Irma Mehmedagic, MD1, Stefan Santén, MD, PhD1,4, Sophie Jörgensen, MD2,5 and
Stefan Acosta, MD, PhD1,3
From the 1Institution of Clinical Sciences, Malmö, 2Department of Health Sciences, 3Vascular Center, Lund University, 4Department of Surgery, and 5Department of Neurology and Rehabilitation Medicine, Skåne University Hospital,
Lund, Sweden
OBJECTIVE: Advanced endovascular aortic repair can be used to treat patients with extensive and complex aortic disease who are at risk of spinal cord ischaemia. The aim of this study was to compare whether life satisfaction differs between patients with and without spinal cord ischaemia at mid-term follow-up.
DESIGN: Nested case-control study.
Patients: Among patients undergoing advanced endovascular aortic repair between 2009 and 2012, 18 patients with spinal cord ischaemia and 33 without were interviewed at home.
METHODS: The Life Satisfaction Questionnaire (LiSat-11) and the Satisfaction With Life Scale (SWLS) were used.
RESULTS: LiSat-11 found that patients with spinal cord ischaemia were more dissatisfied with their activities of daily living than were patients without spinal cord ischaemia (p=0.012). Both groups had similar, very low, scores in the sexual life domain; median 2.0 (interquartile range (IQR) 1.5–3.0) and 3.0 (IQR 2.0–4.0), respectively. There was no difference in SWLS between the groups.
CONCLUSION: This study cohort of patients who underwent advanced endovascular aortic repair was rather homogenous in their rating of life satisfaction and there was little difference between mid-term survivors who had spinal cord ischaemia and those who did not.
Key words: endovascular therapy; spinal cord ischaemia; spinal cord injury; quality of life; life satisfaction.
J Rehabil Med 2016; 00: 00–00
Correspondence address: Stefan Acosta, Vascular Center, Malmö, Skåne University Hospital, SE-205 02 Malmö, Sweden. E-mail: Stefan.acosta@med.lu.se
Accepted Aug 29, 2016; Epub ahead of print Oct 13, 2016
INTRODUCTION
Patients with extensive aortic disease due to aneurysm or dissection, live with the risk of aortic rupture if the disease is left untreated. The risk of rupture is associated mainly with the maximal aneurysm diameter and/or expansion rate of the aneurysm (1). If treatment is considered it should be weighed carefully against the risk of perioperative morbidity, mortality and life-expectancy, in these high-risk patients who are often in cardio-pulmonary poor condition. Neurological complications, such as spinal cord ischaemia (SCI) (2) and stroke (3), following operative therapy may be devastating for the patient, and these complications are rather common.
Analysis of patient-reported outcome measures following advanced aortic repair is important to inform future counselling of patients in the planning stages of this procedure. A recent study assessed life satisfaction in patients with SCI after advanced endovascular therapy for extensive aortic disease at mid-term follow-up (4). The main criticism of this study was that these elderly patients with several comorbidities who had SCI after advanced endovascular therapy were compared with a large sample of healthy Swedes in the age range 18–64 years (5). A better reference sample of cohorts, adjusted for age and comorbidity, was used by Crawford et al. (6) when assessing quality of life at long-term follow-up.
In an attempt to evaluate life satisfaction in patients with SCI more accurately in relation to a more appropriate control group in terms of age and co-morbid conditions, a nested case control study was designed. The aim of this study, in patients with and without SCI, was to study life satisfaction at mid-term follow-up after advanced endovascular therapy for extensive aortic disease.
MATERIAL AND METHODS
Patients
A total of 83 patients at high risk for SCI underwent advanced endovascular therapy and cerebro-spinal fluid drain insertion for complex aortic disease at the Vascular Center, Malmö, Skåne University, Sweden, between 2009 and 2012. As reported previously, 29 patients had SCI peri-operatively (4). At follow-up, 8 patients were deceased; 3 patients were excluded due to no symptoms of SCI; and 18 patients with symptoms of SCI underwent an at-home interview (Fig. 1).
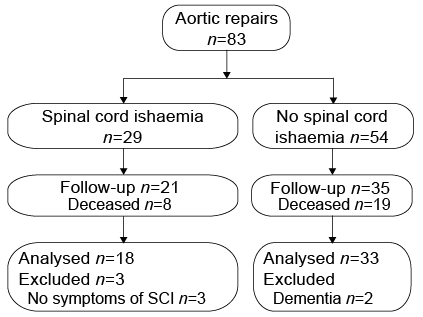
Fig. 1. A total of 83 patients undergoing advanced endovascular aortic repair, were categorized into 2 groups; those complicated with or without spinal cord ischaemia.
As reported earlier, 44 patients with no perioperative SCI were identified (4). At follow-up, 19 were deceased, and 35 patients with no symptoms of SCI remained. Thirty-three patients were eligible to participate in the study; 2 were excluded due to dementia (n = 2) (Fig. 1). A final total of 18 patients with symptoms of SCI and 33 with no symptoms of SCI underwent life satisfaction measurements. Telephone contact was established and all patients were offered a home visit for a 1 h interview. The patients were interviewed according to a study-specific questionnaire regarding comorbidities, everyday life aspects and life satisfaction. Three patients preferred to complete the questionnaire at home, rather than being interviewed. The life satisfaction questionnaires used were the Life Satisfaction Questionnaire (LiSat-11) and the Satisfaction With Life Scale (SWLS). Interviews were carried out throughout summer 2014 until summer 2015. None of the patients lived in a nursing home.
Median time from operation to interview was 45 months (range 14–79 months); 26 months (range 14–56 months) in those with SCI, and 49 months (range 26–79 months) in those without SCI (p = 0.001). Information on survival was retrieved from the Swedish Population registry on 10 August 2015. Median time of follow-up on survival was 58 months (range 22–78 months); 49 months (range 22–74 months) in those with SCI and 62 months (range 38–78 months) in those without SCI (p = 0.086). Mid-term follow-up refers to the evaluation of outcome in patients 2–5 years after complex endovascular aneurysm repair procedures (6).
Life satisfaction
Life satisfaction was assessed with 2 self-report questionnaires, the LiSat-11 and the SWLS. The LiSat-11 (5) contains 11 items rated on a 6-point Likert scale (1 = very dissatisfied to 6 = very satisfied). It includes one item assessing global life satisfaction (“Life as a whole”) and 10 domain-specific items. The SWLS (7), a global assessment tool of life satisfaction, comprises 5 items rated on a 7-point Likert scale (1 = strongly disagree to 7 = strongly agree). The scores are summed to a total score between 5 and 35, where greater scores represent greater life satisfaction. The scores were presented as median (interquartile range; IQR).
Statistical analysis
SPSS software (version 22.0; SPSS Inc, Chicago, IL, USA) was used for data managing and statistical analysis. Continuous variables were expressed as median, IQR and range. The χ2 test and Fisher’s exact test were used when appropriate. The Mann-Whitney U test was used for in-group comparisons of asymmetric continuous data. The Kendall tau B-test was used for ordinal scale data. The log-rank test was used for Kaplan–Meier survival analysis. p < 0.05 was considered significant.
RESULTS
Survival
Kaplan–Meier survival analysis showed no difference in survival of the 29 patients with SCI compared with the 54 patients without SCI (p = 0.88) (Fig. 2) in the original study cohort.
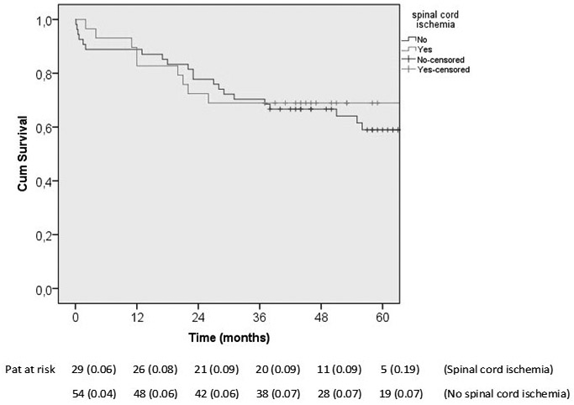
Fig. 2. Long-term comparative survival curves of patients undergoing advanced endovascular aortic repair, complicated vs not complicated with spinal cord ischaemia (SCI). Numbers below the time axis denote patients at risk in the 2 groups at respective time-points. Standard error of cumulative proportion of patient survival at end of interval is shown in parentheses. The tick marks indicate censored data. Complete crude 3-year follow-up indicating no censored data prior to the 36-month time-point.
Patient characteristics
In the SCI group, 2 patients had complete (American Spinal Injury Association Impairment Scale (AIS) A) and 16 incomplete SCI (1 AIS B and 15 AIS D) at hospital discharge after the operation.
Patients with SCI were older (p = 0.018), had a higher proportion of ischaemic heart disease (p = 0.048), and were prescribed acetylsalicylic acid (aspirin) (p = 0.040) in a higher proportion than those without SCI (Table I). Among those who had SCI, aortic aneurysm (p = 0.024) was more often found to be the indication for therapy, and aortic dissection (p = 0.022) was less often found to be the indication, compared with those without SCI. There was also a trend towards a higher proportion of thoraco-abdominal aortic aneurysm (TAAA) (p = 0.063) in patients with SCI (Table II). Patients with TAAA, type 1 and 2, had a higher proportion of occurrence of SCI, compared with those with TAAA, type 3 and 4 (p = 0.007) (Table II).
|
Table I. Comparison of preoperative characteristics in patients with and without spinal cord ischaemia (SCI) after advanced endovascular therapy for aortic disease |
|||
|
SCI (n = 18) |
No SCI (n = 33 |
p-value |
|
|
Age, years, median (range) |
70 (54–76) |
66 (44–82) |
0.018 |
|
Sex (male/female), n (%) |
15 (83)/3 (17) |
21 (64)/12 (36) |
0.14 |
|
Living in couple, n (%) |
16 (89) |
24 (73) |
0.32 |
|
Comorbidity, n (%) |
|||
|
Hypertension |
18 (100) |
29 (88) |
0.16 |
|
Smoking |
16 (89) |
29 (88) |
0.65 |
|
Diabetes mellitus |
3 (17) |
4 (12) |
0.48 |
|
Ischaemic heart disease |
8 (44) |
6 (18) |
0.048 |
|
Stroke or transient ischaemic attack |
2 (11) |
2 (6) |
0.44 |
|
COPD (spirometry verified) |
4/9 (44) |
5/17 (29) |
0.44 |
|
Renal function impairment |
13 (72) |
19 (58) |
0.30 |
|
Cancer diagnosis |
4 (22) |
5 (15) |
0.39 |
|
Medication, n (%) |
|||
|
Lipid-lowering agent |
14 (78) |
19 (58) |
0.15 |
|
Acetylsalicylic acid |
15 (83) |
18 (55) |
0.040 |
|
COPD: chronic obstructive pulmonary disease. |
|||
|
Table II. Comparison of characteristics in aortic disease in patients with and without spinal cord ischaemia (SCI) after advanced endovascular therapy for aortic disease |
|||
|
SCI n (%) |
No SCI (n = 33) n (%) |
p-value |
|
|
Indication |
|||
|
Aortic aneurysm |
17 (94) |
22 (67) |
0.024 |
|
Pseudo-aneurysm |
1 (6) |
3 (9) |
0.56 |
|
Aortic dissection |
0 |
8 (24) |
0.022 |
|
Operation (acute) |
7 (39) |
17 (52) |
0.39 |
|
Thoraco-abdominal aortic aneurysm |
12 (67) |
13 (39) |
0.063 |
|
Thoraco-abdominal aortic aneurysm, |
|||
|
Type 1 |
3/12 (25) |
1/13 (8) |
|
|
Type 2 |
6/12 (50) |
3/13 (23) |
|
|
Type 3 |
2/12 (17) |
4/13 (31) |
|
|
Type 4 |
1/12 (8) |
5/13 (38) |
0.007 |
|
aCrawford classification of thoraco-abdominal aortic aneurysms. Type 1, distal to the left subclavian artery to above the renal arteries. Type 2, distal to the subclavian artery to below the renal arteries. Type 3, from the sixth intercostal space to below the renal arteries. Type 4, from the 13th intercostal space to the iliac bifurcation (entire abdominal aorta). |
|||
Life satisfaction in patients with SCI compared with patients without SCI
According to the LiSat-11 questionnaire, patients without SCI were more satisfied with their activities of daily living (ADL; p = 0.012) compared with patients with SCI. Both groups had relatively high scores in the domains family life and partner relationship. Both groups had low scores in the domain sexual life (Table III).
|
Table III. Comparison of self-reported levels of life satisfaction (LiSat-11) in patients with and without spinal cord ischaemia (SCI) after advanced endovascular therapy for aortic disease |
|||
|
SCI (n = 18) Median (IQR) |
No SCI (n = 32) Median (IQR) |
p-value |
|
|
Life as a whole |
4.0 (3.0–5.0) |
5.0 (4.0–5.0) |
0.12 |
|
Vocation |
4.5 (3.5–5.0) |
5.0 (3.0–5.0) |
0.83 |
|
Economy |
5.0 (4.0–5.2) |
5.0 (4.0–5.0) |
0.58 |
|
Leisure |
4.0 (3.0–5.0) |
4.0 (4.0–5.0) |
0.67 |
|
Contact with friends |
5.0 (4.0–6.0) |
5.0 (4.2–5.0) |
0.80 |
|
Sexual life (n = 17, n = 30) |
2.0 (1.5–3.0) |
3.0 (2.0–4.0) |
0.12 |
|
Activities of daily living |
4.0 (2.0–5.0) |
5.0 (4.0–6.0) |
0.012 |
|
Family life (n = 17, n = 29) |
5.0 (5.0–6.0) |
5.5 (5.0–6.0) |
0.86 |
|
Partner relationship |
5.5 (5.0–6.0) |
6.0 (5.0–6.0) |
0.64 |
|
Somatic health |
4.0 (2.8–4.2) |
4.0 (3.0–5.0) |
0.68 |
|
Psychological health |
5.0 (4.0–6.0) |
4.0 (4.0–5.0) |
0.58 |
|
IQR: interquartile range. |
|||
No difference in the 5 SWLS questions or the total score was found between the 2 groups (Table IV).
|
Table IV. Satisfaction With Life Scale (SWLS) for patients with and without spinal cord ischaemia (SCI) after advanced endovascular therapy for aortic disease |
|||
|
SCI (n = 18) Median (IQR) |
No SCI (n = 33) Median (IQR) |
p-value |
|
|
SWLS 1: In most ways my life is close to my ideal |
4.5 (1.8–6.0) |
5.0 (4.0–6.0) |
0.61 |
|
SWLS 2: The conditions of my life are excellent |
5.0 (2.0–6.0) |
5.0 (4.0–6.0) |
0.21 |
|
SWLS 3: I am satisfied with my life |
5.0 (2.8–6.2) |
6.0 (4.5–6.0) |
0.33 |
|
SWLS 4: So far I have gotten the important things I want in life |
5.0 (4.8–6.0) |
5.0 (5.0–6.0) |
0.85 |
|
SWLS 5: If I could live my life over, I would change almost nothing |
6.0 (4.0–6.2) |
5.0 (4.0–6.0) |
0.60 |
|
SWLS total |
24.5 (15.0–29.2) |
26.0 (22.5–29.0) |
0.59 |
|
IQR: interquartile range. |
|||
DISCUSSION
The present nested case-control study shows the importance of selecting an appropriately co-morbidity matched control group. The main findings were that patients both with and without SCI were satisfied with many aspects of their life, but rated low satisfaction with their sexual life. It is possible that disease severity has less effect on life satisfaction than illness perception and self-efficacy beliefs (8). However, dissatisfaction was seen in both groups regarding sexual life and somatic health, which might reflect that many of these patients were in poor general health.
The small differences in life satisfaction between patients with SCI and those without at mid-term follow-up should, however, be viewed with the knowledge that the interviewed patients with SCI had less severe neurological deficits than those with SCI who died prior to the interview (4). The natural selection of apparently fitter patients at mid- or long-term follow-up (9, 10) should be taken into account when interpreting data on long-term functional and quality of life outcomes (6, 11). Although comparative analysis between the 2 groups should be interpreted with caution, mid-term survival analysis of the entire study cohort of 83 patients showed, somewhat surprisingly, no differences in survival at any time-point between the 29 patients with SCI and the 54 patients without SCI. Hence, this further strengthens that the actual control group was comparable with the SCI group in terms of co-morbidity burden.
In contrast to the survival results in the present study, 2 large retrospective studies have found that SCI after aortic repair was associated with poorer long-term survival compared with those without SCI (9, 10). Nevertheless, when excluding patients with the most severe neurological deficits and without functional improvement, the remaining SCI-patients seem to have similar life-expectancy as those without SCI (9, 10). Patients with SCI, in a uni-variate analysis, were older and had a higher prevalence of hypertension, smoking, dyslipidaemia, renal insufficiency, chronic obstructive pulmonary disease, cerebrovascular occlusive disease, peripheral vascular disease (9) and coronary artery disease (10) compared with those without SCI. The present study showed some similarities with these studies (9, 10) in that the patients with SCI were older and had a higher prevalence of coronary artery disease, but, on the other hand, were better medicated with acetylsalicylic acid, compared with those without SCI.
Since spinal cord injuries result in a spectrum of deficits, such as paralysis, sensory impairments, neurogenic bowel and bladder dysfunction, sexual dysfunction and pain, it is important not to report only on whether ambulatory capacity is present. Investigators should at least determine the presence of urinary bladder dysfunction (2) and use established grading scales, such as the AIS, to assess neurological deficit, in order to make results interpretable and generalizable to other settings (4). Initial neurological assessment based on the AIS has been reported to be the best predictor of prognosis (12), but retrospective studies from vascular units are often hampered by the absence of consequent AIS grading in in-hospital patients (9, 10, 13). Furthermore, a thorough neurological examination and assessment of other SCI-related complications is of great importance in order to plan appropriate rehabilitation interventions. It is also essential to have a multi-disciplinary research team composed of vascular surgeons, neurologists and/or physicians specialized in rehabilitation medicine to be able to deliver high-quality outcome data after aortic repair complicated by SCI.
The limitations of the present study are attributed to missing life satisfaction data in patients who died prior to assessment. In addition, the interviews were performed, on average, at least one year later for the majority of patients in the control group. As the control group, on average, were a few years younger, the age difference between the case and control group at the time of interview was reduced. It is likely that the different time interval between operation and interview in the 2 groups has introduced a bias, but it is very difficult to determine to what extent. Nevertheless, the nested case-control study assured a high-quality control group (14). In view of the previous retrospective comparative study (4), a reference sample from the general population or from healthy controls in studies such as the present one should be avoided if possible. It will be difficult to perform prospective comparative studies of life satisfaction in this particular patient cohort.
It might be considered counterintuitive that an otherwise catastrophic neurological injury seems to have only marginal consequences for life satisfaction. In the present study, only one domain, activities of daily living, was rated significantly lower among patients with SCI compared with those without SCI. The absence of lower life satisfaction scores among patients with SCI might be attributable to statistical type 2 error due to the small number of patients within each group. Another plausible explanation is that SCI patients with the most severe neurological injury, and probably the lowest life satisfaction scores, died before the interview. However, other factors, such as the presence of cardiovascular and pulmonary disease, might, to a large extent, influence life satisfaction and reduce the differences between the 2 groups. It was noteworthy that almost all patients in this study (89% of the SCI patients and 73% of the non-SCI patients) were living in a couple. According to the specific LiSat scores in the present study, this contributed to a large positive effect on their global life satisfaction.
In conclusion, this study showed small differences in life satisfaction between mid-term survivors after endovascular repair of extensive aortic disease complicated by SCI in comparison with an evenly matched control group without SCI. It should, however, be taken into consideration that the interviewed survivors with SCI had less severe neurological deficits than those who died prior to assessment.
REFERENCES

