonstrated misfit and was excluded. In the continued evaluation, item #4 was close to demonstrating misfit, and in combination with other aspects of the Rasch analysis that were not satisfactory, item #4 was also excluded. When both items #9 and #4 were excluded, item 6 demonstrated misfit. After having excluded items #9, #4 and #6, 7 items remained (the ACHC-7 Scale), and no more items appeared as misfit. From this step on, the results from the ACHC-7 Scale are primarily presented.
The third step evaluated unidimensionality. In the ACHC-7 Scale, unidimensionality was indicated, although the second component explained more than 5%. The explaining variance of the first component improved with every exclusion of misfitting items. In the fourth step, the person-response validity was close to satisfactory, slightly exceeding the set criteria in the sample. In the fifth step, the ACHC-7 Scale met the criteria for being able to separate between groups using the person separation index; in step 6, it was demonstrated that it may also separate between individuals using the Cronbach’s alpha coefficient. In the seventh step, differential item functioning (DIF) was analysed concerning age, sex, disease severity and time since diagnosis. Significant DIF with regard to sex was demonstrated in items #2 and #7.
In order to ensure that the items demonstrating misfit (items #4, #6 and #9) were not caused by potential DIF, additional DIF analyses were performed to explore this potential misfit bias. None of these items, however, demonstrated DIF in relation to the variables age, sex, disease severity and time since diagnosis. Thus, we concluded that DIF was not a potential cause of the item misfit.
In step eight, targeting was evaluated. The Rasch analysis demonstrated an acceptable fit between the item difficulty in the ACHC-7 Scale and the ability of the subjects (Fig. 2), even though the mean value of item difficulty was somewhat lower than the mean value of the PwMS level of acceptance (Rasch measures, mean = 52.93, standard deviation (SD) = 13.61). A total of 2 PwMS (1.4%) had a maximum score on the ACHC-7 Scale; 1 PwMS (0.7%) had a minimum score.
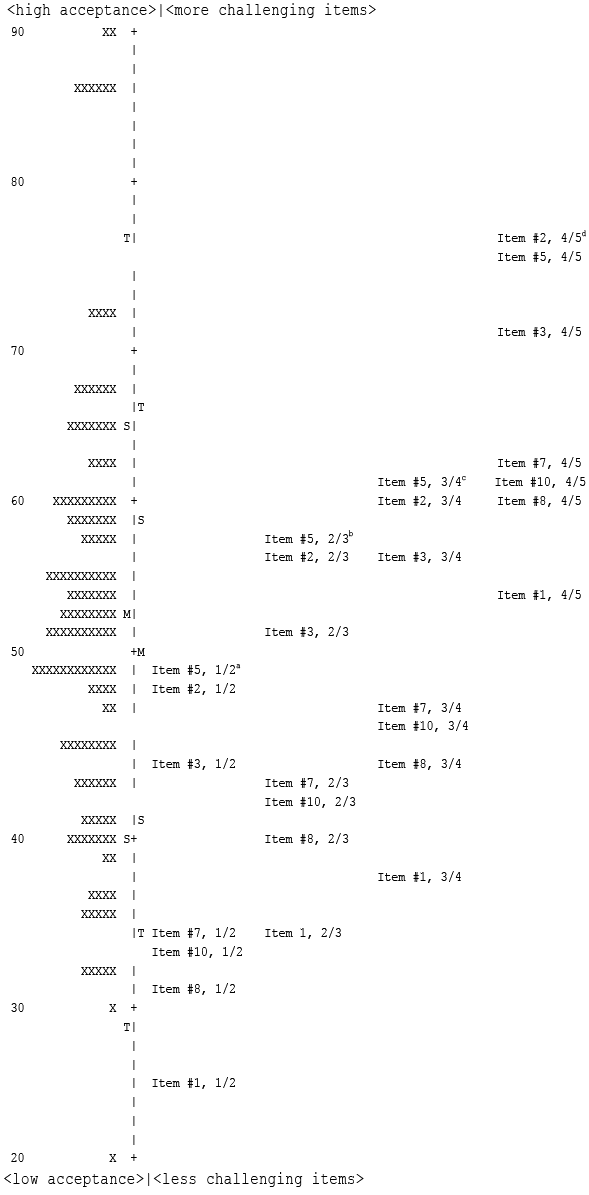
Fig. 2. Person-item map of the 7 items included in the final model of the Acceptance of Chronic Health Conditions Scale (ACHC-7) in a sample of people with multiple sclerosis with Thurstone thresholds. Each item is placed where there is a 50/50 chance of scoring each of the stated categories. a50% chance to respond 1 or 2; b50% chance to respond 2 or 3; c50% chance to respond 3 or 4; d50% chance to respond 4 or 5.
When monitoring the item residual correlations of the ACHC, all values were below 0.5. However, as the mean item residual correlation was only –0.10, a number of so called super-items were created, in all cases where the item residual correlations were higher than the set criterion (larger than –0.30) , This resulted in the creation of 3 super-items, combined out of the original ACHC items #1 to #4, items #6 and #10, and items #7 and #9. The 3 super-items included 1 each of the items that demonstrated misfit in the earlier analysis (items #4, #6, and #9). This new scale of 5 items (original item #5, original item #8, super-item #1 to #4, super-item #7 and #9, and super-item #6 and #10) was then subjected to the same analyses and criteria as the earlier versions. The findings revealed that this scale (now including all the original 10 items) demonstrated overall stronger evidence of internal scale validity, unidimensionality and person response validity, but lower separation and precision in measures (Table V).
DISCUSSION
The aims of this study were to translate and culturally adapt the ACHC Scale into Swedish and to analyse the psychometric properties of the Swedish version of the scale using Rasch analysis. The Swedish version of the 10-item ACHC Scale was considered to be a satisfactory equivalent to the original, but it failed to demonstrate acceptable psychometric properties. Instead, a solution with 7 items (the ACHC-7 Scale) and a solution with 2 items and 3 super-items (the ACHC-5 Scale, with all 10 original items included) demonstrated satisfactory psychometric properties. Use of the ACHC-5 Scale (with all 10 original items) is recommended since this solution presented a more accurate estimate of scale reliability, as it takes into consideration local dependency among items included.
Translation and cultural adaptation
There is a growing body of evidence suggesting that acceptance is an important aspect of adjusting to chronic health conditions (8–10), with potential to facilitate maintained or improved QoL. However, from clinical experience, acceptance can be viewed from different perspectives, as was evident in the translation process in this study. In clinical practice, PwMS who engage in fighting MS, instead of focusing on what makes life meaningful and what can be improved, tend to manifest substantial psychological distress. Since both the expert committee and the PwMS in the pre-testing indicated that acceptance is important to well-being, but that this issue is commonly not addressed by the healthcare services, the ACHC Scale may have potential to improve healthcare services in this aspect, as a means of identifying PwMS who could benefit from support. There may also be reasons to be careful about viewing acceptance as always being a sign of successful adaptation to living with MS. Research concerning adjustment to MS in the early stages of the course of the disease has indicated that it can be of value for the individual with MS to keep a certain distance from the disease in order to maintain QoL (34). In this perspective, use of the ACHC Scale may contribute to increasing the understanding of the acceptance process in MS, highlighting under what circumstances and in what way acceptance may be valuable, thereby guiding which interventions could be most beneficial for the individual and most beneficial from a socio-economic view.
Acceptance can also be seen as reflecting resignation; when that is the case, it is reported to predict distress and relate inversely to better mental and physical health (35). It was more common for the PwMS in the pre-testing to view acceptance more as reflecting resignation, even though they had no problem in viewing acceptance as defined in this study. Awareness of this should be considered when using the ACHC Scale. It may not be beneficial to title a questionnaire as being about acceptance without defining the intended meaning of acceptance.
In the translation process, the comprehensive methodology of translation and cultural adaptation strengthens the quality of the Swedish version of the ACHC Scale. Even though all the translators and the expert committee were experienced and competent in Swedish, English and in their respective professions, a professional translator may have improved the composition of the expert committee. It has been proposed that knowledge about the translation process and extensive validation is more important than the specific method (36). The co-workers in the study found that the most important factors for achieving a high-quality translation included: having knowledge of key aspects of translation and cultural adaptation, in particular the meaning of idiomatic equivalence in comparison with a correct translation word by word; interest in the particular meanings of words in different contexts; and having input from the PwMS in the pre-testing.
Rating scale functioning and targeting
PwMS may gradually come to accept living with MS and thereby successfully adapt to the disease (37). Thus, newly diagnosed PwMS may demonstrate a lower degree of acceptance. In the Rasch analysis sample there was an abundance of responses indicating a higher degree of acceptance; this could be expected, since all these participants were diagnosed at least 10 years previously. A sample that also included newly diagnosed PwMS might have given different results. Although no clear ceiling effect was seen in this sample, more difficult items could still be considered, but the value of this can be questioned, since that probably would not improve clinical use of the scale. In a clinical view, it would be more valuable to identify those with a low degree of acceptance than those with extraordinary acceptance ability.
The generic rating scale used in this analysis met the criteria set. When the category function is inadequate, collapsing scale steps is an option for achieving a better fit (22). Collapsing of categories 2 and 3, the 2 categories least responded to, was considered but not performed because of the uncertainty of the meaning of category 3. If it is not perceived as an alternative in the middle of “agree” and “disagree”, as indicated in the pre-testing, the categories should probably not be collapsed. One option would be to rename category 3 so that it is clearly an in-the-middle alternative, and thereby continue the evaluation of the scale. Future studies with larger samples could also allow for more in-depth analysis of the rating scale functioning in each item, before deciding on collapsing scale steps.
Item goodness-of-fit
All 3 items that did not originally fit the Rasch model can be viewed as having a dual meaning. In item #4 it was possible to agree with one part of the statement and not with the other, which may have contributed to item misfit. To resolve this, the item can be excluded or re-phrased. We chose to exclude it, based on the finding that several aspects of the scale’s psychometric properties improved with the item excluded. Items #6 and #9 could also be seen as having a dual meaning in how “just a part of” was understood. In item #6 one can understand the item as “MS is something that could happen to anyone”, as well as “something unfair because it actually does not happen to everyone and is not part of anyone’s life”. In item #9 it is a matter of if you have integrated MS as part of your life without letting it define you, or identifying with MS as being you. How you understand these items determines how you respond. Exclusion of these items was therefore the better solution. In the present study, using the Rasch model, it is clearly shown that items should have a single meaning, otherwise inconsistency in responses might appear and misfit be demonstrated.
Four items in the ACHC scale were positively worded and therefore reversely coded compared with the other items. It can be noted that all 3 items that demonstrated misfit were reversed items. It has previously been suggested that the psychometric properties (reliability and validity) might be diminished when semantically opposite items are included in a scale (38).
It is also noteworthy that the items demonstrating misfit could remain in the scale when considering the item residual correlation and, thus, by combining items into super-items. This scale (the ACHC-5 Scale) also demonstrated better psychometric qualities than the ACHC-7 Scale, but lacked precision and ability to separate the sample into distinct groups.
Unidimensionality and ability to separate between groups
The 10-item ACHC Scale cannot be considered a unidimensional scale based on the present study. In the ACHC-7 Scale, unidimensionality for the first component was satisfactory; however, the second component explained >5% of variance, implying that further studies on unidimensionality are required, since this questions the use of the ACHC-7 Scale as a summed version. With regard to DIF, 2 items in the ACHC-7 Scale implied differences with regard to sex. The ACHC-7 Scale demonstrated acceptable psychometric properties, although not all of the criteria were fulfilled. The ACHC-5 Scale with 2 items and 3 super-items also did not meet all criteria, but resulted in the greatest variance explained by the measures, with minimal impact of a secondary component, implying that this solution should presently be recommended for use. The multidimensionality detected in the scales not including super-items may therefore simply be a result of the local dependency in the data, as confirmed by the analysis of the scale including super-items. The difficulty of constructing rating scales with satisfactory psychometric properties in all aspects should always be kept in mind when interpreting results, the ACHC Scale included. Future studies with larger data-sets is therefore needed to explore and reveal whether there is an optimal even shorter version of the ACHC Scale that can be used in clinical settings with remaining strong psychometric properties across various aspects of validity, reliability, and sensitivity to change.
Further evaluation of other aspects of validity and reliability than the scope of this study is therefore warranted. Previously collected data on the sample in this study would allow analysis of test-re-test reliability, sensitivity to change, and comparison with other variables. Analysis of data from the ACHC Scale, including newly diagnosed PwMS, would also be valuable.
Conclusion
Satisfactory equivalence between the original and the Swedish version of the ACHC Scale was considered to have been achieved. Rasch analysis of the Swedish version demonstrated acceptable psychometric properties in a version with 7 items (the ACHC-7 Scale) and in a version with 2 items and 3 super-items (the ACHC-5 Scale, with all 10 original items included). Use of the ACHC-5 Scale with super-items is recommended, since it adjusts for local dependency among items.
REFERENCES

