
From the 1Department of Clinical Neuroscience and Rehabilitation, Institute of Neuroscience and Physiology, Sahlgrenska Academy, University of Gothenburg, Gothenburg, Sweden
Objective: Subarachnoid haemorrhage can lead to long-term disabilities. It is a major health issue for the patient and can affect work capacity. The aim of this study was to investigate working capacity after subarachnoid haemorrhage from a long-term perspective, using data from national sick leave records. In addition, factors associated with working capacity were analysed.
Design: A retrospective cohort study.
Subjects/patients: A consecutive total sample of 38 working-age participants with first-ever subarachnoid haemorrhage was included. Working capacity of the 30 participants not on early retirement prior to the subarachnoid haemorrhage was analysed.
Methods: Working capacity was defined as no longer being registered on sick leave or early retirement in the Social Insurance Agency and not being age retired or deceased.
Results: Regain of working capacity continued until 2.5 years post-subarachnoid haemorrhage and 73% of the participants were deemed to have working capacity. Functional independence at discharge from hospital, and higher responsiveness at admittance were the main factors associated with an earlier regain of working capacity.
Conclusion: Nearly three-quarters of subjects were deemed to have working capacity within 2.5 years post-subarachnoid haemorrhage with a non-self-reported outcome. This information will help to individualize rehabilitation for affected persons.
Key words: subarachnoid haemorrhage; stroke; return to work; health insurance; cohort studies.
Accepted Aug 8, 2017; Epub ahead of print Sep 1, 2017
J Rehabil Med 2017; 49: 00–00
Correspondence address: Emma Westerlind, Department of Clinical Neuroscience and Rehabilitation, Institute of Neuroscience and Physiology, Sahlgrenska Academy, University of Gothenburg, Gothenburg, Sweden. E-mail: westerlind.emma@gmail.com
Approximately 5% of all strokes globally are classified as subarachnoid haemorrhages (SAH) (1). A majority (85%) of non-traumatic SAH are caused by a ruptured aneurysm, 10% by non-aneurysmal perimesencephalic haemorrhage, with the remaining 5% having rarer causes (2). SAH accounted for 4.4% of stroke-related deaths in the USA in the period 1979–94 (3). The estimated risk of dying from an aneurysmal SAH before arrival at hospital or receiving treatment is 12% (4) and the estimated 1-year mortality is 15.6% (5). Furthermore, SAH accounts for 27.3% of years of potential life lost due to stroke in those aged <65 years (3). Cognitive impairment, as well as emotional problems, are frequently seen in SAH survivors and affect the persons’ health-related quality of life (6).
In 2008, approximately one-third of the total cost of stroke in high-income countries consists of indirect costs, due to productivity loss resulting from mortality and morbidity (7, 8). Since a substantial number of SAH occur in persons of working age, as shown in 2 Scandinavian studies with mean SAH onset age of 55 and 59 years (5, 9), SAH can result in major suffering and costs to individuals, as well as society if there is incomplete return to work (RTW). Two studies (Sweden and UK) both presented a RTW rate of approximately 50% 1 year post-SAH (10, 11). In another study with a 2–4-year follow-up in the Netherlands, 61% had some RTW but only 35% completely returned to their previous employment (12). All the studies above used self-reported RTW as an outcome measure. Persons who did RTW were more satisfied with life as a whole than those who did not (12).
The aim of this study was to investigate the characteristics of working capacity during a period of 6 years post-SAH and compare this working capacity rate with persons who had suffered an ischaemic stroke or intracerebral haemorrhage.
All patients with first ever non-traumatic SAH (International Classification of Diseases (ICD) code I60) were consecutively included in this study during an 18-month period, during 2009–2010. Inclusion criteria were: patients treated at a stroke unit, neurosurgical unit or intensive care unit at the Sahlgrenska University Hospital in Gothenburg, Sweden; living within 35 km of the hospital; and 18–63 years of age at the time of the SAH. The included participants are from the extended Stroke Arm Longitudinal Study at the University of Gothenburg (SALGOT) (13, 14).
Each of the participants with SAH were individually matched with 2 members of a control group. The control group consisted of participants from the Stroke Arm Longitudinal Study at the University of Gothenburg (SALGOT)-extended (13, 15) who had had an ischaemic stroke (ICD I63) or intracerebral haemorrhage (ICD I61) and participated in a previous study on RTW after stroke (16). The control group was matched 2:1 and in the matching process the variables were prioritized as follows: (i) functional outcome at discharge from hospital according to the modified Rankin Scale (mRS), age and sex, (ii) age, functional outcome at discharge from hospital (mRS) and sex.
The study followed the principles of the Declaration of Helsinki and was approved by the Regional Ethics Committee in Gothenburg in 2008. An amendment for the Social Insurance Agency was approved in 2015. According to the Swedish law regarding personal particulars data (personuppgiftslagen, Swedish law number SFS 1998: 204) no informed consent is needed to collect data from medical charts for clinical purposes and quality control.
From the medical charts, baseline data, such as sex, age, comorbidity, treatment, rehabilitation, complications and whether the SAH was caused by an aneurysm were collected. The Reaction Level Scale (RLS-85) was used to report responsiveness at time of arrival at the hospital and was converted into the Glasgow Coma Scale (GCS, scores 3–15, higher score is better) (17). The Hunt & Hess Stroke Scale data (H&H, scores 1–5, lower score is better) were collected and the patient’s disability at discharge from hospital was assessed with the modified Rankin Scale (mRS, scores 0–6, lower score is better).
Approximately 5 years post-SAH, the mortality register at the National Board of Health and Welfare in Sweden was used to determine the mortality rate and cause of death of participants in the current study. The Social Insurance Agency provided information about early retirement (sickness compensation) and sick leave (sickness benefit) one year prior to the SAH and number of days of sick leave or early retirement within 6 years post-SAH.
During the first 2 weeks of sick leave in Sweden, employers provide sick pay. Thereafter the Swedish Social Insurance Agency, which is a universal public authority, pays sickness benefit. In the RTW process, the Social Insurance Agency uses a step-by-step rehabilitation model to evaluate the person’s capacity to work, with more stringent criteria being applicable the longer someone is absent from work, e.g. after 180 days the person’s working capacity is evaluated against the entire labour market (18). Early retirement is a potential arrangement instead of sick leave for persons for whom RTW is probably not due to chronic sickness; however, RTW is still possible if someone has taken early retirement. The participants’ entry into the study period in the current study began at admittance to hospital with SAH symptoms. The participants who were in early retirement prior to the SAH were not included in the working capacity analyses. The study period was defined as the number of days registered on sick leave or early retirement post-SAH. The main outcome measure was deemed by the Social Insurance Agency to have working capacity. Having working capacity was defined as no longer being registered for sick leave or early retirement (neither full-time nor part-time) in the Swedish Social Insurance Agency and not leaving it within one year after turning 65 years of age (old-age retirement in Sweden) or within 1 month of dying.
Potential predictor variables for working capacity were age, sex, comorbidity potentially affecting working capacity, specialized rehabilitation, GCS score, mRS score, and sick leave prior to the SAH. Age was dichotomized into a younger (≤ 52 years old) and an older group (≥ 53 years old), divided at the median age of the SAH participants. Comorbidity potentially affecting working capacity was counted as existing if the participant had one of the following diagnoses prior to the SAH: myocardial infarction, diabetes, alcohol/drug abuse, mental illness, cancer, chronic obstructive pulmonary disease, rheumatic disease or other specific diseases. Specialized rehabilitation meant receiving specialized rehabilitation treatment at the Sahlgrenska University Hospital rehabilitation unit after the SAH, either as an inpatient or outpatient. The GCS was presented as mild (score 13–15) or moderate/severe (score 9–12/3–8) (19). The mRS was dichotomized into functional independency (score 0–2) and dependency (score 3–6) (20). Sick leave prior to the SAH included those who were on sick leave for at least 2 weeks in the last year before their SAH.
To compare groups and investigate potential differences the Fischer’s exact test and Mann–Whitney U test were used. Death before the event (deemed to have working capacity) was considered as a competing risk and were thus set at worst case scenario, meaning censored after the total follow-up time. Participants in old-age retirement were additionally censored at the time of the event. Time to the event was illustrated with Kaplan–Meier plots and the log-rank test was used to analyse potential difference in time to the event between different factors. When creating the Kaplan–Meier curves, death before the event and old-age retirement were reasons for censoring. Death before the event was considered to violate the non-informative censoring assumption. Therefore, it was treated with a worst-case scenario approach, which means that the participants who died before the event were censored at the end of follow-up instead of at the date of death. This will result in a more conservative estimate for deemed to have working capacity. Old-age retirement was censored at time of retirement, since it is not violating the non-informative censoring assumption. The data was processed and analysed in IBM SPSS 22. The level of significance was set at p ≤ 0.05.
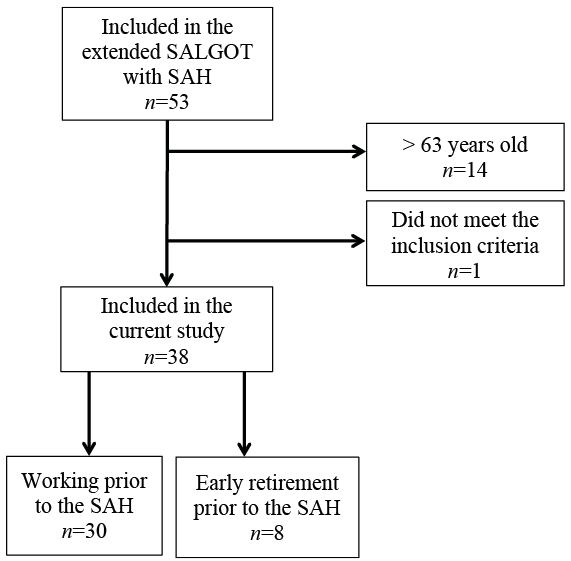
A total of 38 participants met the inclusion criteria (Fig. 1). Before the SAH, 8 participants had retired early, with pain-related diseases and cardiovascular diseases as the most common diagnoses.
Fig. 1. Study population flowchart. SALGOT: Stroke Arm Longitudinal Study at the University of Gothenburg; SAH: subarachnoid haemorrhage.
Of the total 38 participants, 65.8% were women and 34.2% men, as seen in Table I. The median age at time of the SAH was 52.5 years.
Table I. Baseline characteristics of the study population
Six participants of the 38 died before the end of follow-up, 5 of whom died within the first 2 weeks after SAH and 1 after just over 20 months post-SAH. All the deceased participants were women. There were no significant sex differences between the groups, in terms of GCS at SAH onset or mRS at discharge from hospital (p = 0.158 and 0.165, respectively).
The majority of the SAH were caused by an aneurysm. There were no significant differences in mRS group (independent or dependent at discharge) between the aneurysm and non-aneurysm groups (p = 0.296).
The control group consisted of 76 matched persons (59 with ischaemic stroke and 17 with intracerebral haemorrhage). The control group and the SAH group did not differ significantly in age (p = 0.962, with a maximum range of ± 10) or functional outcome at discharge from hospital (mRS) (p = 0.842, with a maximum range of ± 3) but the SAH group included significantly more women (p = 0.010). Fifteen (19.7%) persons in the control group had retired early prior to the stroke.
Of the 30 participants who had not retired early prior to the SAH, 22 (73.3%) were deemed to have working capacity, 5 (16.7%) were deceased, and 3 (10.0%) were retired early 6 years after SAH. No participants were still on sick leave.
The regain of working capacity continued until just over 30 months post-SAH (Fig. 2). The first quartile regained working capacity in the first 1.7 months (standard error (SE) 1.248) and the second quartile within 9.0 months (SE 8.734) post-SAH. The highest rate of persons deemed to have working capacity occurred within the first year post-SAH.
Fig. 2. Cumulative incidence of time to deemed to have working capacity after subarachnoid haemorrhage (SAH).
A similar pattern for time to regaining working capacity could be seen in the control group. At the end of the follow-up period, the proportion deemed to have working capacity in the control group was 77.0% compared with 73.3% in the SAH group (p = 0.796).
A faster regain of working capacity after SAH was associated with functional independency in the mRS (Fig. 3) (p < 0.0005), mild GCS score (Fig. 3) (p < 0.0005), male sex (p = 0.012) and having been assessed as not needing referral to specialized rehabilitation (p = 0.05). After excluding the participants who died before discharge (5 persons, all women) the time to deemed to have working capacity was no longer significantly different between male and female participants (p = 0.119). All participants with a mRS score of 0–2 at discharge from hospital were deemed to have working capacity. Furthermore, age groups, comorbidity, and sick leave prior to the SAH could not be statistically compared due to crossed curves, which indicate violation of the proportionality assumption.
Fig. 3. Cumulative incidence of time to deemed to have working capacity after subarachnoid haemorrhage. mRS: modified Rankin Scale; GCS: Glasgow Coma Scale.
The main findings of the present study were that 73% of participants who were of working age who had had a SAH were deemed to have working capacity. Participants continued to regain working capacity until 2.5 years post-SAH. Functional independence at discharge from hospital and higher responsiveness at admittance were the main characteristics associated with a faster regaining of working capacity. The time to participants being deemed to have working capacity after a SAH compared with ischaemic stroke and intracerebral haemorrhage were relatively similar. RTW is an important factor to consider after a SAH. Previous research has shown that persons with SAH were least satisfied with their vocational situation at follow-up (12) and no-RTW is associated with a poor quality of life (11, 21).
The current study presents a relatively high rate of 73% of subjects who were deemed to have working capacity compared with 61% in a study in the Netherlands (12), 48% in the UK (11), and 56% in the USA (22). All the above-mentioned studies had a self-reporting outcome measure, but a variable follow-up time, with the majority shorter than the current study. The differences in the RTW rate may be due to differences in study design. The current study presents an outcome measure from national records instead of self-reported RTW/working capacity, which enables information about the precise number of days until the participant is deemed to have working capacity and eliminates the risk of recall bias. Furthermore, the long follow-up time could result in a higher deemed to have working capacity rate since the participants continued to regain working capacity up to 2.5 years post-SAH. For instance, cognitive impairment is most common the first 3 months after SAH, but a review has shown that it can persist much longer and therefore explain a late regain of working capacity (23). A different Swedish study presented a RTW rate of 52% after SAH (10), and this difference in RTW rate compared with the current study may be explained by the shorter follow-up time (1 year) and self-reported outcome. Furthermore, different sick-leave systems and culture between countries presumably have an impact on RTW after sickness. In Sweden, healthcare and rehabilitation is funded by the tax payer and the Swedish Social Insurance Agency provides financial compensation to people with all kinds of occupations when they are sick. Employers can receive wage subsidies if they hire people with a disability (24), which may increase the possibility of RTW.
There was a slightly, though not statistically significant, higher rate of subjects deemed to have working capacity in the control group including both ischaemic stroke and intracerebral haemorrhage compared with the SAH group. A Danish study (25) on RTW after stroke showed a RTW rate of 60% after a SAH, 64% after an ischaemic stroke and 43% after an intracerebral haemorrhage, and a significantly lower odds ratio (OR ) of RTW in SAH (OR 0.79) and intracerebral haemorrhage (OR 0.39) compared with ischaemic stroke. A study conducted in the USA has shown that SAH has a higher mortality rate than ischemic stroke or intracerebral haemorrhage, which may partially explain the lower RTW rate; however, these differences in mortality between stroke types appear to have decreased between 1989 and 2009.
The participants consisted of approximately two-thirds women, which is concordant with the SAH population in previous research (27). In the current study, persons with all different types of SAH were included (i.e. aneurysm, perimesencephalic haemorrhage and unknown source of bleeding). Previous research has focused mainly on aneurysmal SAH (5, 9, 11, 12). Furthermore, the majority of participants had a mild GCS score and were functionally independent at discharge, in line with previous research (12). The severity of the SAH (at admission and discharge) was associated with working capacity. Higher mRS score have previously been shown to associate with failure to RTW. The impact of disability varies with the type of occupation and the content of the work performed. Factors that have previously been shown to be associated with RTW are, for instance, self-rated impairment of planning and reasoning, and the SAH victim’s partner’s rating of sensory and motor impairment (28). The current study presented a significantly more rapid regaining of working capacity for men than for women. However, when the participants who died during follow-up were excluded there was no longer a significant difference in sex. This was because only women died during the follow-up period. A higher mortality rate among women after SAH has been shown previously (26). Previous research also supports the notion that there is no sex difference for RTW (22). In the current study, there was a faster regaining of working capacity among the participants who did not receive specialized rehabilitation efforts. This was probably due to the selection of participants for rehabilitation, with the most severely impaired participants receiving the rehabilitation. Another Swedish study has shown similar results in a stroke population, with treatment in a rehabilitation ward unit as an unfavourable factor for RTW (29). An interventional study, however, has reported that early mobilization and rehabilitation increases the probability of good functional outcome (30).
The small sample size limits the generalizability of the study. Regression analyses could not be used to investigate predictor variables for working capacity due to the modest number of participants. Furthermore, using data from the Social Insurance Agency and their estimation of people’s working capacity as outcome limits the comparison with previous research. RTW is the most commonly used outcome in previous studies, and it is difficult to compare this outcome with the one used in the current study “deemed to have working capacity”. However, RTW is also defined differently in different studies with different methods. The current study used GCS and mRS to assess the severity of the SAH. It is a limitation that different kinds of impairment were not presented. For instance, cognitive function has previously been associated with RTW after SAH (10, 31, 32) and it is likely that cognition is a relatively decisive factor for working capacity.
The current study shows a high rate of participants deemed to have working capacity after SAH compared with previous research, and participants continued to regain working capacity during a longer time period than some of the previous follow-up times. The responsiveness at admittance and functional dependency at discharge were associated with time to regaining working capacity. RTW after a SAH is important for the affected person as well as for society generally, and this research can contribute to more individualized and accurate rehabilitation efforts.
This work was supported in part by the Swedish Heart and Lung Foundation, the Swedish Brain Foundation and Promobilia.
The authors declare no conflicts of interests.


 Click to show fullsize
Click to show fullsize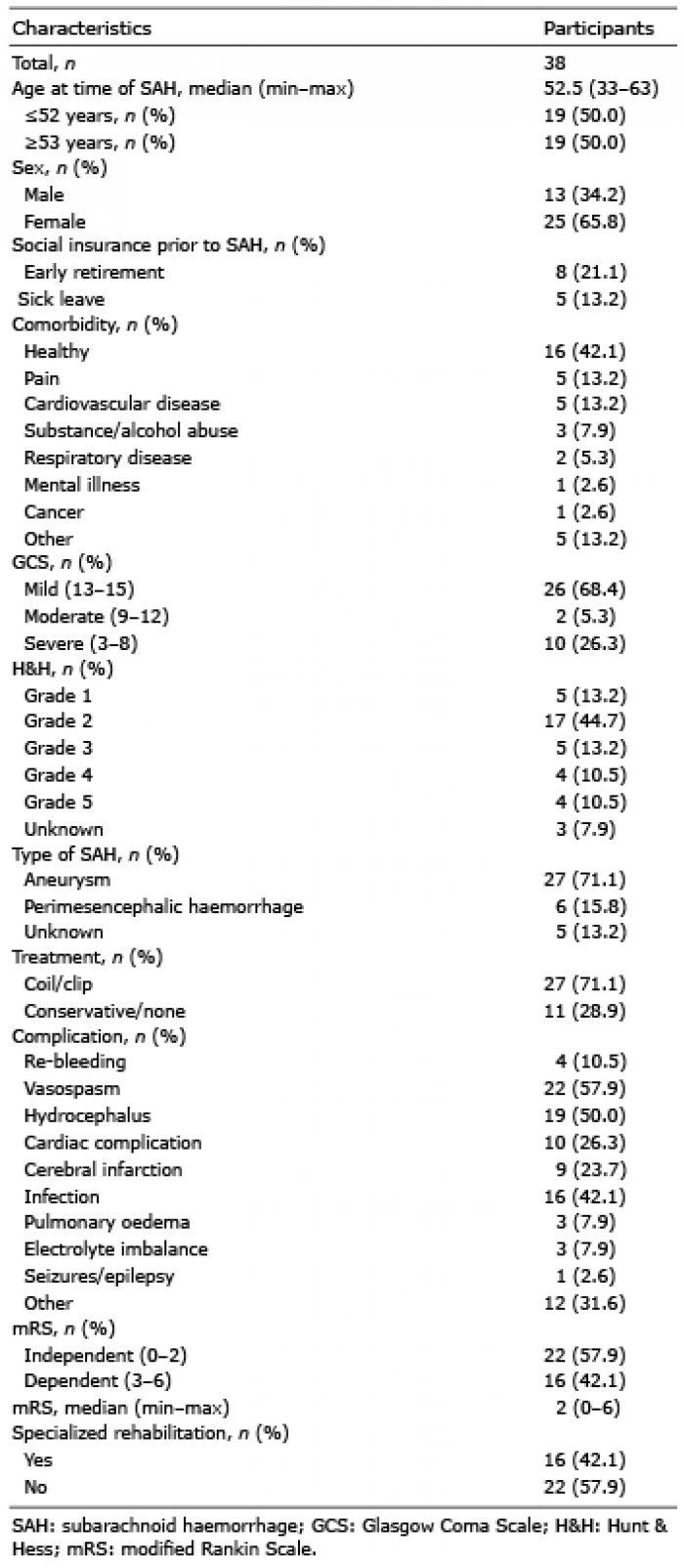 Click to show fullsize
Click to show fullsize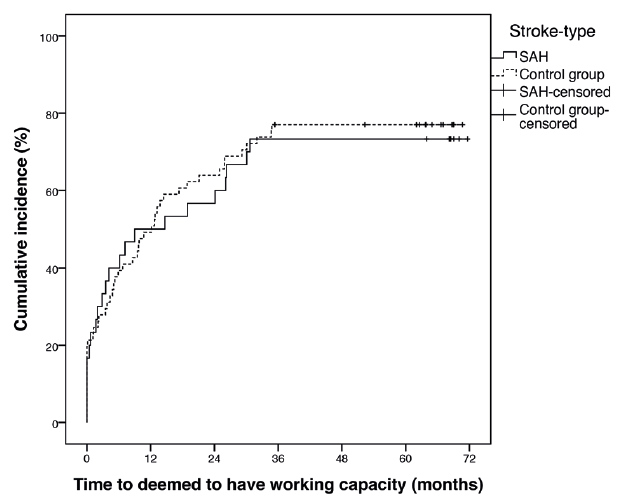 Click to show fullsize
Click to show fullsize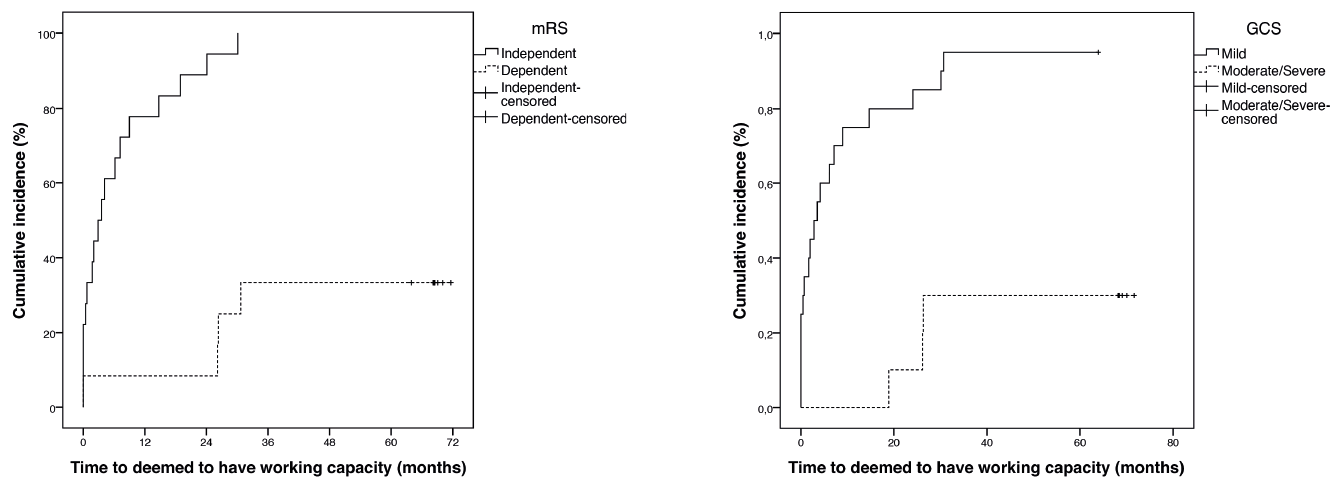 Click to show fullsize
Click to show fullsize