
From the Department of Neurosurgery, Sir Charles Gairdner Hospital, Perth, WA, Australia
Given the continued use of decompressive craniectomy in the management of neurological emergencies recognition of complications is important in order for patients to gain maximal benefit during rehabilitation. One complication that has received relatively little attention is the neurological dysfunction that can occur due to distortion of the brain under the scalp as cerebral oedema subsides. The neurological deterioration that may occur can take many forms, probably due to a multifactorial pathophysiology. Recognition of this condition is important in order to avoid delays in the rehabilitation process. This review discusses the historical background, possible pathophysiological mechanisms, clinical incidence and implications for physiotherapists involved in rehabilitation.
Key words: decompressive craniectomy; rehabilitation; complications.
Accepted Jan 17, 2017; Epub ahead of print Feb 24, 2017
J Rehabil Med 2017; 49: 204–207
Correspondence address: Stephen Honeybul, Department of Neurosurgery, Sir Charles Gairdner Hospital, WA, Australia, E-mail: stephen.honeybul@health.wa.gov.au
There continues to be a considerable amount of interest in the use of decompressive craniectomy in the management of neurological emergencies (1). The procedure itself is technically straightforward and involves temporarily removing a large segment of the skull either unilaterally or bifrontally, in order to allow more room into which the injured or ischaemic brain can expand. The use of decompressive craniectomy has been described for a number of pathological conditions; however, it is most commonly used in the context of severe traumatic brain injury or ischaemic stroke. Once the cerebral swelling has subsided a cranioplasty procedure is performed to replace the bone flap and restore the cranial contour. This is usually carried out approximately 3–4 months after the initial decompressive procedure. Throughout this period many patients face a long and often protracted recovery, often complicated by issues such as infection, electrolyte disturbances, seizures, and cerebrospinal fluid (CSF) hydrodynamic disturbances, such as hydrocephalus, all of which can have a significant effect on the rehabilitation process (2).
One complication that has received relatively little attention is the neurological dysfunction that can occur due to the absence of the bone flap and the subsequent distortion of the brain that occurs under the scalp as cerebral swelling subsides. Various terms have been used to describe the wide variety of different neurological manifestations with which this dysfunction can present. Until recently, these conditions were thought to be relatively uncommon; however, it is becoming apparent that a significant number of patients are particularly susceptible to this phenomenon and may present with subtle functional deficits that may not be appreciated on routine clinical evaluation.
Physiotherapists are often heavily involved in the day to day rehabilitation of these patients and, as such, are well placed to appreciate any such changes in clinical function and perhaps raise the possibility that consideration should be given to diagnose this phenomenon.
The aims of this narrative review are to discuss the historical perspectives, proposed pathophysiology, and clinical incidence of neurological dysfunction secondary to a large skull defect, as well as the practical implications for physiotherapists involved in rehabilitation medicine.
There have been numerous terms applied to describe neurological dysfunction secondary to a large skull defect, the first of which was “syndrome of the trephined”, coined by Grant & Norcross in 1939 (3). Their initial description was of subjective complaints from some individuals with a large skull defect, which were documented as: dizziness, undue fatigability, vague discomfort at the site of the defect, a feeling of apprehension and insecurity, mental depression, and intolerance to vibration. Although they have been credited with the initial term and description, they were by no means the first to notice these clinical symptoms. Indeed, they made no such claim, and their original article cited 137 articles that dealt with reconstruction of cranial defects, many of which described similar clinical changes (3). Thereafter, several terms have been suggested that describe what is, in effect, a different manifestation of the same condition. Grantham used the term “post-traumatic syndrome” to describe similar subjective symptoms to that of “syndrome of the trephined (4). Yamaura & Makino used the term “syndrome of the sinking scalp flap” to describe the objective focal neurological deficits that can occur in patients with a hemicraniectomy defect (5). “Motor trephined syndrome” is another term used to describe objective motor deficits (6). More recently the term “neurological susceptibility to a skull defect” (NSSD) has been suggested, which essentially covers any neurological sign or symptom that is attributable to the lack of cranial coverage (7).
In the classical descriptions patients who exhibit this type of signs and symptoms do so after an initial period of improvement following decompressive surgery. Thereafter, as the scalp flap sinks, there is a period of clinical deterioration and the diagnosis is confirmed when the symptoms resolve or improve following replacement of the bone flap (8).
Unfortunately, despite the numerous terms available, allotting a patient a specific diagnosis can be problematic because patients can present with a wide range of clinical signs and symptoms. The most commonly reported presenting symptom has been that of a motor deficit; however, other reported symptoms have included cognitive deficits, language deficits, altered levels of consciousness, headache, psychosomatic issues and cranial nerve deficits. The mean time between craniectomy and onset of symptoms is approximately 5 months, although a considerable range has been reported (9). In addition, whilst some patients present with classical features, others plateau in terms of recovery in rehabilitation, then clinically improve following cranioplasty (10).
One of the difficulties with use of the current nomenclature is the considerable overlap between the diagnostic categories. For example, a patient may develop a focal deficit, such as a hemiparesis, and be diagnosed with “syndrome of the sinking scalp flap” or “motor trephined syndrome”. However, on closer questioning they may be found to have postural headaches and other subjective symptoms, leading to a diagnosis of “syndrome of the trephined”.
Thus, NSSD may be useful as it is a blanket term to describe any kind of neurological dysfunction of what is, in fact, a multifactorial pathophysiology (7).
The underlying pathophysiology responsible for the various neurological manifestations is unknown; however, a number of theories have been proposed, including: direct effects of atmospheric air on the brain, alterations in CSF hydrodynamics, and changes in cerebral blood flow.
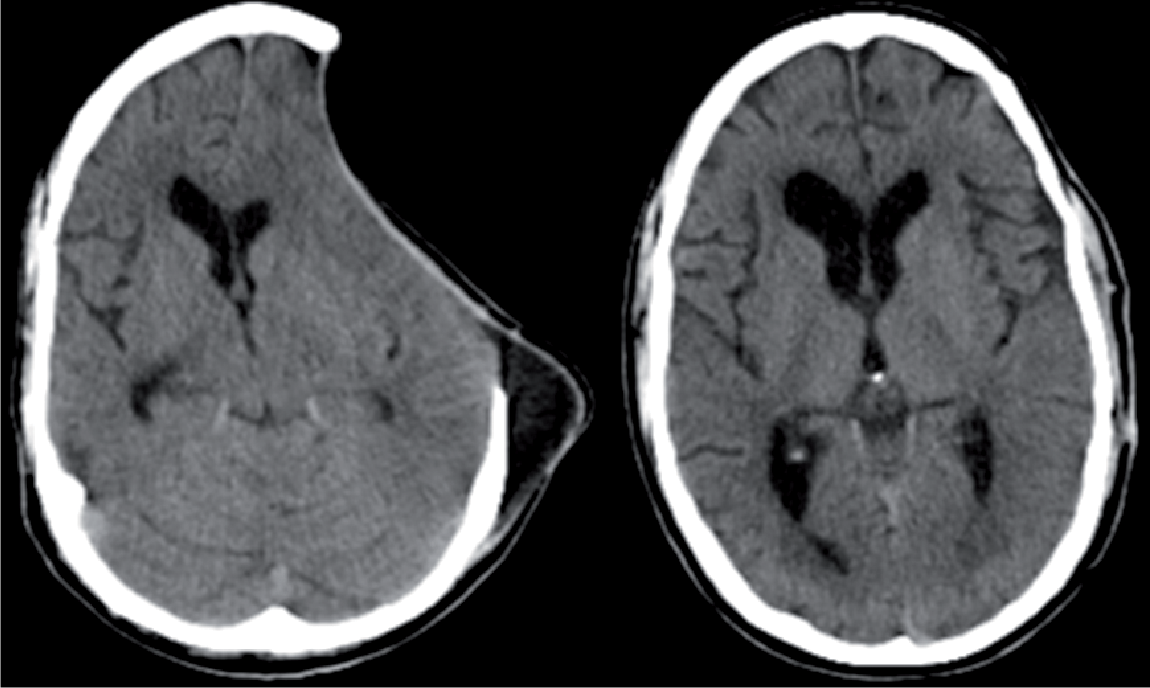
In normal physiological circumstances the brain floats in supportive CSF and fills the confines of the cranial cavity. Once the “closed box” or skull has been opened the principles of the Monroe-Kellie doctrine no longer apply and the brain will be exposed to atmospheric pressure, causing distortion not only of the cerebral cortex, but also of other intracranial structures, such as the dura and cranial nerves (Fig. 1). This may be the cause of posture-related signs and symptoms such as headache, altered sensorium, cranial nerve palsies and mydriasis (11, 12).
Fig. 1. Considerable sinking of the scalp and distortion of the underlying intracranial contents following a hemicraniectomy for severe traumatic brain injury (left). The cranial contour is restored following cranioplasty (right).
In the upright position the intracranial pressure (ICP) will usually be negative; however, in patients with a large skull defect the ICP will equalize with the atmospheric pressure, leading to a higher than normal pressure. This has been demonstrated in studies that used CSF infusion tests, and it was possible to demonstrate that these hydrodynamic abnormalities were reversed once the bone flap was replaced (8).
A number of studies have demonstrated the alterations in cerebral blood flow that can occur under a large skull defect and the subsequent improvement in blood flow that can occur following cranioplasty (13, 14). The pathophysiology underlying this vascular response is unknown, but may be due in part to the transmission of atmospheric pressure on to the cerebral vasculature combined with normalization of CSF compliance and cerebrovascular autoregulatory function (15).
Overall, it would seem most likely that a large skull defect can have numerous effects on the cerebrovascular physiology and CSF hydrodynamics, and that there will be no single pathophysiological mechanism to account for the wide variety of clinical manifestations reported.
The true incidence of this clinical condition remains unknown. Earlier reports regarding neurological dysfunction due to a large skull defect have described these manifestations as either rare or uncommon; however, most publications were either case reports or small retrospective cohort studies. Whilst some of them did describe impressive neurological recoveries, there was often no baseline denominator recording the number of patients for whom the cranioplasty had no clinical impact.
More recently a prospective cohort study found an objective improvement in neurological function in 4 (16%) out of 25 patients who were assessed a few days before and after cranioplasty; however, more work on larger case series will be required to determine not only the true incidence, but also what factors predispose patients to this condition (16). These issues may be important when considering both the impact that this can have on rehabilitation and the timing of the cranioplasty procedure.
Given the continued interest in the use of decompressive craniectomy for a variety of neurological emergencies, there may need to be a greater awareness of some of the practical issues that need to be considered regarding the day to day management of these patients.
Patients who have had a decompressive craniectomy following trauma require careful consideration in their falls risk assessment. Although several publications have observed the theoretical risk of injury to the unprotected cranium and described methods by which this may be prevented (17, 18), there has only been 1 report of a death following a fall onto the unprotected cranium (19). It may be that this is a rare event or it may be under-reported; however, a detailed falls risk assessment is recommended before patients are allowed to be mobilized unaided and unsupervised. The type of assessment will vary between institutions; however, the aforementioned case report highlighted the limitations of using the Glasgow Coma Score (GCS) when making such an assessment. Patients with a low GCS will be a low falls risk as they will be unable to mobilize. As they clinically improve their falls risk will increase, especially when they are awake and alert but confused (GSC 14 – E4, M6, V4). A more practical evaluation would entail at neurocognitive assessment to determine a patient’s level of insight into their individual falls risk and need or otherwise for supervision.
Once successfully mobilized ongoing care is required to avoid injury to the unprotected brain. A helmet that is well fitted and comfortable is recommended; however, as patients continue to recover this can be removed when sitting quietly in a safe environment. It must be emphasized that the most important consideration is a patient’s insight into the possibility of cranial injury and the need to apply the helmets themselves if they mobilize unsupervised. The use of a helmet would be deemed mandatory in the context of definitive rehabilitation exercises. There would be no contraindication to the use of light weights and aerobic exercise on a stationary bicycle; however, the use of heavy weights and excessive jarring exercise should probably be avoided.
Once the brain swelling starts to subside the contour of the scalp will slowly subside and eventually it will become concave. There will be some diurnal variation, in that the scalp will appear “full” first thing in the morning and will slowly become more concave throughout the day as the effect of gravity redistributes CSF throughout the subarachnoid space. In certain circumstances CSF hydrodynamics can be disturbed, such that patients may develop either subdural hygromas or hydrocephalus. When this occurs the scalp flap may appear swollen and tense and there may be accompanying nausea, vomiting and progressive drowsiness. Early recognition of this complication is important in order to expedite either drainage of the hygroma or insertion of a ventriculo-peritoneal shunt.
The optimal timing of cranioplasty has not been clearly established. For many years it was suggested that the procedure should be delayed in order to reduce the risk of infection; however, recent studies have suggested that early cranioplasty can be performed safely (7). In view of these findings it would seem logical to replace the bone flap as soon as clinically possible, given that rehabilitation facilities are often a scarce and valuable resource. Every effort must be made to ensure that these resources are deployed appropriately in order to provide as many patients as possible with maximal benefit. Indeed, given the impact that a large skull defect can have on neurological recovery, it has been suggested that intensive neurocognitive rehabilitation should not be undertaken until a cranioplasty has been performed (20). Whilst this may seem a reasonable position to adopt, it would mean that those patients not affected by the skull defect would miss out on the potential benefit of early rehabilitation. A more realistic approach would be to highlight the need to recognize the condition in susceptible individuals in whom earlier reconstructive cranioplasty may need to be considered.
Patients who have had a decompressive craniectomy face a particularly challenging recovery and all efforts should be made to maximize the potential for neurological recovery. It is becoming increasingly apparent that certain individuals are particularly susceptible to having a large skull defect and physiotherapists involved in the day to day rehabilitation of these patients are well placed to recognize these individuals and perhaps suggest referral for early cranioplasty so that there is minimal disruption to the rehabilitation process.


 Click to show fullsize
Click to show fullsize