
From the 1Department of Rehabilitation Medicine, University Hospital of Linköping, Linköping, Sweden, 2Medtronic EMEA Regional Clinical Center, Milano, Italy and 3Medtronic International Trading Sàrl, Tolochenaz, Switzerland
Oral baclofen has long been a mainstay in the management of spasticity. This review looks at the clinical evidence for the efficacy and safety of oral baclofen in patients with spasticity of any origin or severity, to determine whether there is a rationale for the use of intrathecal baclofen. Results suggest that oral baclofen may be effective in many patients with spasticity, regardless of the underlying disease or severity, and that it is at least comparable with other antispasmodic agents. However, adverse effects, such as muscle weakness, nausea, somnolence and paraesthesia, are common with oral baclofen, affecting between 25% and 75% of patients, and limiting its usefulness. Intrathecal baclofen may be an effective alternative as the drug is delivered directly into the cerebrospinal fluid, thus bypassing the blood-brain barrier and thereby optimizing the efficacy of baclofen while minimizing drug-related side-effects. Intrathecal baclofen is a viable option in patients who experience intolerable side-effects or who fail to respond to the maximum recommended dose of oral baclofen.
Key words: intrathecal baclofen; oral baclofen; spasticity.
Accepted Jan 25, 2017; Epub ahead of print Feb 24, 2017
J Rehabil Med 2017; 49: 193–203
Correspondence address: Per Ertzgaard, Department of Rehabilitation Medicine, University Hospital of Linköping, Garnisonsvägen 10, SE-581 85 Linköping, Sweden. E-mail: per.ertzgaard@liu.se
Although the exact prevalence is unknown, it is estimated that more than 12 million people worldwide could be affected by spasticity (1), and that 12–27% of these have disabling spasticity, depending on the aetiology (2). Substantial evidence demonstrates that spasticity has a negative impact on patients, causing physical impairment (e.g. pain, pressure sores, contractures), limitation of activities, dependence on caregivers, restricted participation in family and social life, and decreased overall quality of life (3, 4).
Numerous definitions for spasticity exist (5), although that provided by Pandyan et al. (6) has been advocated during recent years: “disordered sensorimotor control resulting from an upper motor neuron lesion, presenting as intermittent or sustained involuntary activation of muscles”. Spasticity is a common complication of upper motor neurone syndrome, and can occur when areas controlling movement are damaged, most often by brain injury disorders, such as or cerebral palsy (CP), traumatic brain injury (BI) or stroke, or by spinal cord disorders, such as spinal cord injury (SCI) or multiple sclerosis (MS) (7). Although heterogeneous, the causes of spasticity share a common pathophysiology, in that the damage disrupts the pathways that regulate activity in alpha motor neurones, causing a change in the balance of signals between the nervous system and the muscles. This imbalance leads to increased activity (excitability) in the muscles, resulting in overactive segmental reflexes. Normally when a muscle is rapidly stretched out, a stretch reflex is triggered and the muscle contracts to maintain muscle length and limb position. To allow smooth, non-jerky, coordinated movement, the segmental reflexes must be inhibited to allow the muscle to relax (i.e. stretch). The main neurotransmitter to achieve this is gamma aminobutyric acid (GABA), which is released by neurones in the spinal cord via descending inhibitory impulses from the brain. However, if the descending inhibitory impulses from the brain (and thus GABA) are cut off through disease or injury, inhibition becomes insufficient; instead, excessive muscular contraction during the muscle stretch takes place, resulting in abnormal muscle tone (hypertonicity).
The severity of spasticity varies from mild to severe according to the level of muscle tone (measured by the Ashworth scale or a modified Ashworth scale in most studies) and the level of disability in performing daily activities (8–10). The use of oral medication to treat spasticity is indicated when spasticity interferes with daily functioning, i.e. causes pain, disturbs sleep or affects activities of daily life. In addition, persistent muscular stiffness and spasms can lead to contracture (permanent stiffness of the muscle, tendon or joint, with decreased range of motion) that can be painful and disabling. Thus, treatment aims to reduce muscle tone in order to facilitate movement and limit contracture. However, some patients rely on excess muscle tone when transferring or ambulating, or to maintain posture. Therefore, the use of antispasmodic drugs needs to be tailored to each patient’s specific needs, to find the correct balance. Commonly-used oral drugs include baclofen, tizanidine, diazepam, and dantrolene, which have differing modes of action, but all are aimed at reducing muscle tone and/or spasms (11).
Oral baclofen is used more frequently than other antispasmodic agents to treat spasticity (8). Baclofen is a GABA-agonist that is thought to selectively bind to presynaptic GABA-B receptors, resulting in hyperpolarization of motor horn cells (12) and a subsequent reduction in the hyperactivity of muscle stretch reflexes, clonus, and cutaneous reflexes that elicit muscle spasms (13). Although widely used, baclofen is mainly water soluble and so does not readily cross the blood-brain barrier (14). As a result, patients may require a high dose to treat their spasticity effectively, which can cause intolerable side-effects (15). As an alternative, baclofen can be delivered directly to the cerebrospinal fluid (CSF) in the intrathecal space, bypassing the blood-brain barrier entirely. This allows a much lower dose to be used to achieve similar CSF concentrations as oral baclofen; it has been determined that the intrathecal baclofen (ITB) dose is 100–1,000 times smaller than the oral daily dose (16), which means that a higher CSF concentration can be achieved at a lower plasma concentration than would be achieved with an oral medication (17, 18). As a result, the central nervous system side-effects of oral baclofen (e.g. sedation, drowsiness, headache) may be reduced (12). The fact that baclofen is only slightly lipid soluble means that baclofen remains in the CSF after ITB therapy, with a relatively long half-life (90 min) (19). There is a 4:1 gradient in drug distribution between the caudal and rostral parts of the spinal cord, favouring high levels of action at the spinal level vs the brain and thus further decreasing cerebral side-effects (20). In addition, animal studies have shown that there is a steep gradient of baclofen along the spinal axis, meaning that during slow intrathecal infusion (20 µl/h) most of the baclofen seems to remain around the catheter tip used for the CSF delivery (21). The clinical implication of this is that the catheter position in relation to the targeted spinal cord segment may be critical to efficacy.
This review aims to systematically evaluate the available evidence for oral baclofen,in order to determine: (i) the efficacy of oral baclofen in spasticity treatment in comparison with placebo or active comparators; (ii) the associated complications or adverse events of oral baclofen; (iii) whether the dosage of oral baclofen changes with the disease severity and duration of spasticity. The results are expected to provide a useful overview of the role of oral baclofen in the management of spasticity, no matter the origin or severity of the condition, and could indicate when intrathecal administration should be considered.
A literature search was carried out of all studies published until 4 June 2014, limited to full-text studies in English or European languages that could be translated easily (Appendix S1). Medline, EMBASE and the Cochrane library were electronically searched, while hand-searching of reference lists of included studies and systematic and non-systematic reviews was used as a supplementary measure to ensure that all relevant studies were included. Search terms used individually or combined included “baclofen”, “spasticity” and “oral”; words related to the outcomes of interest were not used, in order to keep the search broad and to ensure that all relevant studies could be assessed.
Studies were considered eligible if they fulfilled the following inclusion criteria:
Studies were excluded if they were in non-humans or in vitro, evaluated a pooled population across countries, or were conference abstracts, case reports, pilot studies or unpublished. One reviewer independently screened the titles and abstracts of identified references, and a 10% sample was assessed by a second reviewer. Any discrepancies were resolved through discussion.
Data was extracted from each included study and comprised study characteristics (e.g. type of study, outcomes assessed, comparators, etc.) and patient characteristics (e.g. number of patients, sex, age, origin, severity and duration of spasticity), as well as the results with regard to muscle tone (Ashworth scale or similar instrument), frequency of spasms, disability, quality of life, the subjective impression of treatment, and reporting of adverse events (AEs). Two reviewers independently assessed the risk of bias in included studies as “low”, “high” or “unclear”, based on the score using critical appraisal skills program (CASP) checklists (22).
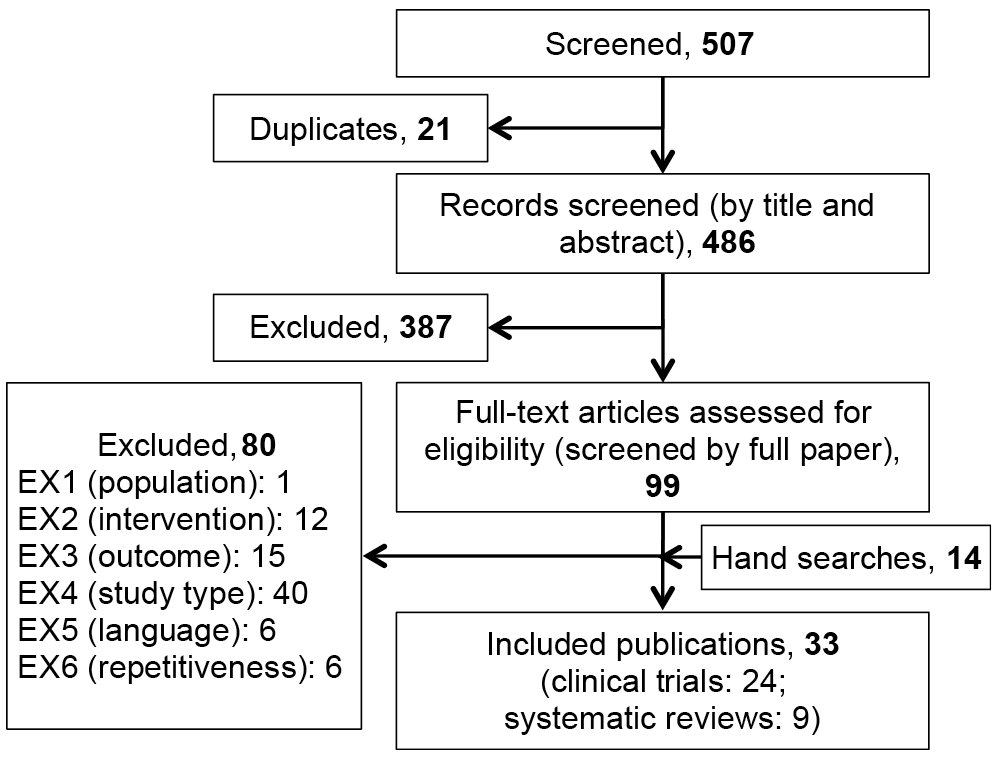
In total, 507 potentially relevant publications were identified from the electronic database searches, of which 21 duplicates were excluded. After screening the titles and abstracts, 387 articles were excluded. A further 80 were excluded as they did not meet the inclusion criteria when reviewed on full text. In addition to the remaining 19 papers, 14 eligible papers were identified from manual searches. Therefore, 33 publications met the inclusion criteria and were included in the systematic review (Fig. 1).
Fig. 1. PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flow diagram of included/excluded studies.
Of these, 24 were clinical trials (20 RCTs, 2 comparative, quasi-experimental studies, 2 open-label studies) and 9 were systematic literature reviews (Table I and Appendix S2). Ten studies were placebo-controlled, while 12 used active comparators. Eighteen studies related to spasticity of spinal origin (15 MS, 3 SCI), while 6 were of cerebral origin (3 CP, 2 BI, 1 post-stroke). Most studies were relatively old (17 published pre-1990, 7 post-1990), often with small sample sizes (mean 42.7 patients, range 10–166) and of short duration (generally between 10 days and 3 months, with 2 longer-term studies of 1 and 6 years).
Table I Study and patient characteristics of included studies
The severity of spasticity was clearly reported or could be calculated using Ashworth values (Ashworth score 1–2 , 2–3, and 3–4 for mild, moderate, and severe spasticity, respectively) in 16 trials, and was deemed mild-to-moderate (1 study), moderate (5), moderate-to-severe (7) or severe (3). The mean age of the patients ranged from 2 to 64.9 years, while the mean duration of spasticity (where reported) ranged from 4 to 26.6 years.
In total, 16 of the 24 clinical studies were at low risk of bias (using the criteria outlined in Appendix S1), while the risk was unclear in 7 studies; only 1 study was considered at high risk of bias (an open-label study in SCI) (Appendix S2). The quality of the 24 clinical studies was graded as moderate to high for MS, CP and BI/stroke, and low for SCI. The risk of bias in the 9 systematic reviews was low in 3 studies, unclear in 5 studies, and high in 1 study (Appendix S2).
The efficacy of oral baclofen with regard to improvements in muscle tone, spasms, disability and subjective impression, according to the origin of spasticity, is outlined in Table II.
Table II. Efficacy outcomes reported in included studies
Open-label studies. In patients with SCI, oral baclofen was shown to improve spasticity and spasms in the majority of patients (23). However, the study in patients with BI did not detect a significant difference in muscle tone or spasms after using oral baclofen (24).
Comparison with placebo. Overall, oral baclofen was significantly superior to placebo at reducing muscle tone in 5 out of 10 placebo-controlled studies (2 MS studies, 1 in spinal cord lesions, 1 in CP, and 1 in stroke) (25–29), and improving spasms in all 3 studies that assessed this outcome (1 in spinal cord lesions and 2 in MS) (25, 26, 30).
Seven studies in MS evaluated the effects of oral baclofen on spasticity (25–27, 30–32). Baclofen was significantly more effective than placebo at improving muscle tone (55–72% of patients experienced an improvement with baclofen compared with baseline vs 0–17.4% with placebo) (25–27) and spasm frequency (42–72% vs 6.3–16% of patients) (25, 26, 30). One study demonstrated that improvement in disability was significantly greater with baclofen (34.8% of patients) compared with placebo (30.4% of patients) (26); however, in 2 other studies the improvement in disability was comparable between the baclofen and placebo groups (30, 32). Two studies indicated that patients or investigators believed baclofen to be better than placebo, but the results were either not statistically significant (31) or no p-value was provided (25).
In one of the 2 placebo-controlled studies in patients with CP, baclofen was significantly superior to placebo with regard to an improvement in muscle tone, such that baclofen was preferred by the majority of patients and investigators (28). In contrast, the other study did not exhibit a statistically significant difference in muscle tone between baclofen and placebo (33). In patients with stroke, baclofen significantly reduced muscle tone and disability measured with the Oswestry index compared with placebo (29).
None of the placebo-controlled studies measured the effects of oral baclofen using standardized quality-of-life instruments.
Comparison with active comparators. Overall, there was no significant difference in efficacy between oral baclofen and the active comparators at reducing muscle tone (34–42), improving spasms (34, 36–38, 40, 42, 43) or reducing disability (34, 40, 42, 44).
Eight studies in MS compared oral baclofen with other anti-spasticity drugs; 6 against tizanidine (34–38 ,44) and 2 against diazepam (43, 45). There were no significant differences between baclofen, tizanidine or diazepam with regard to improvement in muscle tone (34–37, 38) or spasm frequency (34, 36–38, 43). The only statistically significant difference was that 75% of patients preferred baclofen rather than diazepam in one study (no preference in the remaining patients) (43); other studies also indicated a trend towards a preference for baclofen (34, 45).
A similar scenario was observed in the 2 comparative studies in patients with SCI, with no significant difference in muscle tone or spasms between oral baclofen and clonidine or cyproheptadine (39), or transcutaneous electrical nerve stimulation (TENS) (40). In the 1 comparative study in CP, the improvement in muscle tone was comparable between baclofen and eperisone, but patients in particular expressed a preference for eperisone (41). In patients with BI, there were no significant differences between baclofen and tizanidine with regard to muscle tone and spasms, although the global assessment indicated a trend in favour of tizanidine (p = 0.057) (42).
In one study, both baclofen and TENS showed an improvement in Functional Independence Measure (FIM) and Functional Disability Score (FDS) compared with baseline (40). Similarly, in a comparison of baclofen vs tizanidine disability improved in a significant number of patients (42). However, there were no significant differences between the groups. This result was confirmed in the study by Smolenski et al. (34). In contrast, neither tizanidine nor baclofen induced significant changes in neurological disability (Kurtzke’s scale) or in functional disability (Pedersen’s method) in the study by Stien et al. (36).
None of the active-controlled studies measured the effects of oral baclofen on quality of life.
The baclofen starting dose varied from 5 to 30 mg/day, independent of the baseline degree of spasticity. The highest dose varied from 20 to 120 mg/day (Table III), and did not appear to increase between moderate to severe spasticity. Further analysis showed that there was no relationship between the baclofen dosage and the severity or cause of spasticity, although the median minimum dose was slightly lower in BI and stroke patients (10–12.5 mg/day), while SCI patients appeared to tolerate a higher maximum dose (up to 200 mg/day) (Table III). There was no correlation with the number of adverse events (Fig. 2a). However, there was a correlation between the maximum daily baclofen dosage and the duration of spasticity (R=0.55) (Fig. 2b), in that the longer the duration of spasticity, the higher the baclofen dose required to manage symptoms.
Table III. Relationship between baclofen dosage and severity or cause of spasticity
Fig. 2. Correlation between maximum baclofen dosage and (a) number of adverse events (n = 16 studies), and (b) duration of spasticity (n = 11 studies).
The safety profile of oral baclofen compared with placebo or active comparators, according to the origin of spasticity, is outlined in Table IV.
Table IV. Adverse events reported in included studies
Comparison with placebo. Adverse events were more common with oral baclofen than with placebo in all studies, reported in 26–73% vs 4–27%, respectively, of patients with MS (25, 27, 31, 46), 25% and 40% vs 0 and 5% of patients with CP (28, 33), and 50% vs 15% of stroke patients (29). Overall, nausea, somnolence and paraesthesia were most commonly reported for baclofen.
Comparison with active comparators. Adverse events were common with oral baclofen, tizanidine and diazepam, and affected a similar proportion of patients (between 25% and 60% of baclofen patients (34, 36, 41–43) 33–64% of tizanidine patients (34, 36), and 75% of diazepam patients (43). The most commonly reported adverse events were muscle weakness for baclofen, somnolence and tiredness for tizanidine, and sedation for diazepam. Baclofen caused more adverse events than both eperisone (41) and TENS (40).
This systematic review suggests that, in general, oral baclofen can be effective in reducing muscle tone and spasm frequency in patients with mild, moderate and severe spasticity, with similar results across all origins of spasticity. The outcomes in placebo-controlled trials favoured oral baclofen over placebo, although the differences were not always significant (particularly when low dosages were used). Baclofen was at least as effective as other antispasmodic agents, such as tizanidine and diazepam, with a trend towards preference for treatment with oral baclofen. Few studies evaluated the improvement in disability after treatment with oral baclofen, and the results were contradictory. Only 4 studies showed a significant improvement compared with baseline, with no difference between treatments in 2 of these studies. Of the remaining studies, 3 determined that there was no improvement in disability score compared with baseline, and 2 provided only descriptive data.
However, unwanted adverse events were common with oral baclofen, affecting between 25% and more than 70% of patients. Muscle weakness, somnolence, nausea and dizziness were most often reported (Appendix S2), and are well known side-effects associated with oral baclofen. Events were mostly mild-to-moderate in severity and reversible. Adverse events were always more common with oral baclofen than placebo, but the differences compared with active comparators were not so apparent; oral baclofen appeared to be better tolerated in some studies (34, 36, 42, 43), but not others (38, 41).
Overall, a dosage of up to 80–90 mg/day was used to treat moderate to severe spasticity (Table III). The median maximum dosages used were similar across the indications (50–80 mg/day, with the lowest dose in stroke), although a higher dosage of up to 200 mg/day was tolerated in SCI patients. In fact, baclofen is used predominantly for lower limb spasticity in SCI and MS and is often the drug of first choice; its efficacy in spasticity of cerebral origin (i.e. CP, BI and stroke) is less well established (47, 48). We did not observe a clear relationship between the dosages of baclofen used and the severity or cause of spasticity (Table III), or the number of adverse events (Fig. 2a). This is surprising, as clinical experience shows that higher dosages are normally required to treat severe spasticity, and that higher dosages can result in an increased number of adverse events. Although it has been reported that adverse events are more likely to appear at dosages ≥ 60 mg/day in severe spasticity (49), this was not observed in our review. However, few studies (n = 16) report both the baclofen dosage and the baseline severity or number of adverse events; therefore, it is difficult to substantiate what is observed in clinical practice. A closer look at the studies suggests that a rapid increase in the daily dose during the titration period was accompanied by a greater number of adverse events than a slow increase. In addition, there was a correlation between the final dosage of baclofen and the duration of spasticity: the longer the patient had had spasticity, the higher the baclofen dosage used to relieve symptoms (Fig. 2b). This finding is not unexpected, as the severity of spasticity may increase over time (50), particularly in MS (51); the majority of the studies in our review were in MS, which may explain the increase in baclofen dosage over time. In general, a maximum baclofen dosage of 80–90 mg/day was used in patients who had had spasticity for more than 10 years (Fig. 2b). These results, combined with the fact that there was large variation in the baclofen starting dose (5–30 mg/day), indicate that the baclofen dosage used should not be standardized, but should be adapted and titrated according to the specific needs of each patient (47).
The findings of this review are consistent with those of previous systematic reviews, in which oral baclofen was determined to be effective at relieving spasticity (49, 52–54) with no significant differences in efficacy compared with other antispasmodic agents (49, 51–58). Adverse events were common with oral baclofen in these reviews, ranging between 10% and 75%; similar to our review, all adverse events were well-known side-effects associated with the oral formulation and were rarely severe, were reversible and appeared to be dose related (49). The largest review of 30 trials found no significant differences in the rate with oral baclofen compared with tizanidine (52). Muscle weakness as side effect was reported to be more apparent with oral baclofen compared with tizanidine in most (49, 52–55, 57), but not all (56, 58), reviews. A review in SCI, CP and cerebrovascular disease patients stated that neurological events seemed to be dose-related and tended to disappear when doses were reduced (55).
Adverse events are generally regarded to be the limiting factor in using oral baclofen (47, 49, 59). The poor lipid solubility of oral baclofen means that the drug does not readily cross the blood-brain barrier, and so cannot always be titrated to a high enough dose to provide effective relief (47, 49, 60–62). Increasing the dosage does not significantly increase the concentration at the site of action in the CSF, but instead results in high plasma levels (47, 61–63). As a result, spasticity is often not well controlled, leading to a significant loss of function with continued pain and care-related problems (64), combined with side-effects that may be intolerable (15, 47). Thus, there is a need for action in patients who fail to respond adequately to oral baclofen.
An alternative is ITB. A study in severe spasticity of cerebral origin suggests that ITB therapy can provide effective long-term management, with effects that do not diminish over time (> 5 years) (65). As with oral baclofen in our review, the effects of ITB are likely to be independent of the underlying disease (as indicated in a recent case series of spasticity of spinal vs cortical origin (66)). ITB therapy represents an important adjunct in the management of severe spasticity, allowing physicians to continue using baclofen (which is effective in many patients), but administered in a way that maximizes the efficacy of baclofen while minimizing its drug-related side-effects. Adverse events do occur with ITB, which may be drug-related (e.g. drowsiness, somnolence, nausea, vomiting), occurring in 4.4–54% of patients, or device/procedure-related (e.g. infection, catheter migration or disconnection, pump dysfunction, CSF leak, spinal headache, etc.), occurring in approximately 20–36% of patients (19, 67–72). A greater number of adverse events have been reported during the titration phase (67, 69), when patients are allowed to continue with oral medication and when the optimal dosage of intrathecal baclofen has not yet been achieved. As with oral baclofen, careful management is required during ITB therapy to prevent overdose (leading to drowsiness or respiratory depression, for example) and, in particular, abrupt withdrawal of baclofen (usually the result of faulty delivery); continued withdrawal may result in rhabdomyolysis or multiple organ failure, or may mimic sepsis, malignant hyperthermia, autonomic dysreflexia, or neuroleptic–malignant syndrome (19). However, such events are relatively rare and can be managed if the patient is treated immediately (49). It has been determined that the risk for adverse consequences of ITB therapy does not exceed the benefits in patients with spasticity (49). Nevertheless, it is important to understand that ITB therapy is an invasive surgical procedure that requires a highly-specialized set-up, managed by an experienced team that must be able to carefully follow up each patient and adjust treatment (including the baclofen dosage and pump programming) according to their specific needs. Yet although it is a therapy that requires a long-term commitment from both patients and physicians, ITB therapy has proven effective at reducing spasticity, as well as providing other benefits, such as increased independence, greater ability to self-care, increased mobility, reduced muscle pain and fatigue, and better sleep (19). Therefore it is important to fully consider the risk–benefit ratio, and that the potential risks of an implantable device are understood and carefully weighed against the greater efficacy with ITB therapy.
This systematic review is the first to focus on the effects of oral baclofen in all origins of spasticity and across all severities. However, there are limitations to the available data that should be considered. Few of the included studies were recent, and only 2 have been published since 2000. In addition, most trials were small-scale (< 50 patients) and short-term (usually < 3 months). This makes it difficult to truly assess the long-term efficacy and safety of oral baclofen in spasticity, a symptom that usually requires long-term management. Only half of the studies included demonstrated a difference between oral baclofen and placebo. Larger, longer-term studies would be helpful to determine the full extent of the efficacy and safety of oral baclofen, which is commonly used in the management of spasticity. Further evidence comparing the efficacy and safety of oral baclofen with ITB therapy would also be beneficial, as this is currently lacking. Finally, the lack of clinical studies on baclofen having disability, goal attainment and quality-of-life as outcomes needs to be addressed, as this is an increasingly important factor that should be measured when treating diseases of a chronic nature.
In conclusion, oral baclofen appears to be effective in the management of spasticity, regardless of origin or severity, and reduces muscle tone and decreases spasm frequency to a significantly greater extent than placebo, and is comparable with other oral antispasmodic agents. However, the lack of consistency in outcome measures across studies makes it difficult to draw firm conclusions. In addition, there is a need to measure the impact on disability, goal attainment and quality of life in this chronic condition. Oral baclofen seems to be the preferred drug of choice, but adverse events are common. Intrathecal baclofen, which is expected to be more effective than oral baclofen at a much lower dose, resulting in a reduced risk of adverse events, may be a viable alternative in patients who require high doses of oral baclofen for optimal efficacy, but who experience intolerable side-effects as a result, or who fail to respond to the maximum recommended dose of oral baclofen.
This review was funded by Medtronic International Trading Sárl.
The authors would like to thank Deborah Nock (Medical WriteAway, Norwich, UK) for medical writing and editorial assistance on behalf of Medtronic Sàrl.
Conflicts of interest: Per Ertzgaard has received consultancy fees unrelated to this research from Medtronic, and has worked on educational projects with Allergan and IPSEN, but otherwise reports no conflict of interest.


 Click to show fullsize
Click to show fullsize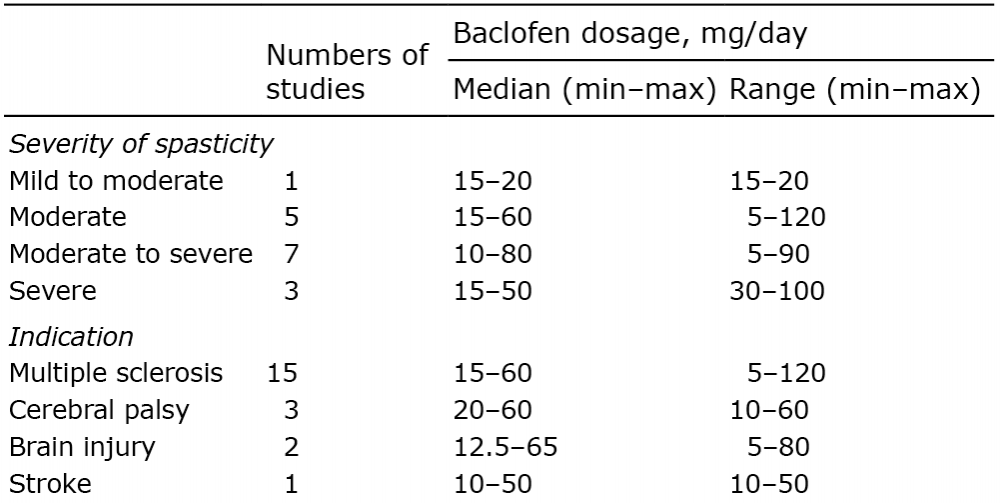 Click to show fullsize
Click to show fullsize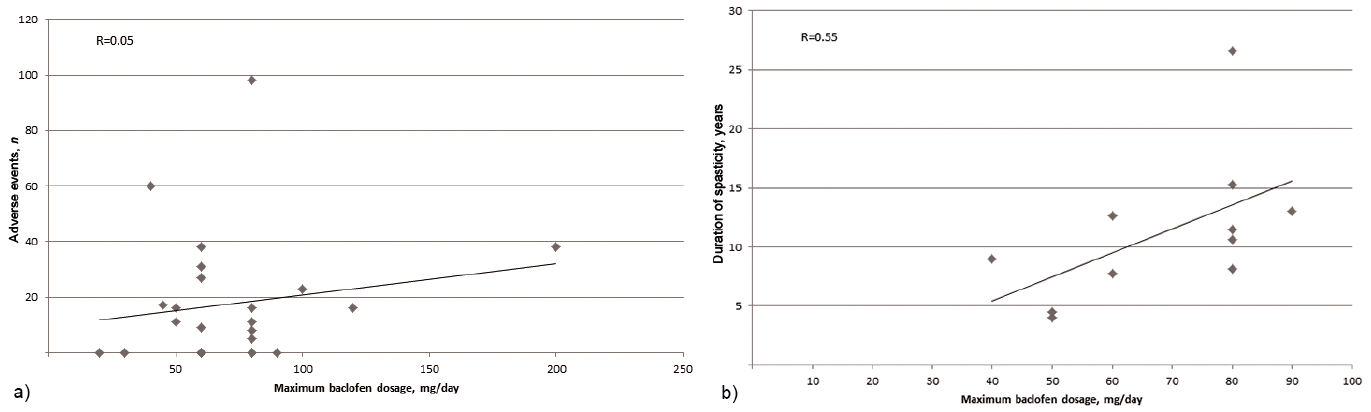 Click to show fullsize
Click to show fullsize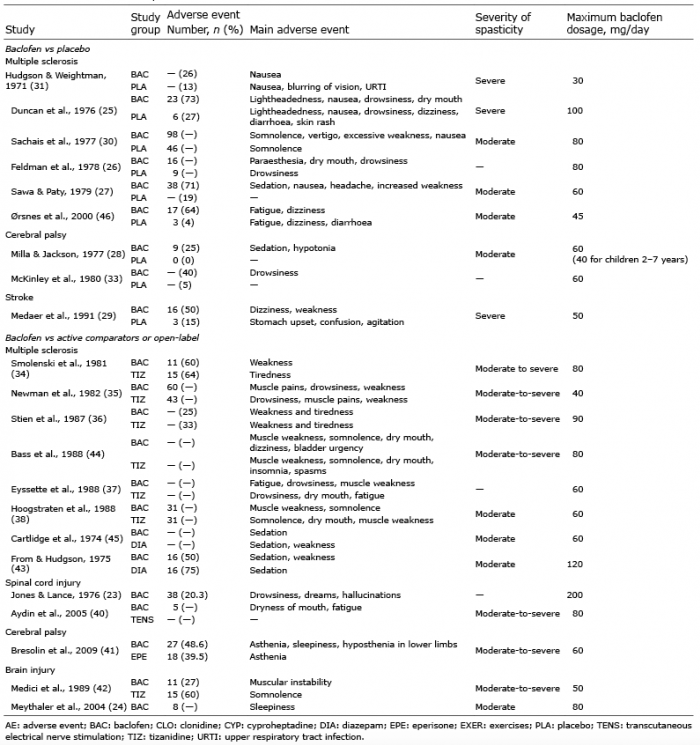 Click to show fullsize
Click to show fullsize