
From the 1Centre for Human Movement Sciences, and 2Centre for Rehabilitation, Department of Rehabilitation Medicine, University of Groningen, University Medical Centre Groningen, Groningen, The Netherlands, 3School of Biological Sciences, Centre of Sport and Exercise Science, University of Essex, Colchester, UK, 4Knowledge Centre for Sport Netherlands, Ede, 5Centre for Sports Medicine, University of Groningen, University Medical Centre Groningen, and 6Hanze University of Applied Sciences, Research Group Healthy Ageing, Allied Health Care and Nursing, Groningen, The Netherlands
Objective: To describe professionals’ perceptions of factors that facilitate or hamper the implementation and continuation of a physical activity promotion programme in rehabilitation.
Design: This study used a qualitative design.
Methods: Semi-structured interviews (n = 22) were conducted with rehabilitation professionals (n = 28) involved in the implementation of a physical activity promotion programme. Two additional interviews were conducted with the programme coordinators (n = 2). The study involved 18 rehabilitation organizations implementing the programme that targets people with disabilities or chronic diseases. Organizations were supported in the implementation process by the programme coordinators.
Results: Commonly perceived facilitating factors were: involvement of committed and enthusiastic professionals; agreement with their organizations’ vision/wishes; the perceived additional value of the programme; and opportunities to share knowledge and experience with professionals from other organizations. Commonly perceived hampering factors were: uncertainty about continuing the programme; limited flexibility; and lack of support from physicians and therapists to implement the programme.
Conclusion: Professionals perceived a heterogeneous set of factors that facilitate and/or hamper the implementation and continuation of a physical activity promotion programme in rehabilitation. Based on these findings, recommendations were formulated to enhance embedding of physical activity promotion during and after rehabilitation.
Key words: people with disabilities; active lifestyle; sports; sustainability; rehabilitation professionals; semi-structured interviews.
Accepted Feb 3, 2017; Epub ahead of print Apr 21, 2017
J Rehabil Med 2017; 49: 00–00
Correspondence address: Femke Hoekstra, Centre for Human Movement Sciences, University of Groningen, University Medical Centre Groningen, PO Box 196, NL-9700 AD, Groningen, The Netherlands. E-mail: f.hoekstra@umcg.nl
In the Netherlands, sports activities are currently considered to be important components of effective rehabilitation care (1–3). The embedding of sports into rehabilitation can play a role in promoting an active lifestyle in patients with disabilities. Unfortunately, research showed that the incorporation of sports during rehabilitation in itself was not enough to maintain an active lifestyle in all patients after discharge from rehabilitation (3). Van der Ploeg et al. (3) showed the necessity to offer patients a period of tailored counselling focusing on sports and daily physical activities after rehabilitation to attain a physically active lifestyle in their home setting. The results of this randomized control trial showed that self-reported physical activity levels of patients who received tailored physical activity counselling after rehabilitation improved up to one year after discharge (3).
Following these previous and positive findings, the evidence-based programme “Rehabilitation, Sports and Exercise” (RSE) was introduced and prepared for dissemination in Dutch rehabilitation care (4). The RSE programme specifically targets people with physical disabilities and/or chronic diseases, to encourage them to participate in sports and daily physical activities during and after rehabilitation (4, 5).
However, the implementation of a new programme into rehabilitation practice is challenging (6, 7). The continuation of a programme over an extended period may be even more difficult (8–11). Insights into factors at the level of the organization that influence these processes are important, to understand how and why the programme is (not) successfully implemented and continued over time (12, 13). Although many studies has been conducted on the identification of factors influencing the implementation of evidence-based programmes in healthcare settings (14, 15), less is known about enabling and constraining factors of the implementation and continuation of a physical activity promotion programme (e.g. RSE programme) in rehabilitation care.
The aim of this qualitative study was therefore to describe professionals’ perceptions of factors that facilitate or hamper the implementation and continuation of a physical activity promotion programme in rehabilitation.
A qualitative design using semi-structured interviews with rehabilitation professionals was chosen to gain in-depth insights about factors influencing the implementation and continuation of a physical activity promotion programme in different rehabilitation settings based on professionals’ experiences, attitudes and expectations. The study is part of the Rehabilitation, Sports and Active Lifestyle (ReSpAct) study (4, 5). The study protocol was approved by the ethics committee of the Centre of Human Movement Sciences of the University Medical Centre Groningen. All invited professionals agreed to participate and approved the use of the collected data for scientific purposes.
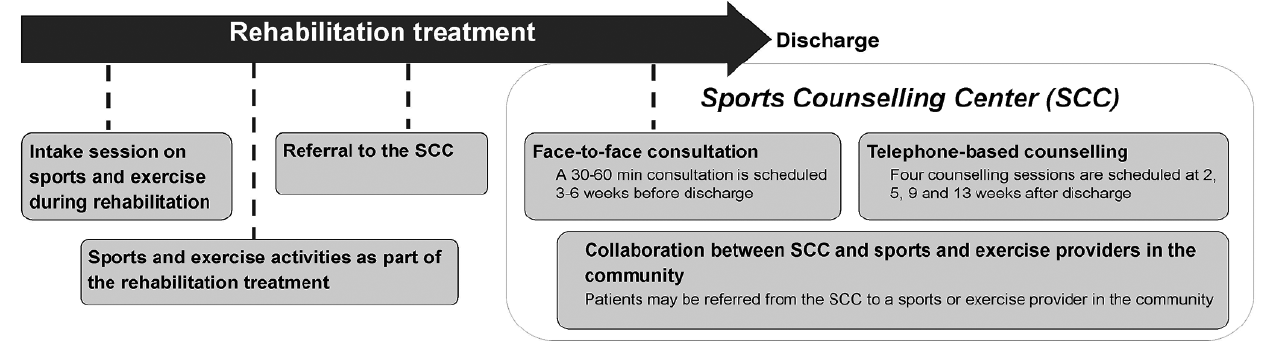
Professionals from 12 rehabilitation centres and rehabilitation departments of 6 hospitals were involved. The RSE programme was implemented in all 18 organizations with the support of a Dutch organization1. Fig. 1 illustrates the content of the RSE programme. A detailed explanation of the RSE programme has been provided elsewhere (4, 5).
1Stichting Onbeperkt Sportief, this national organization aimed for a larger participation within disabled sports and physical activity and the development of suitable and accessible sports facilities. From January 2016, Stichting Onbeperkt Sportief became part of Knowledge Center for Sport Netherlands.
Fig. 1. Content of the Rehabilitation, Sports and Exercise (RSE) programme. The programme consists of activities during and after a rehabilitation treatment.
The implementation of the programme consisted of the following key steps:
Each participating organization appointed a project leader to coordinate the implementation of the programme within the organization, and 1 or more counsellors to execute the programme (4, 5). Two national programme coordinators were engaged to support and coordinate the implementation on a national level. Table I shows activities that were part of the implementation strategy.
Table I. Activities related to the implementation strategy
From the involved organizations (n = 18), all project leaders and a selection of counsellors were invited to participate in a semi-structured interview by researcher FH. Counsellors were selected to participate if they were actively involved in the implementation of the RSE programme. Prior to each interview, professionals were informed about the content and aims of the interview. Furthermore, both national programme coordinators were invited to participate in an interview about their experiences with disseminating the programme and perceived influencing factors.
Interviews with project leaders were conducted using a topic list that was based on a theoretical framework (16). This framework displays 3 main phases of an introduction process (adoption, implementation, continuation), categories of determinants (socio-political, organization, programme, professional, patients) and the implementation strategy (16).
Each interview started with an open question about professionals’ general experiences with the RSE programme. Thereafter, open questions were asked about their experiences with the implementation of the RSE programme and potential factors that influenced this process. Probing questions were asked about the way the RSE programme was implemented and executed in the concerning organization. Furthermore, specific questions were prepared about professionals’ experiences with activities that were part of the implementation strategy and initiated by programme coordinators. Subsequently, project leaders and counsellors were asked about their expectations on the continuation of the RSE programme after the programme period (2012–2015) and possible influencing factors.
Appendix 1 sets out the content of the interviews. Prior to each interview, professionals received this diagram by e-mail in order to motivate them to think about perceived facilitators and barriers. Moreover, this diagram was used as a tool to guide the interview.
Appendix 1. Visual overview of content of the interview with rehabilitation professionals. Professionals received this diagram by e-mail in order to motivate professionals to think about perceived facilitators and barriers. The diagram was based on the theoretical framework of Wierenga et al. (2013). The “start, “implementation” and “embedment” represent the 3 main phases (adoption, implementation, continuation) of the theoretical framework. The grey box with “influencing factors” contains the 5 categories of the “implementation determinants” presented in the framework. The activities related to the implementation strategy were not included in the diagram that was send to professionals prior to the interview, but these were added to the diagram and explained by the researcher at the end of the interview. Moreover, this diagram was used as a tool to guide the interview. Dates of signature of declaration to participate, signature of agreement to participate and the official approval of the project plans varied among organizations.
The content and topic list of the interviews with the 2 programme coordinators differed from the interviews with the project leaders and counsellors. During the first interview with the programme coordinators, open questions were asked about their experiences with the implementation of the RSE programme within each organization separately (n = 18). A second interview was conducted in order to obtain information about programme coordinators’ perceptions on facilitating and hampering factors to the implementation and continuation of the programme in rehabilitation organizations.
All interviews were audiotaped and transcribed verbatim. To familiarize with the data, transcripts were read several times and a summary was written of each transcript. The first 2 transcripts were independently coded by FH and MvB using an open coding procedure (17). Based on these 2 transcripts a code scheme including potential facilitating and hampering factors was developed. Consequently, all transcripts were coded using this coding scheme by researcher FH, involved in the evaluation of the RSE programme, and a second coder (MvB, research assistant 1 or research assistant 2). Coding was performed in ATLAS.ti (Scientific Software Development GmbH, Berlin, Germany). Meetings with all coders were organized to discuss discrepancies in coding procedures and to reach consensus. Subsequently, codes representing similar topics were combined into broader factors. Facilitating and hampering factors were then classified into the different groups of the theoretical framework (16). Finally, results were discussed with an expert panel consisting of members with different backgrounds and expertise (physician/researcher RD, researcher CvS, researcher FJH). Two other members of the panel (LvdW and MD) reflected on the final results and recommendations. A selection of quotations was translated into English to illustrate the results.
A total of 22 interviews with rehabilitation professionals (n = 28) involved as project leader (n = 21) or counsellor (n = 7), were held between November 2014 and March 2015. Of these, 22 interviews, 6 were conducted with 2 professionals (i.e. double interview design). Interview duration ranged from 40 to 115 min (mean ± 70 min). Two interviews of duration ± 80 min per session were conducted with the 2 programme coordinators in October 2014 and April 2015. Table II gives an overview of the rehabilitation setting and characteristics of the conducted interviews.
Table II. Setting and characteristics of all conducted interviews (n = 24)
Tables III and IV show the perceived facilitating and hampering factors reported by professionals for the implementation and continuation of the RSE programme.
Table IV. Facilitating and hampering factors to the continuation of the “Rehabilitation, Sports and Exercise” programme
A selection of quotations to illustrate the findings is presented in Table V.
Table V. Examples of quotations to illustrate the findings
Professionals mentioned factors related to the following categories: “socio-political context”, “organization”, “programme”, “professional”, “patients” and “implementation strategy”. Factors related to the “patients” were only mentioned in the implementation phase. A few factors were only stated by professionals working in a general hospital (Tables III and IV).
Counsellors mainly talked about factors related to the execution of the programme, such as the flexibility of providing counselling sessions, the additional value of the programme and characteristics of their patients. Project leaders named factors related to diverse categories both more on a management level (e.g. organizations’ vision/wish, financial aspects) as well as on a more practical level (e.g. flexibility and compatibility of the programme). The 2 programme coordinators emphasized the engagement of physicians in the implementation of the programme, and the support from rehabilitation professionals within the organization to implement and continue the RSE programme. The next section provides a detailed description of perceived facilitating and hampering factors.
Network. During implementation, almost all organizations have started or have strengthened their collaborations with the municipal governments, non-profit foundations and/or providers of sports activities, such as sports clubs or fitness clubs. Good collaborations and a good network enabled counsellors to gain (up-to-date) information about possibilities to participate in sports and exercise activities for disabled persons in the region.
Uncertainty about the continuation. Almost all professionals expressed their uncertainty about the continuation of the programme after 2015 (Table IVa), which was thought to be related to the expected changes in the financial system of the Dutch rehabilitation care. Since, in general, financial resources for healthcare have been under pressure, professionals were worried about the future, and some managers were therefore restrained in their decisions to expand the SCC.
To overcome this uncertainty, professionals suggested the importance of continuing the nationwide cooperation among rehabilitation organizations after the programme period. This could help to share ideas and seek for financial possibilities to embed the RSE programme into the routines of the organizations after the programme period.
Vision and wishes. A commonly mentioned facilitating factor for both phases was the fact that the content of the RSE programme was in line with the organizations’ vision and/or wishes (Tables III and IV). In some organizations there was already an operating SCC before the start of the programme period. Participating in the RSE programme gave them the opportunity to implement a SCC at more locations of their organization and/or to intensify and expand the guidance at the existing SCC. Other professionals reported that participating in the RSE programme provided the opportunity to integrate sports and exercise, including tailored counselling, in a more structural way.
Moreover, almost all professionals experienced that sports and exercise had received a more important and structural place into rehabilitation care by implementing the RSE programme. Several professionals highlighted the impact of the implementation process on the position of the department “Sports and Exercise Therapy” and the position of sports therapists2 in the multidisciplinary rehabilitation team (Table V).
2Sports therapists are health professionals educated to help and/or encourage people with disabilities or chronic diseases to participate in sports and exercise activities.
Support from rehabilitation professionals. Support from rehabilitation professionals from all levels (managers, physicians, therapists) was a commonly perceived influencing factor (Tables IIIb and IVb). At the start of the implementation, some professionals encountered insufficient support from physicians and/or therapists to execute the RSE programme, which hampered the referral of patients to the SCC. Consequently, both project leaders and counsellors have put a lot of effort into creating a committed environment regarding the promotion of sports and physical activities during rehabilitation. For the continuation phase, support from managers and physicians was emphasized as an important influencing factor, since these professionals can have an impact on decision-making processes (Table IVb).
One project leader working in a hospital was not satisfied with the decision to implement the RSE programme (Table V). The project leader explained that the involved manager decided to participate in the RSE programme, despite the fact that physicians of the rehabilitation department did not support it. One reason for the lack of support, as reported by the project leader, was that most patients who were treated at the rehabilitation department were not eligible to be referred to the SCC. In addition, facilities for sports and exercise activities in that hospital were perceived to be limited and were experienced as a barrier to the integration of sports and exercise during rehabilitation.
Physiotherapy and sports therapy. A commonly perceived barrier was the lack of support from physiotherapists to refer patients to the SCC. Several physiotherapists did not see the necessity of setting up a SCC. Professionals recognized a hierarchy in which physiotherapy was seen as a more important component of a rehabilitation treatment than sports therapy. Improving the communication and collaboration between sports therapists and physiotherapists was a successful way to overcome this barrier in one hospital. On the other hand, in other organizations, the lack of support from physiotherapists remained a hampering factor (Table V).
Sports and exercise promotion in hospital care. Most rehabilitation departments of hospitals did not recognize active lifestyle as a key point of attention in their provided care. This resulted in uncertainty about future plans among professionals in hospitals. The collaboration between a rehabilitation department in a hospital and a neighbouring rehabilitation centre was reported as a facilitating factor to the implementation and continuation of the RSE programme in a hospital setting, since rehabilitation centres were, in general, more “sport minded” compared with hospitals.
Committed and enthusiastic counsellors. Almost all professionals stated that the involved counsellors were committed to and enthusiastic about the implementation of the RSE programme (Table IIIc). This enthusiasm was reported as an important factor to successfully implement the programme, because counsellors had a major role in promoting the RSE programme (including SCC) within their organization and in creating support from their colleagues. In addition, professionals mentioned that rehabilitation professionals who were not committed to executing the RSE programme were not selected to work as a counsellor in the SCC.
Engagement of a rehabilitation physician. For many professionals, the engagement of physicians in the implementation was reported as a facilitator for the implementation and continuation of the programme (Tables IIIc and IVc). Since physicians play a key role in the multidisciplinary team, it was important that they had a positive attitude towards the RSE programme. Furthermore, professionals explained that an enthusiastic and committed physician could enable the implementation by creating support from their physician colleagues.
Additional value. Almost all professionals were positive about the content and nationwide design of the RSE programme. Moreover, the additional value of the RSE programme, especially the tailored counselling sessions, was clear for all professionals (Table V). Counsellors experienced that the guidance they provided to their patients was effective, which was a clear stimulating factor.
Flexibility. Despite the fact that professionals were very positive about the programme, they also mentioned that counsellors experienced difficulties in applying the protocol of the counselling sessions to all patients. Counsellors preferred to be more flexible in the number and times of counselling sessions, in order to be more in line with the needs and wishes of their patients. Because several counsellors perceived problems in reaching patients by telephone, counselling sessions were sometimes performed by e-mail. In general, counsellors had positive experiences with performing counselling sessions by e-mail. They mentioned that the counselling by e-mail was time-consuming and could be carried out in a more flexible way. However, most counsellors preferred a telephone conversation with their patients. Almost all professionals reported that a more flexible execution of the counselling sessions was required for the continuation (Table IVd).
According to the professionals, patients participating in the RSE programme generally had a positive attitude towards physical activities and appreciated the tailored support from the SCC. Counsellors experienced that the support to patients in low stages of behavioural change (low level of motivation) was more challenging compared with patients in higher stages of behavioural change (high level of motivation). The socio-economic status of patients also played a role in the execution of the programme. Some patients had limited financial resources for engaging in physical activities, which hampered a referral of patients to activities outside the organization and/or in personal environment.
Activities on national level. Professionals reported that a financial incentive gave the opportunity to accelerate the implementation process. However, some professionals preferred to receive financial incentives over a longer period.
The extent to which professionals communicated with programme coordinators and received advisory support varied among organizations. However, independent of the degree of support provided, professionals experienced it as a positive factor (Table V).
For almost all professionals, the meetings organized with the involved professionals contributed positively to the implementation and continuation of the RSE programme. Professionals emphasized the additional value of sharing knowledge and experiences with professionals from other organizations. The planning of meetings for a selection of professionals, such as meetings for managers/project leaders and meetings for counsellors, provided additional benefits.
Project leaders and counsellors were very positive about the structured training in motivational interviewing and highlighted the broad possibilities for application to general rehabilitation care.
Activities at the organizational level. To create awareness and to provide information about the RSE programme within the organization, project leaders and counsellors gave oral presentations to other departments in the organizations, e-mailed information to colleagues and/or published information on the internal website/newsletter of the organization. Professionals highlighted the importance of regularly repeating these activities (Table V).
The results of this study showed that professionals perceived a heterogeneous set of factors that facilitated or hampered the implementation and continuation of a physical activity promotion programme in rehabilitation care. Some factors, such as collaboration with other organizations, financial resources, organizations’ vision/wishes, support from professionals, uncertainty about future, and additional value of the programme, were reported to influence both phases. Other factors were perceived only as influencing factors during implementation (e.g. collaboration among professionals within the organization, patients’ characteristics, activities related to the implementation strategy) or continuation (e.g. conclusions of the ReSpAct study).
The literature showed that financial resources/reimbursement, time available, professionals’ attitude and support from organization are frequently cited influencing factors to the implementation of a physical activity (promotion) programme in rehabilitation care (18–22) or in primary healthcare (15, 23, 24). These factors were also reported by professionals involved in the current study to hamper and/or facilitate the implementation process. Some factors specifically related to the RSE programme (e.g. name of “sports counselling centre”, linked ReSpAct study, motivational interviewing) were not mentioned at an earlier stage in literature.
In contrast to previous studies (14, 25, 26), lack of knowledge or skills to implement the programme was not experienced as a hampering factor by professionals in the current study. An explanation might be that the professionals involved in the current study were actively supported during the implementation. Several activities related to the implementation strategy (i.e. meetings, courses in motivational interviewing, up-to-date materials) may have contributed to the fact that the professionals did not report lack of knowledge and skills as a hampering factor. Although the effectiveness of using a multifaceted strategy to support an implementation process is debatable (7, 27, 28), the experiences of the professionals in the current study suggest that the different activities used to support the implementation of the RSE programme may have contributed positively to this process. The question remains, however, whether the combination of activities applied in the current study was the most optimal and efficient way to successful implementation. Future research should therefore focus on (cost)effectiveness of (combinations of) activities to support the implementation and continuation of physical activity promotion in rehabilitation.
Although professionals were very positive about the implementation process and were supported to successful implementation, they all expressed their uncertainty about the continuation of the programme. Almost all factors (e.g. reimbursement, vision/wishes of the organization, collaboration, professionals’ attitude/motivation) that were perceived by professionals as influencing the continuation of the programme were stated in previous literature on influencing factors of physical activity promotion in primary healthcare (23, 26). However, no studies have been found focusing on the identification of factors influencing the continuation/sustainability of a physical activity promotion programme in rehabilitation care. The importance of distinguishing between phases has been pointed out several times (14, 16, 26, 29, 30). As shown in the current study and based on previous literature conducted in other healthcare settings (8, 14, 15, 26, 31), we know that reimbursement of the programme, effectiveness of the programme and policy of the organizations are important factors to successfully continue a physical activity promotion programme.
In addition to these findings, we formulated recommendations based on 3 “umbrella” factors that may contribute to the sustainability of the performing activities to promote physical activity during and after rehabilitation (Table VI).
Table VI. Recommendations to enhance (further) embedding of physical activity promotion activities during and after rehabilitation
The first factor is the flexibility of the programme. Professionals in the current study mentioned that a more flexible execution of the programme was required to continue the programme within the context of their organization. Since rehabilitation care is characterized by a multidisciplinary setting with a heterogeneous patient group, the programme should allow a flexible approach. The importance of adapting an evidence-based programme to the healthcare context has been highlighted by several other researchers (8, 32, 33). According to Damschroder et al. (32), a programme includes “key components” and “adaptable elements”. To maintain effectiveness of the programme, these “key components” should be implemented according to the protocol, while changes may be allowed in the “adaptable elements”. In the current study, the “key components” of the RSE programme were clearly defined (i.e. intake, face-to-face sessions, counselling) (4). Concerning the “adaptable elements”, we do not know how many and what kind of adaptations (i.e. e-mail-based counselling, use of other social media) are acceptable to maintain the desirable outcomes on patient level. Although different adaptations may have a different influence on patient outcomes (8, 34, 35), adaptations seem essential to sustain the programme within the organization (8, 33). As a result, the way physical activities are integrated in rehabilitation may differ between patient groups and between organizations. Based on literature from other settings (33, 36), this variation may be used to further optimize the procedure of embedding physical activities into rehabilitation care. Collecting data about the number and type of adaptations made within each organization is therefore highly recommended (36).
The second factor is the attitude of the professionals. All professionals emphasized the enthusiastic and committed counsellors and physicians as being important for implementing and continuing the programme. They highlighted that it is important to continuously create awareness, knowledge and support related to performing physical activities during and after rehabilitation among all members of the multidisciplinary team. To ensure that this will continue on the longer term, we recommend appointing (a group of) professionals working in the organization who are responsible for a structural embedding of physical activities into rehabilitation. In this way, “local ownership” is created, which has been previously shown to contribute positively to successful sustainability (31, 33, 37, 38).
In Dutch rehabilitation care, most rehabilitation centres and some hospital rehabilitation departments include “sports therapy” as a separate field in rehabilitation care, which has the responsibility to embed sports and physical activities into rehabilitation (1). However, the current study showed that some professionals experienced a lack of support from physiotherapists to embed physical activities into rehabilitation. In line with previous literature (27, 39) we found that good communication and collaboration between members of the multidisciplinary team (e.g. sports therapists, physiotherapists, physicians) during implementation seems also essential for successful continuation. Again, “local ownership” may facilitate this process.
The third factor is the nationwide collaboration. To overcome future barriers, professionals suggested continuing the nationwide collaboration among organizations. Again, to ensure the continuation of this collaboration, a (group of) professionals or a foundation should be responsible for this. In the same way, a “nationwide ownership” should be established. Previous studies showed that such an ownership may facilitate the sustainability of evidence-based programmes in healthcare settings (31, 33). In the current study, the programme coordinators organized a membership of the RSE programme, which includes continuous (advisory) support, information and up-to-date materials from programme coordinators. All rehabilitation centres and rehabilitation departments of hospitals are invited to become a paid member of the RSE programme after the programme period (2012–2015). Thus, a “national ownership” is created and collaboration among organizations on the national level may continue, which is expected to strengthen the RSE programme. This may positively contribute to a structural embedding of physical activities into rehabilitation in the long term.
A limitation of this study is the possible selection bias. We only selected professionals working in 1 of the organizations participating in the RSE programme (4). It is likely that these professionals were, in general, more positive about the implementation of the physical activity promotion programme than other rehabilitation professionals. Furthermore, professionals received support during the implementation phase with the use of a multifaceted strategy. This may explain why, in general, professionals were very positive about the implementation process. Future studies should investigate whether rehabilitation professionals working in organizations that were not supported in implementing a physical activity promotion programme perceive other facilitating and hampering factors. On the other hand, because organizations received support during the implementation phase, the start of the continuation phase was clearly defined. Therefore, professionals were able to distinguish between factors that influence the implementation and/or continuation. Another limitation of the current study is that we did not collect data about influencing factors perceived by physicians. It is therefore possible that we missed some important information. However, our sample still consisted of a heterogeneous group of professionals that perceived a heterogeneous set of influencing factors.
Lastly, this study built upon the results of a previous RCT using self-reported physical activity outcome measures (3). It is thus possible that the successful results of this previous RCT may be overestimated (40). Therefore, the ReSpAct research group is currently re-evaluating the outcomes of the RSE programme at the patient-level (5). Although the ReSpAct study uses also self-reported measures, longitudinal data are available from a large and heterogeneous study population (n = 1,719). Moreover, objective data regarding physical activity levels are obtained from a subgroup of patients in order to gain insight into the validity and reliability concerning self-reported physical activity measures in the context of the present study.
In conclusion, rehabilitation professionals perceived a heterogeneous set of factors that facilitate or hamper the implementation and continuation of a physical activity promotion programme in rehabilitation care. We formulated 3 recommendations to enhance (further) embedding of physical activity promotion during and after rehabilitation: (i) implement key components of an evidence-based procedure and adapt these to the local multidisciplinary context; (ii) establish local ownership; and (iii) establish national ownership.
The authors would like to thank Daan van Kooten and Eline Brans for their assistance in data collection and data analyses. The authors would also like to thank the following organizations for their support in the ReSpAct study: Adelante Zorggroep, Bethesda Ziekenhuis, De Trappenberg, De Vogellanden, Maasstad Ziekenhuis, Medisch Centrum Alkmaar, Militair Revalidatiecentrum Aardenburg, Revalidatiecentrum Leijpark, Revalidatiecentrum Reade, Revalidatie Friesland, Revant, Rijnlands Revalidatiecentrum, RMC Groot Klimmendaal, Scheper Ziekenhuis, Sint Maartenskliniek, Sophia Revalidatie, Tolbrug Revalidatie, and ViaReva.
This study was funded by the Dutch Ministry of Health, Welfare and Sport (grant no. 319758) and supported by Stichting Onbeperkt Sportief.
The authors declare no conflicts of interest.


 Click to show fullsize
Click to show fullsize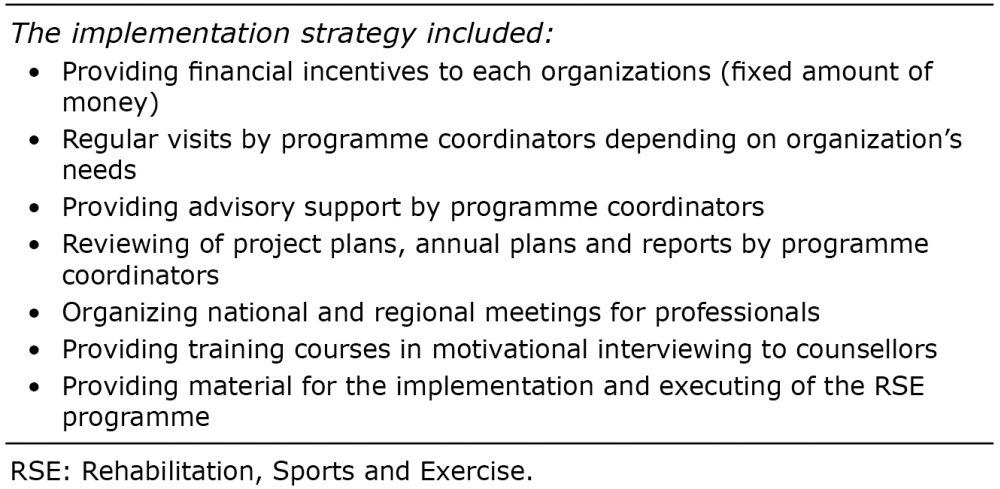 Click to show fullsize
Click to show fullsize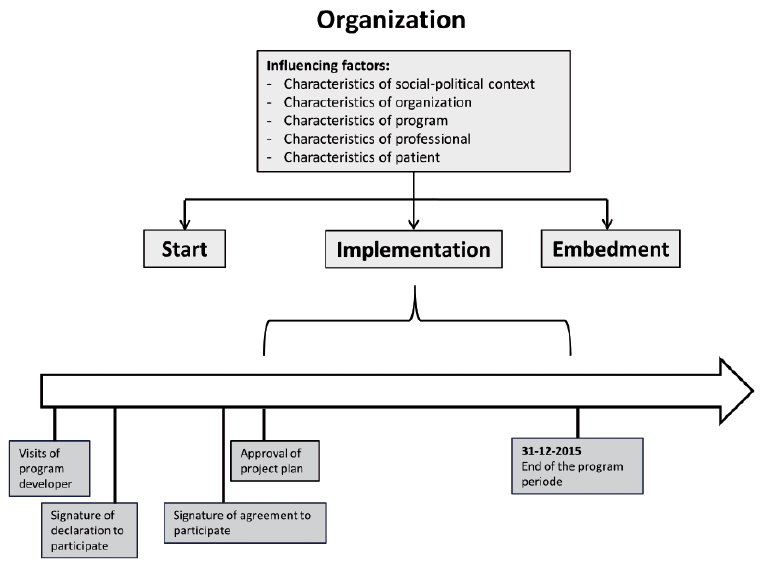 Click to show fullsize
Click to show fullsize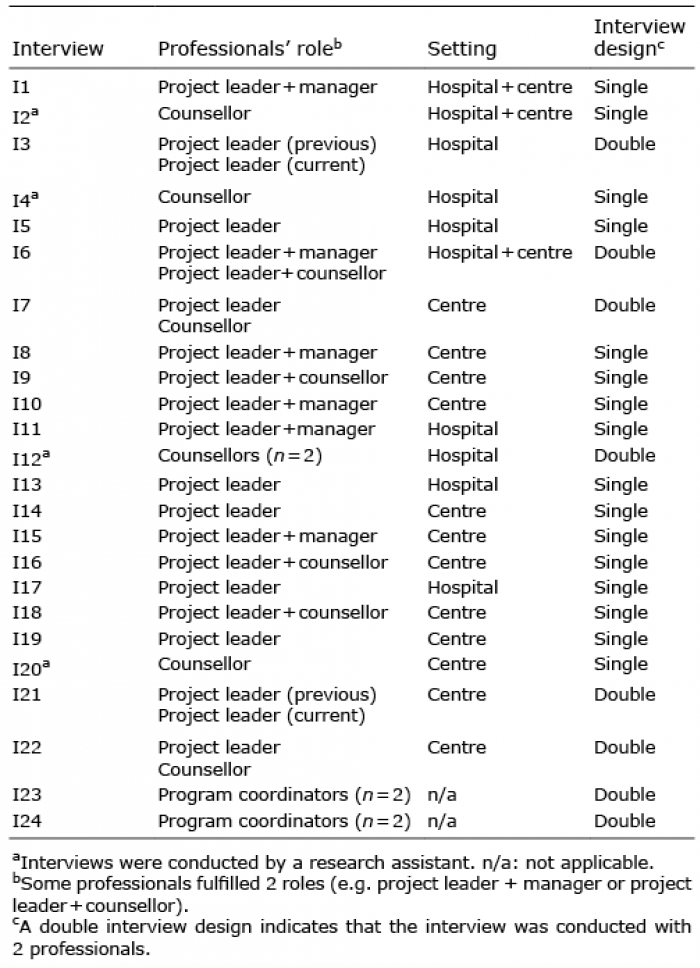 Click to show fullsize
Click to show fullsize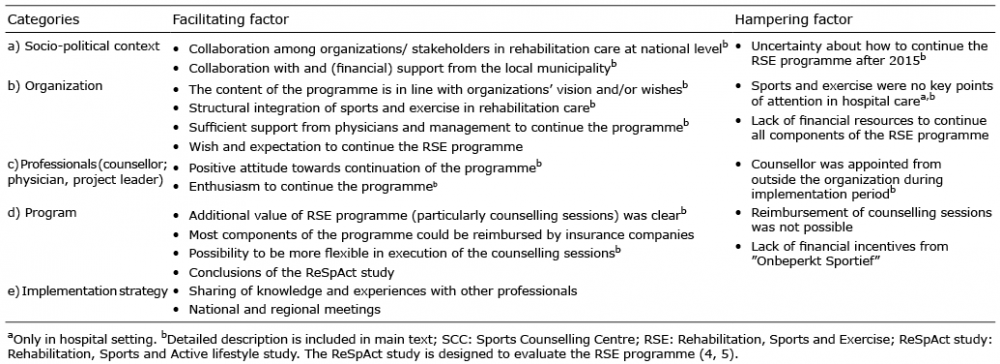 Click to show fullsize
Click to show fullsize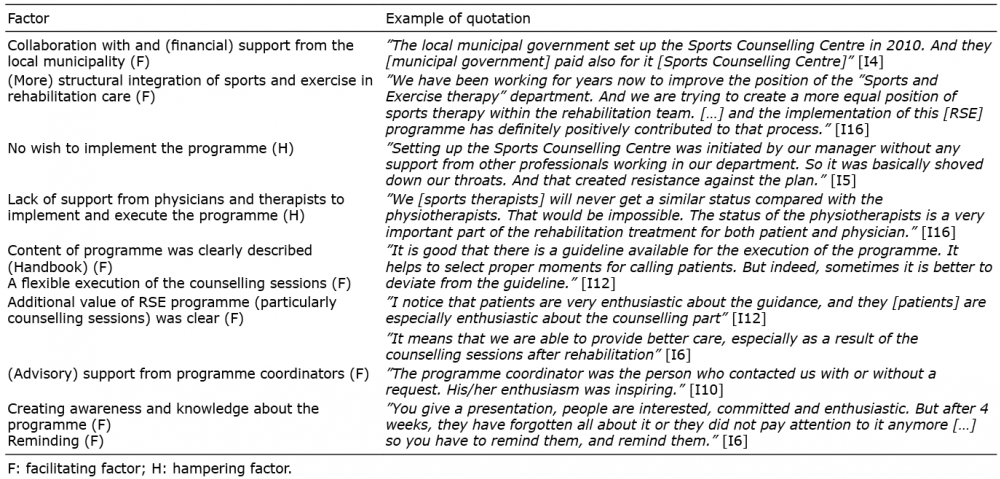 Click to show fullsize
Click to show fullsize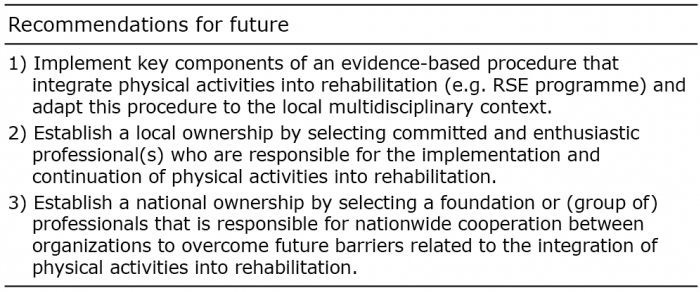 Click to show fullsize
Click to show fullsize