
From the 1Center of Rehabilitation Medicine, West China Hospital, Sichuan University, Chengdu, Sichuan Province, 2Interdisciplinary Division of Biomedical Engineering, The Hong Kong Polytechnic University, Hong Kong, 3Institute for Disaster Management and Reconstruction, Sichuan University-The Hong Kong Polytechnic University, Chengdu, Sichuan Province, 4Department of Gastroenterology, The First Affiliated Hospital of Nanjing Medical University, Nanjing, 5Department of Rehabilitation Medicine, Wuxi Rehabilitation Hospital, Wuxi, Jiangsu Province, China and 6Epidemiology of Functioning, Swiss Paraplegic Research, Nottwil, Switzerland
Objective: Previous epidemiological studies of adole-scent idiopathic scoliosis in mainland China have had diverse results. The aim of this cross-sectional study was to determine the epidemiology of adolescent idiopathic scoliosis based on a representative sample
city, Wuxi, in eastern China.
Methods: Primary and secondary school students aged 10–16 years were enrolled in the study. Physical examination and Adam’s forward bending test, combined with scoliometer measurements were performed at school-based screening. Students with an angle of trunk inclination of 5° or more were referred for whole-spine X-ray. The threshold for confirmed diagnosis was a Cobb angle of 10° or more.
Results: A total of 79,122 students were screened. The overall prevalence of adolescent idiopathic scoliosis in Wuxi City was estimated as 2.4%. Girls had a higher prevalence in each age subgroup compared with boys. Higher prevalence was found in individuals with lower body mass index. Mild and moderate curves were the most common types in our study.
Conclusion: The prevalence of adolescent idiopathic scoliosis in this region was slightly higher. Medical resources should be considered for children with lower body mass index and high risk of scoliotic progression. Measurement with a scoliometer would be suitable for mild-to-moderate scoliotic deformities, while alternative methods should be developed for those with severe deformities or higher body mass index.
Key words: adolescent idiopathic scoliosis; prevalence; scoliosis screening; positive predictive value; body mass index; Cobb angle.
Accepted Apr 13, 2017; Epub ahead of print May 24, 2017
J Rehabil Med 2017; 49: 00–00
Correspondence address: Mansang Wong, Interdisciplinary Division of Biomedical Engineering, The Hong Kong Polytechnic University, Hong Kong, 999077, China. E-mail: m.s.wong@polyu.edu.hk, Chengqi He, Center of Rehabilitation Medicine, West China Hospital, Sichuan University, No. 37, Guo Xue Xiang, Chengdu, 610041, China. E-mail: hxkfhcq2015@126.com
Adolescent idiopathic scoliosis (AIS) develops in the age range 10–16 years and is characterized by a lateral curvature of 10° or more, usually combined with vertebral rotation. The term, idiopathic scoliosis refers to patients in whom it is not possible to find a specific disease causing the deformity (1).
Based on the definition published by the American Commission on Chronic Illness, screening is a “presumptive identification of unrecognized disease or defect by application of tests, examination or other procedures which can be applied rapidly” (2). AIS screening meets this definition as it targets high-risk populations and then refers them to appropriate early intervention, therefore reducing the surgery rate and improving patients’ quality of life physically and psychologically in the near future.
The prevalence of AIS ranges from 0.93% to 12% worldwide (1). As a common spinal deformity in adolescents, early detection of AIS is essential in order to provide appropriate treatment. School-based AIS screening has been performed in many countries since the 1950s. Its necessity and efficacy have been controversial, however, due to evidence of over-prescription of braces, unnecessary radiological exposure rate, and low investment-benefit ratios (3). Professional associations, such as the American Academy of Orthopedic Surgeons (AAOS) and the Scoliosis Research Society (SRS) supported such screening, for example, while the United States Preventive Services Task Force advised against it (4). Nonetheless, it remains the most effective method, not only for detecting patients in the early stage of scoliosis, but also for preventing curvature progression and reducing surgical rate.
Many studies on the prevalence of scoliosis have been carried out in mainland China. In a recent meta-analysis, Zhang et al. reported that the overall pooled prevalence of scoliosis in mainland China was 1.02% among primary and middle-school students (5). Nonetheless, several studies were found to have substantial limitations. Researchers used varying definitions of AIS and study protocols, which made data comparison across studies difficult. Based on lessons learned from previous research, a large AIS screening programme was conducted to determine the prevalence of AIS in Wuxi (eastern China) and to determine the associated factors.
This prospective cross-sectional epidemiological study was performed between April and December 2015 in Wuxi City, Jiangsu Province, eastern China. Primary school (5th and 6th grades) and secondary school (7th to 9th grades) students aged 10–16 years were screened for AIS while undergoing an annual physical examination. All schools in central Wuxi City were enrolled irrespective of their geographical, economic or ethnic background.
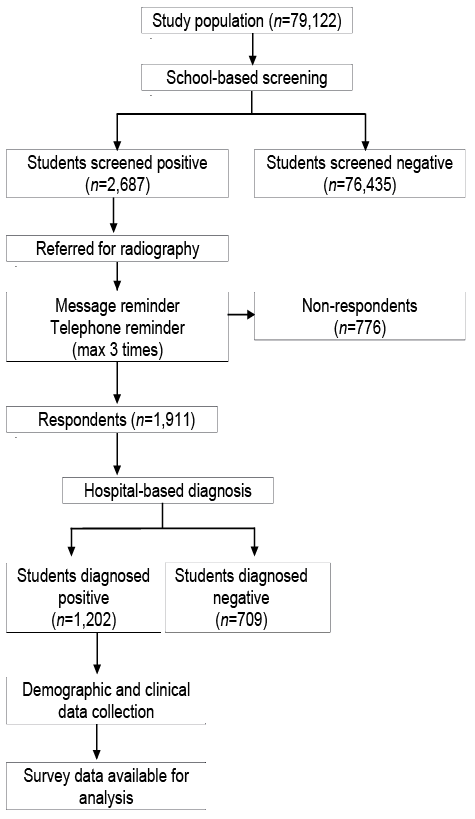
A 2-step screening method including school-based screening (first phase) and hospital-based diagnosis (second phase) was applied in this study (Fig. 1). Ethical approval (ChiECRCT-20150021) was obtained from China Ethics Committee of Registering Clinical Trials ahead of the screening. Its guidelines and regulations, as well as the principles of the Declaration of Helsinki were followed. Teachers, parents and students were informed about the objectives of the study and the details of the examination, and written consent was obtained from all participants and their parents.
Fig. 1. Flowchart of epidemiological study of adolescent idiopathic scoliosis in eastern China including the school-based screening phase and the hospital-based diagnosis phase.
School-based screening was conducted in schools by an experienced screening team consisting of 3 orthopaedic surgeons, 4 rehabilitation physicians, 6 therapists and 2 nurses from Wuxi Rehabilitation Hospital. Boys and girls were examined separately. Physical examinations, including examination of shoulder asymmetry, scapula prominence, unequal waistline or arm span, and abnormalities involving the trunk or spine, such as humps in the ribs or lumbar regions, were performed during this phase. Thereafter, the Adam’s Forward Bending Test (FBT) combined with determination of angle of trunk inclination (ATI) by scoliometer (Orthopedic Systems Inc., Union City, California, USA) were performed, while allowing the upper extremities to hang freely with the palms opposed in a relaxed manner (6, 7). This process took approximately 1 min for each student. Students with an ATI reading of at least 5° or with 2 or more significant clinical signs were re-screened and those screened positive were referred to Wuxi Rehabilitation Hospital for further evaluation with whole-spine posterior-anterior radiography (8, 9). The inter- and intra-observer correlation coefficient (ICC) in measuring the ATI reading was 0.855 (95% confidence interval (95% CI): 0.835–0.875) and 0.880 (95% CI: 0.865–0.895). The scoliometer has a sensitivity of approximately 100% and a specificity of approximately 47% at an ATI reading of 5° (10), while the sensitivity decreases to 83%, but specificity increases to 86% at an ATI reading of 7° (8, 9, 11).
Referred students were the first to again undergo the FBT combined with scoliometer examination, followed by a standing posterior-anterior whole-spine X-ray examination when deemed necessary. The final diagnosis of scoliosis, as defined by the Scoliosis Research Society, was based on Cobb angles of 10° or more, as measured by 2 independent observers (1). When differences occurred consensus was achieved by discussion. Students who were diagnosed with non-idiopathic scoliosis (mainly neuromuscular scoliosis) were excluded at this phase. The intra-observer correlation coefficient in measuring the Cobb angle was 0.954 (95% CI: 0.932–0.976).
Students diagnosed as AIS were recommended for specific intervention by a senior specialist. Students who were screened positive (ATI reading of 5° or more) at the school-based screening phase, but were not diagnosed as AIS patients (Cobb angle of 9° or less) were followed up every 3–6 months.
At the school-based screening phase, data regarding sex, age, weight, height, body fat (measured by Omron Body Fat Analyzer HBF-306; Omron, Japan), resting metabolism, ATI reading and contact information (i.e. name, home address and phone number) were recorded for screened-positive students, while radiological data regarding curve level, Cobb angle and Risser scores were collected once they participated in the hospital-based diagnosis. Students who attended the hospital-based diagnosis and were screened positive were documented as respondents in the database. Conversely, those who were referred for radiography were documented as non-respondents if they did not respond to the reminders (Fig. 1).
All analyses were performed with SPSS 20.0 (IBM Corporation, USA). The PPVs for diagnosis were calculated with the number of diagnosed cases and the number of cases referred by initial screening. The PPVs for treatment were calculated with the number of cases referred to specific treatment groups and the number of diagnosed cases. Age-and-sex growth charts developed by the US Centers for Disease Control and Prevention were used to categorize each student into one of the following body mass index (BMI) subgroups: obesity (BMI ≥ 95th percentile), overweight (BMI ≥ 85th and < 95th percentile), normal weight (BMI ≥ 5th and < 85th percentile) and underweight (BMI <5th percentile) (12). Overall prevalence and prevalence by age, sex, BMI subgroups and curve magnitude were estimated. Curve distribution by age and sex was also estimated.
Unit-non response, i.e. non-attendance at the hospital-based diagnosis although screened positive, was adjusted for by inverse probability weights based on the propensity score method (13). In this study, the basic idea of propensity scores is to replace covariates of both respondents and non-respondents with the predicted probabilities of attending the physical examination among those screened positive. The inverse propensity scores were estimated from a logistic regression model with backward selection of response status on demographics and predictive factors as well as weighted analysis. The idea was to give respondents who are similar to non-respondents a higher weight in the analysis. All analyses were provided for weighted data, since no significant differences were detected between weighted and unweighted data. A p-value less than 0.05 was considered statistically significant and 95% CI was presented.
In total, 79,122 (92%) out of 86,145 primary and secondary school students enlisted in Wuxi City at the time of the annual school examination according to the Ministry of Education participated in this study, comprising 43,258 boys and 35,864 girls. The distribution of screened students according to age and sex is shown in Fig. 2. Among the students who participated in the school-based screening, 2,687 (1,120 boys and 1,567 girls) were referred for radiography because of the detected ATI reading or other significant clinical signs. Eventually, 1,911 screened-positive students participated in the hospital-based diagnostic stage and 776 were lost to follow-up after not responding to several scheduled reminders, as shown in Fig. 1. Descriptive statistics for referred students are summarized in Table I.
Fig. 2. Number of students screened by age and sex for adolescent idiopathic scoliosis.
Table I. Demographic data for study sample for adolescent idiopathic scoliosis
The overall PPV was 63.0% for students with a Cobb angle of 10° or more. It decreased to 48.19% in students who needed to be followed up or undergo exercise training (Cobb angle range 11–24°) according to SRS criteria (1). The corresponding PPVs for those who qualified for bracing (Cobb angle 25–40°) or surgery (Cobb angle 41° or more) were 14.08% and 0.73%. The variations in PPV by sex according to ATI reading and Cobb angle are shown in Tables II and III. Compared with the overall PPV, a similar trend was detected either in girls or in boys. No significant difference was found between girls and boys in each subgroup (χ2 = 0.456, p =0.500 for diagnosis; χ2 = 0.886, p = 0.346 for follow-up and exercise training; χ2 = 0.721, p =0.396 for bracing; χ2 = 0.181, p=0.671 for surgery). In addition, this trend was stable in students with ATI readings of 10° or below, while once it went up to 11° or more the PPVs were no longer consistent.
Table II. Positive predictive value (PPVs) of angle of truck rotation (ATI) reading followed by Scoliosis Research Society (SRS) criteria in girls and boys
Table III. Overall prevalence and prevalence in girls and boys
The overall prevalence of AIS for primary and secondary school children aged 10–16 years in Wuxi City was estimated at 2.4%, with a prevalence of 3.12% in girls and 2.14% in boys, respectively. Girls had a 1.46 times higher AIS prevalence than boys in the current study (see Table III). Cobb angles of those diagnosed ranged from 10° to 45°, with a mean of 18.68° (standard deviation 8.16°).
Detailed overall prevalence and prevalence by age and sex are shown in Table IV. The lowest and highest overall prevalence was found in 10-year-olds (0.05%, 95% CI: 0.03–0.07%) and 16-year-olds (3.77%, 95% CI: 3.64–3.90%), respectively. The data demonstrated an increasing trend in overall prevalence rate with age and the prevalence from 0.53% (95% CI: 0.48–0.58%) to 4.10% (95% CI: 3.96–4.24%) in girls and from 0.64% (95% CI: 0.58–0.70%) to 3.50% (95% CI: 3.37–3.63%) in boys. Moreover, as none of the boys aged 10 years were diagnosed with AIS, the prevalence could be estimated only in boys aged 11–16 years. Girls had a higher prevalence in each age subgroup (with a peak in the 15-year-old age subgroup) compared with that of boys (with a peak in the 16-year-old age subgroup). The highest ratio of girls to boys (2.36:1) for AIS prevalence was found in students aged 13 years.
Table IV. Prevalence by age and sex
Prevalence rates calculated by BMI subgroups and sex are shown in Table V. AIS prevalence rates decreased with BMI. Students who were assigned to the underweight group had the highest prevalence rate both in girls (4.66%, 95% CI: 4.28–5.04%) and boys (2.88%,95% CI: 2.58–3.18%) and the lowest prevalence rate was found in those with obesity.
Table V. Prevalence by body mass index and sex
Prevalence of AIS by curve magnitude and sex is summarized in Table VI. The highest overall prevalence (1.16%, 95% CI: 1.09–1.24%) was found in students with Cobb angles ranging between 10° and 24°.
Table VI. Prevalence by curve magnitude and sex
The overall prevalence decreased to 0.33% (95% CI: 0.30–0.38%) when the curve magnitude became moderate (25–40°), while those who were diagnosed with severe AIS had the lowest prevalence of 0.02% (95% CI: 0.01–0.03%). This decreasing trend of prevalence was consistent in boys and girls. Girls, however, had a higher prevalence of AIS in each curve magnitude subgroup compared with boys and the highest ratio of girls to boys (3.00:1) was detected in the subgroup with the most severe magnitude of curve.
Fig. 3 demonstrates an increasing trend in Cobb angles by age for overall curve distribution as well as distribution for girls, but not for boys.
Fig. 3 Curve distribution by age and sex. (a) Estimated means and 95% confidence interval (95% CI) of Cobb angle by age. (b) Estimated means and 95% CI of Cobb angle by age and sex.
Several tests can be used for AIS screening. For the school-based screening phase, the FBT combined with the scoliometer is a simple and fast method for identifying the presence of minor spinal deformity, although its accuracy is the subject of debate (10). One of the important concerns of school-based screening is over-referral to radiological examination when confirmed diagnosis needs to be made. Higher specificity, sensitivity, positive predictive value (PPV) and negative predictive value (NPV) are preferred; however, suboptimal accuracy was inevitable due to the behavioural non-compliance of the examiners and individual differences of the participants. In addition, it was not ethical to refer screened-negative individuals for X-ray examination, especially in a large-scale screening study. Therefore, PPV becomes the value that was commonly used for accuracy assessment in an AIS screening study and was often between 19.3% and 51.5% in previous studies (5, 11, 14–17). A meta-analysis conducted by Fong et al. investigated the clinical effectiveness of AIS screening and reported a relative low PPV of 28% for diagnosis (15), while a recently published large population-based screening study using a 3-stage design showed a PPV of 78.4% for diagnosis at a referral rate of 6.6% (18). This indicates that the clinical effectiveness of AIS screening can be improved with certain methods, as higher PPVs and lower referral rates are always favoured by researchers. The PPVs in the current study were 63.0% for diagnosis (Cobb angle 10° or more). Compared with the findings of previous studies, the well-trained professionals who had experience from a pilot screening study, which included 11,024 primary school students, may have contributed to the high PPV for diagnosis in the current study (19). It not only can reduce the referral rate, but also can improve the PPV, and, in turn, save medical resources and avoid unnecessary radiological exposure. As shown in Table II, the PPVs of a Cobb angle above 24° were no longer as high as that of a Cobb angle below 25°. In addition, large fluctuations were observed in both girls and boys with ATI readings above 10°. This may be due to the limited sample size of subgroups with a Cobb angle above 24° and those with an ATI reading above 10°. However, the most important factor might be the accuracy of the scoliometer. As reported by Pierre et al., the scoliometer has a sensitivity of approximately 100% and a specificity of approximately 47% at an ATI reading of 5° (10), while its sensitivity drops to 83%, but specificity rises to 86% at an ATI reading of 7° (8, 9, 11). This indicates that the scoliometer would become more reliable as ATI reading increased and the results of the current study for individuals with Cobb angles below 25° and ATI readings below 11° meet these criteria. However, these criteria might not be suitable for moderate and severe cases in the current study. This implied that the scoliometer might not be the best choice for detecting moderate and severe AIS. Non-invasive and efficient technologies (for example, ultrasound) could be considered in future AIS screening studies. Hengwei et al. increased the PPV from 64.8% to 78.4% by adding a re-screening session for individuals with ATI reading of 5° or more (18), indicating that the frequency of evaluation may also be critical in improving the accuracy at the school-based screening phase. In addition, the PPVs in the current study were calculated by dividing the number of students with Cobb angles of 10° or above by the number of students who participated in the hospital-based diagnostic stage. This may have been an overestimation as it seems plausible that students with apparent scoliotic curves may have been more likely to show up for clinical examination.
Many scoliosis screening studies have been performed in mainland China (5); however, there are few reports on AIS prevalence from eastern China. As a medium-sized city, Wuxi is regarded as a developed city in terms of economy, humanity and lifestyle in eastern China. Most residents in this city are native Chinese. In total, 79,122 (92%) out of 86,145 students participated in this study and all the primary and secondary schools in Wuxi City were enrolled. Therefore, it is believed that the results may represent the situation in eastern China. According to the literature, the prevalence of scoliosis in mainland China was 1.02% (5). The current study reported an overall AIS prevalence of 2.4%, which was higher than that in the meta-analysis (5). Factors such as latitude, age, screening technologies, evaluation frequency and diagnostic criteria, may contribute to the variation of the overall prevalence rate. Grivas et al. assumed that the different prevalence rate of scoliosis might be due to lifestyle differences across different geographical latitudes (20). For age range, the pooled overall prevalence was estimated for ages 5–19 years and the ranges varied across independent studies in the meta-analysis conducted by Zhang et al. (5). In terms of screening technologies, evaluation frequency and screening professionals, most of the studies adopted the physical examination and FBT combined with the scoliometer, while some combined physical examination with Moiré topography instead of FBT (21, 22). Tian et al. adopted Cobb angles of 5° or more as the diagnosis threshold instead of 10° or more (23). Hengwei et al. repeated the screening procedure aiming at increasing the PPV and reducing the referral rate (18), while findings reported by Minghelli et al. were only based on the results of the scoliometer (24). As a 2-step AIS screening study, participants in the current study were first screened in the schools and further diagnosed in the hospital by our team consisted of well-trained and experienced orthopaedic surgeons, rehabilitation physicians, therapists and nurses, compared with the screening only conducted by nurses or technicians (25). Nine studies were found to have comparable prevalence rate while the current study reported the highest overall prevalence rate (see Table VII) (21, 22, 26–32).
Table VII. Adolescent idiopathic scoliosis (AIS) screening conducted in mainland China
It was assumed that a larger sample size, multiple screening methods used, well-trained professionals, higher geographical latitude and fewer sunlight hours may contribute to a higher overall prevalence in the current study. Given the importance of various factors, consensus procedure or guideline in AIS screening is needed for future studies. In addition, 2-step diagnostic studies always encounter attrition in the second step. In this case, students who were screened positive at the school-based screening phase might not show up at the hospital for X-ray examination. This could be related to students’ and parents’ limited knowledge about AIS and reluctance with regard to radiographic examination. Potential AIS cases in non-respondents may cause bias with regard to the overall prevalence estimate. However, we believe that this cannot be avoided in any epidemiological studies. Here, we tried to counter this problem by applying inverse probability weights of attending the physical examination among those screened positive. With this method, the prevalence was adjusted by predicting the potential positive cases in non-respondents.
It has been widely accepted that the prevalence rate among girls is higher than that among boys (33, 34). One possible explanation is the interaction between the production of leptin and nervous systems in girls, which would, in turn, initiate the scoliosis. Another possible reason would be that the imbalanced strength of paraspinal muscle along the concave and convex sides of the spine could lead to higher chances of curve progression. Although this was also observed in boys, it is believed that the muscle strength is much weaker in girls compared with that in boys. Our results confirmed this. However, it is interesting to note that a high peak prevalence occurred in 15–16-year-old females (4.10–4.69%) and 16-year-old males (3.50%) respectively, and the highest ratio of girls to boys (2.36:1) was found in 13-year-olds. The results were consistent with the findings of another large population-based AIS screening conducted in Guangdong Province (18) through different professional associations, i.e. the Scoliosis Research Society, the American Academy of Orthopedic Surgeons, the American Academy of Pediatrics, and the Bright Futures guidelines (17), suggested different criteria for screening. Considering that the observed high peak prevalence rate might be due to an accumulated effect along the development of the deformity, it is suggested to conduct the screening 1 or 2 years ahead of the age at which the high peak prevalence was observed. This indicated that the population at high risk in mainland China might be different and the results could serve as reference and guidance for future screening studies in mainland China.
A few studies reported associations between BMI and prevalence rate of AIS. Hengwei et al. used 18 kg/m2 as the threshold for allocating patients to an under- and overweight group and explored the prevalence across BMI subgroups. They found a significantly higher prevalence in students with BMI less than 18 kg/m2. In the current study, patients were allocated into 4 BMI subgroups based on the age-and-sex growth charts developed by the U.S. Centers for Disease Control and Prevention (Table V) (35). The highest prevalence was found in the subgroups with lower BMI. The trend was consistent with the results reported by Hengwei et al. and Hershkovich et al. (18, 36). The latter concluded that the prevalence rate of spinal deformities was significantly greater among underweight patients, and that increased BMI had a protective effect against developing spinal deformities based on a cross-sectional survey of 829,791 adolescents in Israel (36). One of the possible explanations might be the developmental disharmony between autonomic and somatic nervous systems in individuals with lower BMI, which may in turn launch selectively increased sensitivity of the hypothalamus to circulating leptin, with asymmetry as an adverse response (37). In addition, thicker adipose tissue over the spine in patients with higher BMI may have a protective effect. Also, it cannot be excluded that nutrition-related factors are involved.
Approximately 10% of diagnosed cases of AIS require conservative treatment and 0.1–0.3% require surgical correction. As shown in Table VI, mild (Cobb angle of 11–24°) and moderate (Cobb angle of 25–40°) curves were also the most common types in the current study. The ratio of girls to boys increased with curvature magnitude, indicating that progress may occur more frequently in females, which was consistent with the findings of previous studies (33, 34).
A limitation of the current study is the experimental design. As a cross-sectional study, longitudinal data cannot be provided; therefore the change in prevalence in the certain period is unknown. Follow-up screening is necessary in the future in order to detect the effectiveness of screening and scoliotic progression.
This screening study, conducted in Wuxi, eastern China, reported an overall prevalence of AIS of 2.40% and filled the epidemiological blank regarding AIS in this region. It is recommended that more attention and medical resources should be considered for children with lower BMI and high risk of progression of scoliotic deformity. Application of scoliometer measurement appears to be suitable for mild-to-moderate scoliotic deformities, while alternative methods should be developed for those with severe deformities or higher BMI.
The authors appreciated Fen Qu, Ning Sun, Tao Wang, Huabo Li, Lijie Zhang, Bihui Ma, Qiuyan Li, Hanhan Sun and Yingying You for their invaluable support in both the school-based screening and hospital-based diagnostic phase. Guoping Shen and Yangguang Wang were acknowledged for their professional radiological insights regarding AIS. Special thanks are also given to the participants and their parents for joining this study.
Funding for this study was provided by Wuxi Science and Technology Program (WSTP), China (grant number: ZD201408). The WSTP had no further role in study design; in collection, analysis and interpretation of data; in the writing of the report; or in the decision to submit the paper for publication.
The authors declare no conflicts of interest.


 Click to show fullsize
Click to show fullsize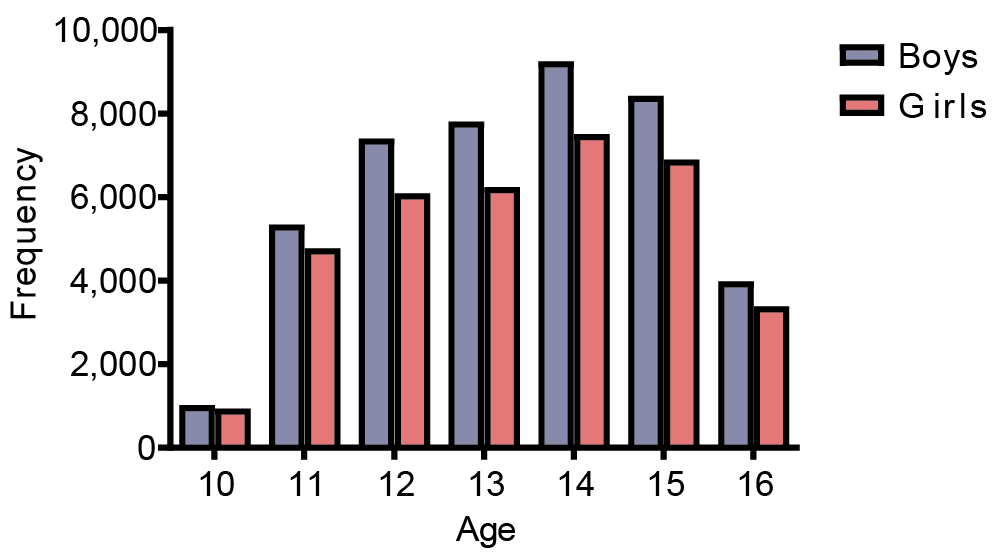 Click to show fullsize
Click to show fullsize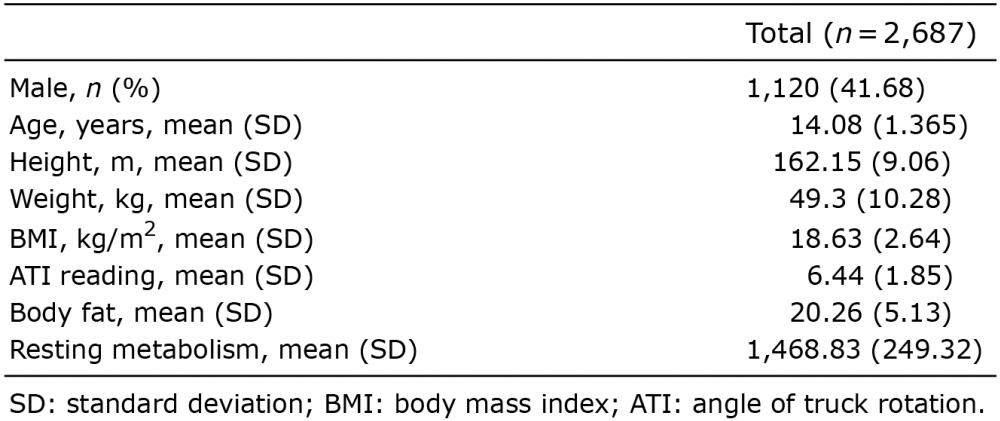 Click to show fullsize
Click to show fullsize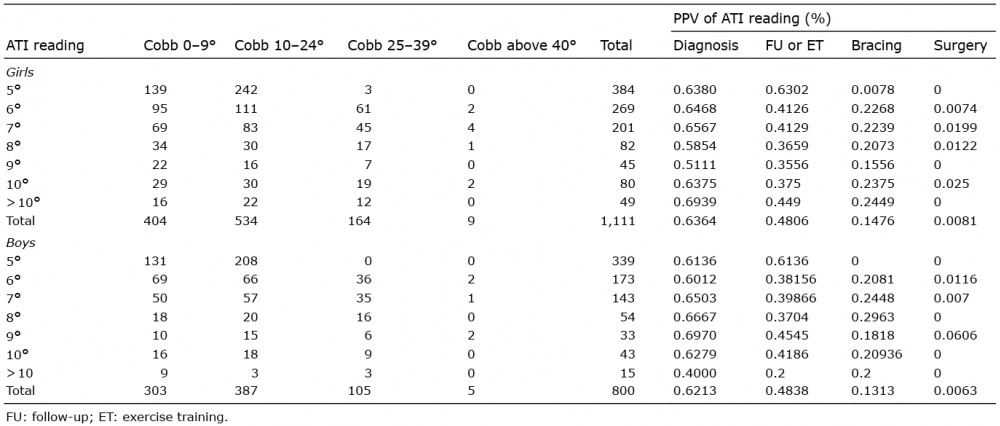 Click to show fullsize
Click to show fullsize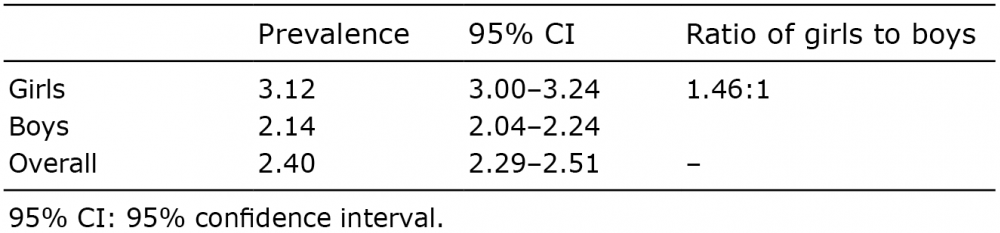 Click to show fullsize
Click to show fullsize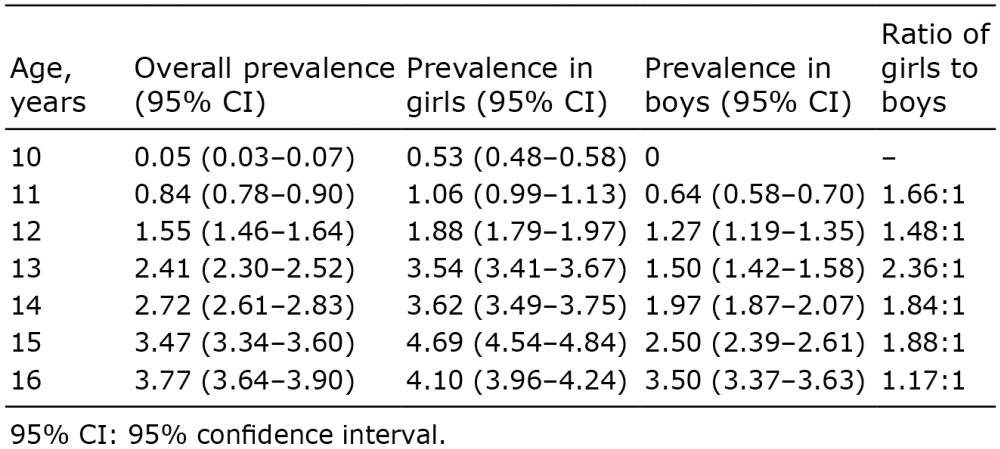 Click to show fullsize
Click to show fullsize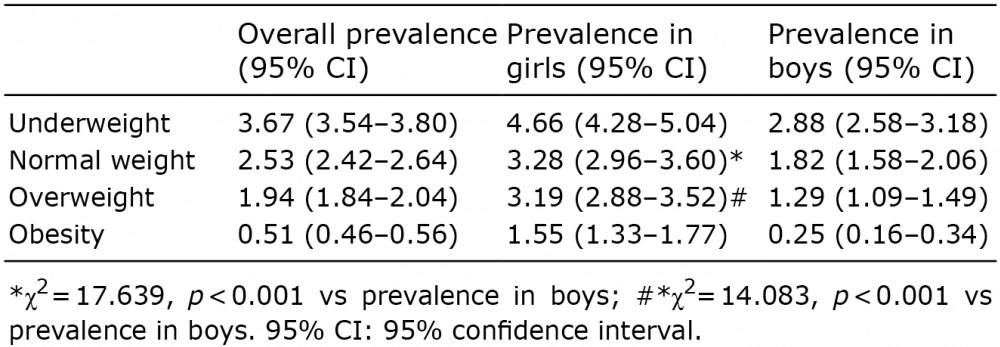 Click to show fullsize
Click to show fullsize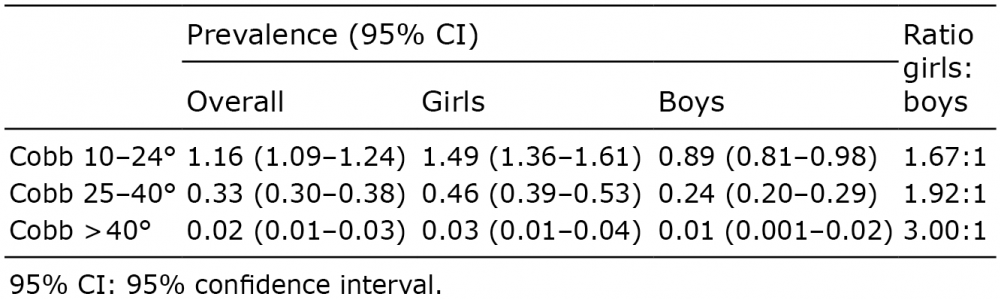 Click to show fullsize
Click to show fullsize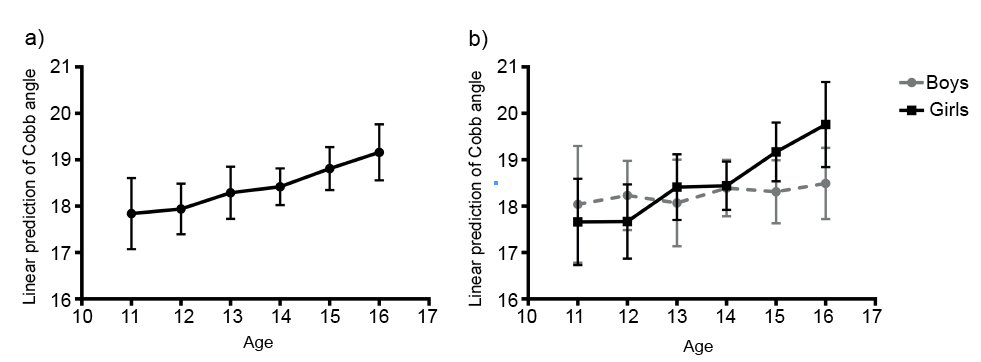 Click to show fullsize
Click to show fullsize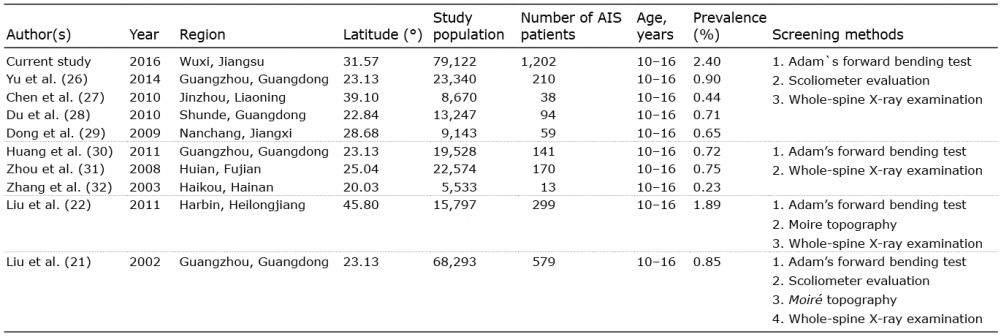 Click to show fullsize
Click to show fullsize