
From the Neurology Department, Ningbo Medical Center Lihuili Eastern Hospital, Ningbo, Zhejiang, 315000, China
Objective: To evaluate the influence of transcutaneous electrical nerve stimulation in patients with stroke through a systematic review and meta-analysis.
Methods: PubMed, Embase, Web of Science, EBSCO, and Cochrane Library databases were searched systematically. Randomized controlled trials assessing the effect of transcutaneous electrical nerve stimulation vs placebo transcutaneous electrical nerve stimulation on stroke were included. Two investigators independently searched articles, extracted data, and assessed the quality of included studies. The primary outcome was modified Ashworth scale (MAS). Meta-analysis was performed using the random-effect model.
Results: Seven randomized controlled trials were included in the meta-analysis. Compared with placebo transcutaneous electrical nerve stimulation, transcutaneous electrical nerve stimulation supplementation significantly reduced MAS (standard mean difference (SMD) = –0.71; 95% confidence interval (95% CI) = –1.11 to –0.30; p = 0.0006), improved static balance with open eyes (SMD = –1.26; 95% CI = –1.83 to –0.69; p<0.0001) and closed eyes (SMD = –1.74; 95% CI = –2.36 to –1.12; p < 0.00001), and increased walking speed (SMD = 0.44; 95% CI = 0.05 to 0.84; p = 0.03), but did not improve results on the Timed Up and Go Test (SMD = –0.60; 95% CI=–1.22 to 0.03; p = 0.06).
Conclusion: Transcutaneous electrical nerve stimulation is associated with significantly reduced spasticity, increased static balance and walking speed, but has no influence on dynamic balance.
Key words: transcutaneous electrical nerve stimulation; TENS; stroke; spasticity; balance; meta-analysis.
Accepted June 20, 2017; Epub ahead of print Sep 1, 2017
J Rehabil Med 2017; 49: 00–00
Correspondence address: Shuqing Lin, No. 1111 Jiangnan Road, Ningbo, Zhejiang, 315000, China. E-mail: 185426748@qq.com
Stroke patients commonly experience spasticity resulting in decreased balance and significantly reduced quality of life (1–3). Decreased bal-ance becomes ubiquitous in patients with stroke and seriously reduces ability to perform activities of daily living (4–6), caused mainly by abnormal muscle tone, cognitive changes, decreased muscle power, limited range of motion, uncoordinated movements, and alterations in sensory integration (7, 8).
Transcutaneous electrical nerve stimulation (TENS) has been reported to effect pain control and sensory stimulation, increase muscle power and move-ment function, and decrease spasticity (9). TENS could thus be an important adjunctive therapy to improve functional ability and decrease spasticity in stroke patients (10). Previous studies have demonstrated that supplementation with TENS can significantly reduce spasticity, and improve balance and walking speed (11–13).
In contrast to this promising finding, however, some relevant randomized controlled trials (RCTs) have shown that TENS does not reduce spasticity and increase walking speed (14–16). Considering these inconsistent effects, we therefore conducted a systematic review and meta-analysis of randomized controlled trials (RCTs) to evaluate the influence of TENS on spasticity, balance, and walking speed of stroke patients.
This systematic review and meta-analysis was conducted according to the guidance of the Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) statement (17) and the Cochrane Handbook for Systematic Reviews of Interventions (18). All analyses were based on previous published studies, and thus no ethics approval or patient consent were required.
PubMed, Embase, Web of Science, EBSCO, and the Cochrane Library were systematically searched from inception to February 2017, with the following key words: transcutaneous electrical nerve stimulation or TENS, and stroke or hemiplegic. To include additional eligible studies, the reference lists of retrieved studies and relevant reviews were also hand-searched and the process above was performed repeatedly until no further article was identified. The inclusion criteria were as follows: (i) patients with stroke who were able to walk independently; (ii) patients underwent TENS or placebo TENS; and (iii) the study design was RCT.
The following information was extracted for the included RCTs: first author, publication year, sample size, baseline characteristics of patients, TENS intervention, control intervention, study design, MAS, Timed Up and Go (TUG) test, balance (open eyes), balance (closed eyes), and walking speed. The study author was contacted to acquire data when necessary.
The primary outcome was MAS. Secondary outcomes included TUG test, balance (open eyes), balance (closed eyes) and walking speed.
The Jadad Scale was used to evaluate the methodological quality of each RCT (19). This scale consists of 3 evaluation elements: randomization (0–2 points), blinding (0–2 points), and drop-outs and withdrawals (0–1 points). One point was allocated to each element mentioned in the article, and a further point was given if the methods of randomization and/or blinding were described appropriately and in detail. A point was deducted if methods of randomization and/or blinding were inappropriate, or drop-outs and withdrawals had not been recorded. The Jadad Scale score varied from 0 to 5 points. An article with Jadad Scale score ≤ 2 was considered to be of low quality. If the Jadad Scale score was ≥ 3, the study was considered to be of high quality (20).
Standard mean differences (SMD) with 95% confidence intervals (95% CIs) for continuous outcomes (MAS, Timed Up and Go test, balance (open eyes), balance (closed eyes), and walking speed) were used to estimate the pooled effects. All meta-analyses were performed using the random-effects models with DerSimonian and Laird weights. Heterogeneity was tested using the Cochran Q statistic (p < 0.1) and quantified with the I2 statistic, which described the variation in effect size that was attributable to heterogeneity across studies. An I2 value greater than 50% indicated significant heterogeneity. Sensitivity analysis or subgroup analysis was performed to detect the influence of a single study on the overall estimate via omitting 1 study in turn when necessary. Owing to the limited number (< 10) of included studies, publication bias was not assessed. p < 0.05 in 2-tailed tests was considered statistically significant. All statistical analyses were performed with Review Manager Version 5.3 (The Cochrane Collaboration, Software Update, Oxford, UK).
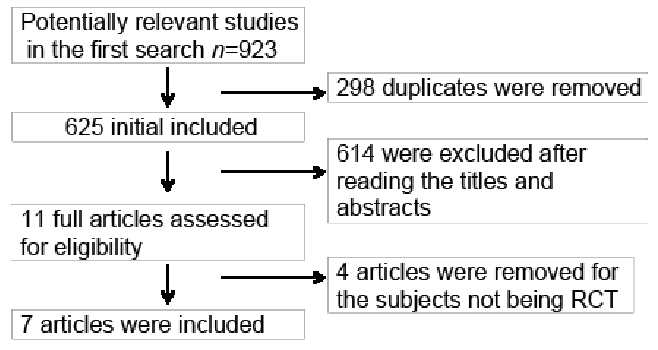
The flow chart for the selection process and detailed identification was presented in Fig. 1. A total of 923 publications was identified through the initial search of databases. Ultimately, 7 RCTs were included in the meta-analysis (11–16, 21).
Fig. 1. Flow diagram of study searching and selection process.
The baseline characteristics of the 7 eligible RCTs in the meta-analysis are summarized in Table I. The 7 studies were published between 1997 and 2014, and sample sizes ranged from 24 to 41 with a total of 214.
Table I. Characteristics of included studies
Post-stroke time varied from several days to several years. Among the 7 RCTs, 3 studies reported the MAS (11, 12, 16), 2 studies reported the Timed Up and Go test (12, 13), 1 study reported the balance (open eyes) and balance (closed eyes) (12), and 3 studies reported the walking speed (12, 14, 15). Jadad scores of the 7 included studies varied from 3 to 5, and all 7 studies were considered to be high-quality ones according to quality assessment.
The MAS was known as a subjective method to measure spasticity. In order to perform the MAS, the patient’s ankle was passively extended from maximal plantar flexion to the painless range and a score ranging from 0 to 4 (0, 1, 1+, 2, 3, and 4) was assigned: 0 indicated normal or very low muscle tone, and 4 indicated that passive extension was not possible. MAS was analysed with a random-effects model, the pooled estimate of 3 included RCTs suggested that TENS supplementation significantly alleviated spasticity as shown by reduced MAS compared with the control group (SMD = –0.71; 95% CI = –1.11 to –0.30; p = 0.0006), with no heterogeneity among the studies (I2= 0%, heterogeneity p = 0.78) (Fig. 2).
Fig. 2. Forest plot for the meta-analysis of modified Ashworth scale (MAS). 95% CI: 95% confidence interval.
No heterogeneity was observed among the included studies for the primary outcome (I2 = 0%). Thus, we did not perform sensitivity analysis by omitting 1 study in each turn to detect the source of heterogeneity.
Dynamic balance was evaluated through the TUG test, which measured the time required for a patient to stand up from a 46-cm high chair, then walk 3 m, and return to the chair. Three repeated measurements were required. Compared with a control group, TENS supplementation did not alter TUG test scores (SMD = –0.60; 95% CI = –1.22 to 0.03; p = 0.06; Fig. 3).
Fig. 3. Forest plot for the meta-analysis of Timed Up and Go (TUG) test. 95% CI: 95% confidence interval.
Static balance with open eyes or closed eyes included anterior posterior velocity and medial later velocity. A TENS group was found to significantly improve static balance with open eyes (SMD = –1.26; 95% CI = –1.83 to –0.69; p < 0.0001; Fig. 4) and closed eyes (SMD = –1.74; 95% CI = –2.36 to –1.12; p < 0.00001; Fig. 5), as well as walking speed (SMD = 0.44; 95% CI = 0.05 to 0.84; p = 0.03; Fig. 6).
Fig. 4. Forest plot for the meta-analysis of static balance (eyes open, mm/s). 95% CI: 95% confidence interval.
Fig. 5. Forest plot for the meta-analysis of static balance (eyes closed, mm/s). 95% CI: 95% confidence interval.
Fig. 6. Forest plot for the meta-analysis of walking speed (m/s). 95% CI: 95% confidence interval.
A recent meta-analysis pooling the results of 8 clinical studies revealed that electric stimulation was effective to improve gait speed in stroke patients. However, only 2 RCTs were included in the analysis. Also, this meta-analysis focused only on gait speed (22). The current meta-analysis involved 7 RCTs, and the results clearly suggest that TENS supplementation could significantly reduce spasticity, improve static balance and walking speed, but is not associated with a significant improvement in dynamic balance. Regarding the sensitivity analysis, there was no heterogeneity for the primary outcome despite different intensity, frequency of stimuli, and frequency of application. We did not omit one study in each turn of the analysis to detect the source of heterogeneity.
Previous studies have reported that TENS can decrease spasticity in patients with spinal cord injury (23) and chronic stroke (15), and reduce H-reflex size and spasticity in patients with hemiplegia (24). A combination of TENS and an exercise programme resulted in improved standing postural control, quadriceps and gastrocnemius maintenance, and somatosensory function in the lower extremity (25).
Spasticity was thought to account mainly for decreased balance in patients with stroke, multiple sclerosis, spinal cord injury, and traumatic brain injury. In addition, spasticity was found to trigger spastic movement disorder, slowed gait, disturbances in voluntary movement, and reduce passive and active range of motion, functional ability, and dynamic balance (26–28). This meta-analysis confirmed that TENS supplementation could significantly alleviate spasticity and improve static balance compared with placebo TENS.
Gait is a complex movement including balance, coordination, proprioception, and integrated harmony between joints and muscles (29). Sensory electrical stimulation applied to the Achilles tendon and gastrocnemius 6 times per week for one month, led to increased speed in stroke patients (21). Our meta-analysis also confirmed that TENS in combination with an exercise programme could significantly improve walking speed. In addition, one included study reported that TENS supplementation could also improve step length, and cadence in the affected leg during gait, as well as proprioception to each muscle (12). An asymmetrical gait pattern could result in decreased speed and balance, increased double stance, and short step length in most stroke patients (30).
Several limitations should be taken into account. Firstly, the analysis was based on only 7 RCTs, all with a relatively small sample size (n < 100). Overestimation of the treatment effect was more likely in smaller trials compared with larger samples. The post-stroke time ranged from several days to several years and the intensity, frequency of stimuli, and frequency of application were different in the included RCTs. Two RCTs involved 30 min of TENS (100 Hz, 200 µs, 2–3 times sensory threshold) per day, 5 days a week for 4 weeks (12, 16), 1 RCT involved 60 min of TENS (100 Hz, 200 µs, 2–3 times sensory threshold) per day, 5 days a week for 4 weeks (15), 1 RCT involved 60 min of TENS (100 Hz, 200 µs, 2–3 times sensory threshold) (11), 1 RCT involved TENS (100 Hz, 200 µs) per day, 5 days a week for 3 weeks (13), and 1 RCT involved TENS (20 Hz, 200 µs) (21). These 2 factors may have had an influence on the pooling results of this meta-analysis. The mechanisms mediating the impact of TENS on stroke remain elusive. Finally, some unpublished and missing data might biased the pooled effect.
In conclusion, TENS is associated with significantly reduced spasticity, and improved static balance and walking speed in stroke patients, but has no influence on dynamic balance. TENS is recommended for use in patients with stroke.
The authors declare no conflicts of interest.


 Click to show fullsize
Click to show fullsize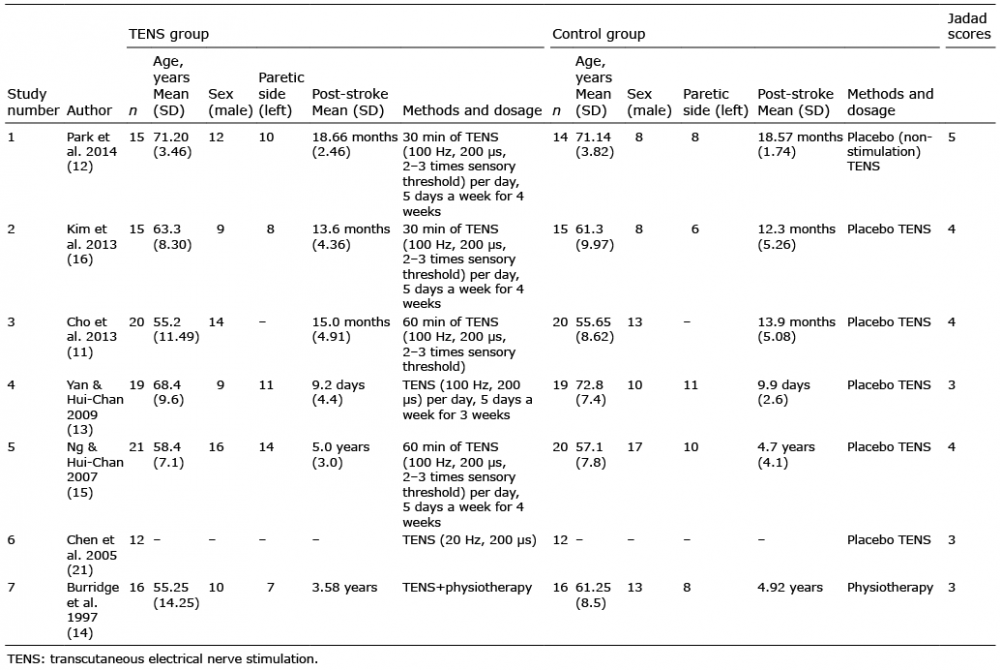 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize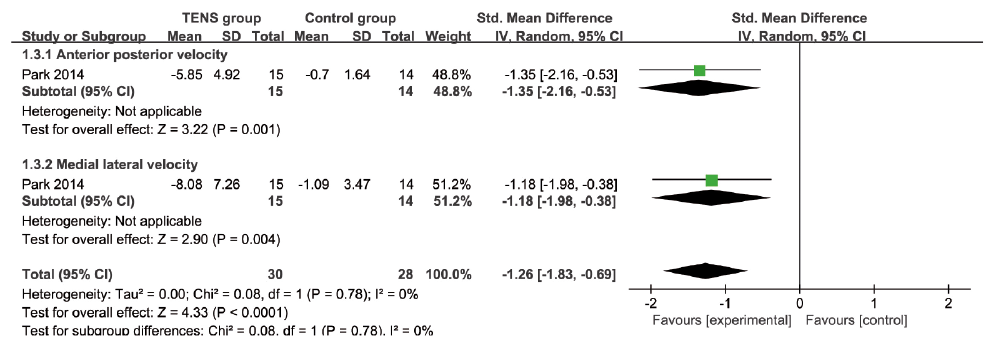 Click to show fullsize
Click to show fullsize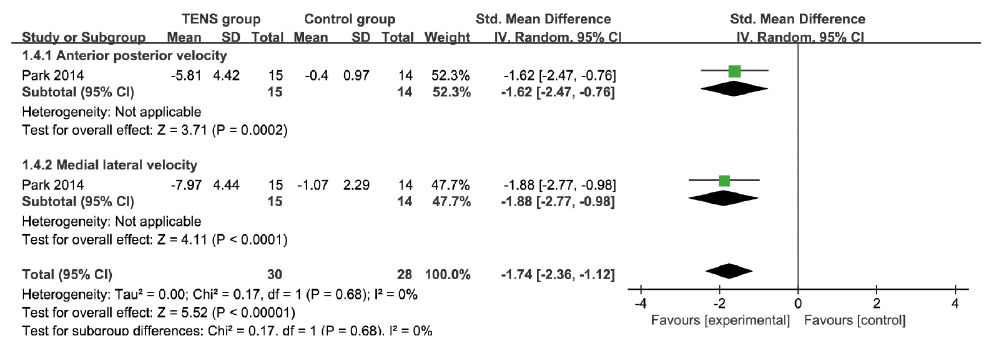 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize