
From the 1Center for Rehabilitation Sciences Research and 2Department of Rehabilitation, F Edward Hebert School of Medicine, Uniformed Services University of the Health Sciences, Bethesda, MD, USA
Objective: To explore how the social context of the clinic influenced the way former patients with lower limb loss in the Military Advanced Training Center at Walter Reed National Military Medical Center evaluated their outcomes.
Design: Cross-sectional phenomenological-based interviews and observations.
Patients: Twenty individuals with lower limb amputation were recruited from a multidisciplinary military treatment programme for patients with lower-extremity traumatic limb-loss injured in Afghanistan or Iraq.
Methods: Lightly structured interviews were conducted either in person or over the telephone with former patients and clinical care-providers. Where possible, observation was conducted in conjunction with the interviews. The research team used content analysis of the data, consistent with ethnographic methods.
Results: Analysis of the therapeutic effect of social relationships developed in the clinical rehabilitation programme identified 3 areas of significance: enduring relationships with key care-providers, access to treatment team by patients, and peer support among patients.
Conclusion: The social component of service delivery influences patients’ outcomes from clinical care. These results could be translated across healthcare settings to improve patient outcomes.
Key words: amputation; autonomy; lower extremity; peer support; rehabilitation; social organization.
Accepted Aug 18, 2017; Epub ahead of print Dec 5, 2017
J Rehabil Med 2018; 50: 87–94
Correspondence address: Seth Messinger, Center for Rehabilitation Sciences Research, Uniformed Services University of the Health Sciences, 20814 Bethesda, USA. E-mail: seth.messinger.ctr@usuhs.edu
In order to determine in what ways the social relationships developed in a clinical programme are therapeutic, retrospective narratives from former patients were studied to evaluate their impressions of the effectiveness of the US Armed Forces Amputee Patient Care Program (APCP). This programme provides rehabilitative care to US military service members who have sustained traumatic amputations during deployment to Iraq or Afghanistan. Organized in 2001 at Walter Reed National Military Medical Center (formerly the Walter Reed Army Medical Center), the multi-and interdisciplinary rehabilitation programme receives military patients from conflict zones who have been transported through Germany to the USA (1, 2). After being treated on inpatient medical and surgical units, patients are discharged to an outpatient amputee patient care programme (3, 4), which utilizes a delivery of care model that seeks to improve patient physical functioning while also addressing other critical healthcare, social and psychological needs, including planning for life after injury (5, 6). The overall goal of the programme is to provide a setting in which injured service members can recover to as close an approximation of their pre-injury functioning as possible (7).
While the primary focus of the APCP is to work with patients to return them to a high level of physical functioning, in this paper we argue that patients also benefit from substantial psychological and social support derived from the programme persists after they leave Walter Reed. This unanticipated effect of the programme was made manifest through 3 features of the programme’s social environment. Our work builds on a recent paper by Dunne and co-authors (8) that examines life after limb loss through users’ relationships with their assistive devices. These authors found that users attached meaning to their assistive devices beyond physical functioning. In addition, our work has been informed by Suarez and colleagues on how persons with traumatic spinal cord injury regain a sense of personal health and wellbeing (9). We have reached similar conclusions to these researchers regarding how former patients assign value to less overt aspects of rehabilitation programming. In this paper these are the meanings and psychological support embedded in the social and organizational aspects of the programmes in which participants were enrolled.
Between October 2001 and March 2017 almost 1,500 US military service members have sustained conflict-related lower-extremity amputations. Life-saving techniques and technologies used at the site of injury have led to an increased rate of survivability from once-fatal wounds (10–12). While most injured service members to-date are men (over 98% of the injured population), there are also 21 female service members with these injuries. Ninety-four of the nearly 1,500 service members have upper-limb loss in addition to lower-extremity amputations.
In the majority of explosive blast cases, injury results from a combination of the blast wave, fragment penetration and rapid bodily displacement. Compounding these immediate injuries to the extremities, blast injuries can, over time, lead to further tissue loss as well as infections in the residual limb, intact limbs, and other parts of the body (5, 13). There is also the potential for extensive nerve damage, with almost one-third of Walter Reed’s patients having nerve lesions and damage resulting in neuropathic pain and various levels of limited function (13, 14). Heterotopic ossification, uncomfortable bone formation at the site of amputation, is a common post-operative comorbidity associated with lower-limb amputations (5). Finally, almost one-quarter of patients with trauma-related amputation reported severe ongoing problems with their residual limbs, including phantom limb pain, wounds and sores, all of which can be a persistent problem with a significant negative impact on individuals’ functional outcomes and overall quality of life (15, 16).
In order to address these challenges of living with lower limb amputation (8, 16, 17) the programme at Walter Reed has invested heavily in both technology and care delivery support so as to aid in meeting the goal of restoring patients to a close approximation of pre-injury physical functioning (7). These technologies run the gamut from mechanically sophisticated prosthetic limbs (18) to the use of complex gait analysis tools, including the Computer-Assisted Rehabilitation Environment (CAREN) system (19), imaging systems to create three-dimensional models of residual limbs for prosthetic fitting, as well as specialized gym equipment for adaptive athletics. One outcome from the rehabilitation programme that underscores the impressive physical functioning outcomes it achieves is that more than 270 service members have been able to return to duty and more than 50 to redeploy to Iraq or Afghanistan after suffering conflict-related injuries1.
Although the investment in these resources has been high, there have been few outcome studies involving military patients with limb loss. One early study of patients with upper- and lower-extremity limb loss investigated reasons why patients may or may not incorporate their prosthetic devices into their daily routines (20). In that study, factors external to the rehabilitation programme, such as issues of broken trust associated with the injury or afterwards, were seen as having a greater influence over the extent to which patients adhered to their rehabilitation programme and adopted their prosthetics into their everyday lives. Other studies have examined rates of return to duty (21, 22) the experience of female veterans with limb-loss (23), ongoing work on life after injury as former patients navigate community living (24, 25), and, as mentioned above, the significance and meaning of assistive devices in the lives of individuals with lower-extremity amputations (8).
Through a close examination of how 20 former patients with lower-limb amputation assess their outcomes, this paper seeks to strengthen our general understanding of what kinds of outcomes are experienced by service members after their recovery in the clinical settings at Walter Reed, and to explore more particularly the influence of the social context of the clinical programme on how former patients evaluated their outcomes after their recovery (26, 27).
In 2015 the Center for Rehabilitation Sciences Research, Bethesd, MD, USA, launched a qualitative project to investigate how former patients from the US Armed Forces APCP were experiencing life in the community. The data for this study was collected using lightly structured observations and interviews. As part of this effort, an interview guide grounded in an interpretive phenomenological approach (28) was developed that explored different topics associated with how patients experience their recovery from injury and, more generally, with how former patients viewed the influence that the rehabilitation programme has had in their current lives. Eight interviews were conducted in person with former patients, with opportunities to suspend the formal part of the interview in order to participate and observe the individual in their home or community settings. Observations were used to develop a sense of the daily routine of former patients in their home communities, and were triangulated with the interview data. When face-to-face observations and interviews were impossible interviews were conducted over the telephone. Sunderland (29) points out that phone use (and by extension social media) are important means by which individuals communicate and to which they make meaning from their experience. These tele-technologies allow former participants to maintain social links with each other (after they have left the rehabilitation programme and moved around the country) and with key clinical providers at Walter Reed.
In addition, a small group of clinicians (particularly occupational and physical therapists) were interviewed in order to understand the influence of clinical work from the perspective of care-providers. All interviews were digitally audio-recorded and transcribed by a member of the research team. The transcription was checked against the audio file by a member of the research team who had not conducted or transcribed the interview.
For this sub-study a sample of 20 participants with major lower-limb amputation (19 men and 1 woman) who were at least 12 months past their last residential rehabilitation stay were selected. All participants had been injured while serving on active duty in the US military in either Afghanistan or Iraq. Participants ranged in age from mid-20s to early 40s. All participants relied on their prosthetic limb(s) for at least part of the day and used a wheelchair at other times. Table I shows the distribution of amputation levels among the 20 participants.
Table I. Distribution of amputation level (n = 20)
Participants were recruited using a convenience strategy that relied on a database managed by the Walter Reed APCP. Flyers were distributed through a mailing list and participants were enrolled as they responded. Efforts were made through the use of recruiting flyers to target under-represented groups, such as people of colour, women, and officers.
All personal identity information was changed through the use of code numbers, pseudonyms, and other efforts to obscure military rank or other features that could be used to compromise the confidentiality requirements of the Walter Reed National Military Medical Center and the Uniformed Services University of the Health Sciences Institutional Review Boards.
Content analysis was used to identify patterns among the themes and topics in the interview data (30, 31). The research team began the analysis by conducting multiple readings of field note data (drawn from observations at Walter Reed and in the community) and the interview transcripts to familiarize themselves with the data. Interview transcripts from patients and clinicians, and field note data, were then open coded and the initial codes were explored for key themes and topics. The research team then reviewed emergent themes, and alternative understandings were discussed. Alternative interpretations were tested against the data, and themes that were more strongly supported by the data were incorporated in the final analysis. While our systematic coding procedures help to support our interpretations of the data, the ultimate validity of the data must be judged within the wider context of the rich descriptions offered (32).
The results indicate that the social relations enfolded within the rehabilitation programme created durable psychological supports that former patients relied on after leaving Walter Reed and moving into their communities. Although the programme clinicians and leaders emphasized physical functioning outcomes, this research shows that, after the physical functioning gains have faded, the psychological supports remain durable. The impact of these factors loomed large in the year(s) after leaving care when the novelty of access to new devices had, to some extent, diminished. Three programme features emerged as being particularly important to building and/or reinforcing these psychological supports: daily access to key care-providers, on demand access to the entire clinical treatment team, and recovering with peers.
Former patients look back on the atmosphere of the physical and occupational therapy clinics as having been instrumental in how they perceive their continued success, a term that took on varied meanings in light of each participant’s own experiences. Participants used “success” talk when using their past accomplishments as a measure to describe their overall quality of life. For example, patients with lower-extremity limb loss are all taught and coached to walk on prosthetic limbs. The goal is to enable them first to walk with crutches and canes, and ultimately to walk unassisted. Patients are then encouraged to learn to run, swim, cycle, etc. For some patients there is reluctance or resistance to achieving these goals (26), and for others walking without canes may not be attainable. However, constant encouragement from clinicians helped most participants to reach the limits of their capacities. These efforts, and the accomplishments that often come with them, remain powerful sources of strength that former patients can draw on even after running has been eliminated from their repertoire of personal goals.
Diego, a research participant in his 30s with bilateral transfemoral amputations caused by injuries in Iraq in 2006, provides a good example of this kind of success talk. He describes the important legacy that sports training in the clinic, such as running or wheelchair basketball, currently plays in his life. Since leaving the rehabilitation programme in 2008 he has remained married and continues to work for the federal government. He reported that he had gained a considerable amount of weight since leaving the rehabilitation programme, and no longer participates in physical activity beyond family-focused activities, such as walks and hikes. Nonetheless, he still viewed the coaching he received from his physical therapist to push himself to the limits of his physical abilities as critical to giving him a sense of a future.
I feel lucky about the program. I absolutely feel that her [his physical therapist] attitude there helped me to get through my injuries. I would not want her to see me now, I probably am too out of shape, too heavy [laughing], to run, or to want to run. But I think without it I wouldn’t have made it so far.
Another former patient, Mark, who was not particularly interested in the physical emphasis and sports-oriented nature of the programme during his time as a patient, credits the programme with the confidence that he understands as being the foundation for his current successes. Here Mark, who was injured in Iraq and was recovering from bilateral transfemoral amputations, describes being alternately engaged with the programme and deeply depressed and withdrawn. As he reports,
I was really angry about my injury, .... I don’t know if you remember, but I was really angry a lot of the time.
Mark describes a series of different kinds of low points, which were mitigated through the emotionally supportive relationship he developed with his physical therapist.
I wouldn’t really do much more than the minimum. I remember not going on trips, not hanging out, not being particularly nice to others, But I talked to [name redacted] and, though she kept pushing me, she was really comforting.
Her work with Mark helped to give him a foundation that he drew upon after leaving the programme.
But after I got married [towards the end of his time in the programme] and finally got out I realized how much she [his physical therapist] had helped. I ended up going to college and I was doing well. I don’t know, something happened, I started thinking back to Walter Reed and it just kind of hit me that they really fixed me up. I mean I had great endurance from all the walking and hand cycling, and I could do a lot of stuff with my prosthetics. I just felt like I had confidence.
Supporting the physical and occupational therapists are recreational therapists and representatives from adaptive sport and leisure activities, including the creative arts (e.g. expressive writing, visual arts, performing arts, etc.). All of these individuals help to emphasize and embody the physical, psychological and emotional goals of the programme. Riley, who continues to struggle with lingering health issues associated with unilateral transfemoral amputation, is one of the few former patients who has neither attended school nor worked for any longer than brief periods. Nonetheless, the fact that he lives independently plays an important role in his sense of having a successful outcome. He echoes this sense that the caring and support he received from physical and occupational therapists who had got to know him during his recovery helped him to maintain his confidence in himself.
The folks here [this conversation was recorded during one of the Riley’s return visits to Walter Reed] got me out of bed and up on my feet. They did everything for me; they found an internship in auto sales when I wanted to explore that. Whatever I wanted or needed they either did, or tried like hell to do.
The emotional support that participants remember drawing on during their time as patients were important elements of their recovery. The longer term relationships with key clinicians (usually physical or occupational therapists) presented the critical opportunity for a break from maintaining a military bearing during the rehabilitation process. As a former patient explained,
It’s hard to stop being the bad-ass Marine, so it’s nice to have someone that you can talk to quietly who isn’t going to call you a [wimp].
Having regular access to the full treatment team has significant benefits for patients and clinicians alike. In the amputee programme at Walter Reed, the weekly meeting of the “amputee clinic” brought together rehabilitation medicine physicians, surgeons, occupational and physical therapists, prosthetists, social workers and others on an as-needed basis, providing the opportunity for each outpatient in the APCP to meet with his or her entire treatment team to address their weekly needs. Patients noted the importance of this meeting in helping them to instantiate a sense of autonomy and control over their course of treatment. For example, in these meetings patients were treated as a critical member of the treatment team, and as the single person who had the pre-eminent perspective on the progress of treatment (cf. 33). Chad, a soldier injured in Iraq, with a unilateral transfemoral amputation, described his recollection of how seriously his treatment team took his ideas for his own care.
In one of the meetings that we had on Wednesdays I remember that I said I wanted to improve my running. The docs and my PT [physical therapist] talked about new exercises I would need to try and the prosthetist who was there described different prosthesis configurations that could be assembled. By the time I left the meeting I had a whole new program that started Thursday [the following day] and the prosthetics folks had the prescription they would need to get started on getting me the leg. It was always like that, you could talk to everyone once a week and you knew how you were doing.
Participants also remembered these meetings as opportunities to learn more about troubles or challenges they were facing that might be more opaque. For example the psychological or neurological after-effects of their injury experience could be discussed and ways to manage problems associated with troubled sleep, low mood, or family contact could be explored in an atmosphere that patients recalled as being free of judgment. Treating psychological injuries is a high priority for clinicians in military medicine, but there is also recognition of the stigma that patients attach to psychological diagnoses. Lawrence, an army officer with bilateral transfemoral amputations following an explosion in Iraq described being able to talk about “weird experiences that didn’t fit” during one of these sessions.
I was there for like a year, or maybe a year and 3 months. I remember that I had a lot of trouble sleeping and headaches, bad dreams and stuff like that. I remember spending time in a lot of those clinic meetings talking about my meds, and experimenting with different combinations. There was a lot of time talking about whether I wanted to talk to a psychologist. I never [wanted to], so they kept tinkering with my various prescriptions and eventually it worked. Maybe I just got a bit better, I don’t know. But I remember how they let me make the decisions; they didn’t try to force one thing or another on me.
Clinicians also found this approach valuable. The weekly clinic sessions were broken into 2 parts: in the first part, the clinical team discussed the patient’s progress and came to some decisions about medications and clinical goals. The second part of the session started with the patient being invited to participate in the meeting. This scheduling allowed time for each member of the clinical team to get up to date on medication changes or healthcare needs, while saving critical time for the patient to introduce new topics of discussion that were of particular concern. A physical therapist explained:
It’s so much quicker to have everyone in the room with the patient. We can go over what changes are happening with their meds, or talk about the consequences of an upcoming procedure on their treatment or therapy. It’s like having a mini-panel or case conference with your whole patient load each week.
The most significant after-effect of this part of the clinical programme was to reinforce for patients that they had both autonomy and agency with regard to the unfolding of their rehabilitative care, which they relied on in their lives after the hospital. As these patients left the hospital programme and started receiving healthcare at Veterans Affairs (VA) hospitals or from other providers they described drawing on these experiences with their care-providers to set up programmes and systems in their new communities. Whether they were able to fully affect a change in their ongoing treatment was not the critical factor in this equation. What was more important was a patient’s sense that they did have a say, and that they could continue to advocate for themselves within what could often be a relatively faceless bureaucracy. As one patient recalled:
Sometimes you can get the docs [at a local VA hospital] to do things differently if you kind of advocate for yourself. Sometimes it doesn’t work. I can get my prosthetic worked on in the community, for some reason the VA still says they have to make the brace I wear on my other leg. Win some, lose some.
Peers are an important element in how former patients remember their time in the rehabilitation programme at Walter Reed. The benefit of recovering alongside their peers is often instantiated by how it changes patient’s experience of time. Being with other military patients creates a transitional time that participants said they valued as they shifted from the immediacy of their deployment experiences to the longer term demands of recovery and community reintegration (27). In addition, sharing the clinical space with patients who had arrived earlier allowed participants to visualize a living time-line of their proposed recovery (cf. 34). For example, Colin, who had a transtibial amputation caused by an injury sustained in Iraq, spoke about his first few days as an outpatient. Here he describes how important a role peers can play.
The most important thing for me was [gaining] perspective in terms of helping and accelerating [my] mental healing process. At first I was like ‘holy crap my leg’s off and its not going to grow back.’ It really helped me being surrounded by all these guys, even if at first it was a little depressing – because you’re like ‘wow, this guy has half an arm, and that’s all he has left.’ Once you get past that and start interacting with them then you realize they are not any different – they might be physically injured but they’re strong mentally and they’re a lot of fun to be around.
During his recovery period, which lasted well over 12 months, Colin was able to learn what he could expect in his own rehabilitation from watching and interacting with his peers. He was also in a position to be a guide to newly injured service members who had come in during the weeks and months after his injury.
I’d be working out on a mat or just standing in my prosthetic [leg] working on balance and see a guy walking between parallel bars or taking some jogging steps and I’d always pester my PT [name redacted] ‘when can I do that, I want to do that?’ As I got stronger and I could walk on my leg I’d go up to [Walter Reed Army Medical Center inpatient ward] 57 and talk to new guys and try to cheer them up or give them some idea of what to expect.
For most former patients remembering the social intensity of their rehabilitation programme is an important element in their narratives of recovery. The participants in our study do not all necessarily maintain ties with their former peers, but nearly all of them point to other patients as being key to their own recovery from both the physical and psychological consequences of their injury. Robert Sanderson explained:
It was good not having to explain or talk too much about things. If you couldn’t sleep because of nightmares, or you couldn’t really wake up because of the meds you didn’t have to say much [to the other patients]. They just understood or maybe they would share a trick they used that helped them. Either way it felt really good to have that understanding.
Competition was another important consequence of the social world of the rehabilitation programme (35). Patients encouraged each other, but also took pleasure in accomplishing goals and in exceeding one another’s accomplishments. Clinicians abetted this by posting accomplishments on the walls. For example, if a patient with lower-extremity amputations walked the track for a mile or more, that accomplishment would then be celebrated in a leaflet posted on the wall. When someone went the same distance or farther a new leaflet would replace the earlier one. Aaron, who had lost parts of both of his legs, one above the knee and the other below the knee, commented on the role that competition played in the clinic.
It felt good to be back in that kind of environment. Even if [we] don’t make a big deal of competing, [the patients] keep an eye out on what others are doing or can do. That happened in the PT clinic all the time too. I’d be wondering ‘how far can he walk’ or ‘what do I have to do to be able to run like that.’ Seeing how others were doing was a huge motivator.”
As part of the competitive environment there was also a certain amount of teasing and “trash-talk” that functioned as a way for patients to encourage one another to not “slack off” during their workouts. One patient, who stood on a stair step machine without moving for a few moments, was cheered on with sarcastic comments like “look at him go!” His retort was that he was responding to a text from his wife, but shortly thereafter he started climbing the treadmill stairs. This kind of teasing was nuanced around the patients’ informed sense of the ebb and flow of pain and tiredness that afflicted them. Jerry, who had bilateral transfemoral amputations, recalls how he and his peers became experts in pain.
If someone was in a lot of pain it was obvious and that guy got a break. I mean we would know, right? We all were experts about pain. But if someone was just kind of leaning on the machine or not doing much we’d talk shit to them. It wasn’t planned; it’s just that guys would always rag on guys who were being lazy. I worked hard to avoid [having] that [directed at me].
At the start of the study it was anticipated that the participants would attribute their self-described successful outcomes to their access to highly sophisticated assistive technologies (36–39). In part this expectation was related to the central role that assistive technologies play in the programme (7). However, what the results of this research demonstrate is that, while assistive technology plays a role in recovery among former patients of Walter Reed, the social dimensions of the clinic plays an even more significant role in how patients evaluate the success of their recovery.
The social context of clinical work is an important location to explore wider vistas of therapeutic impact, particularly on durable gains in social and psychological support. This approach has been used fruitfully in care settings that treat both physical injury and disease (34), military injury (40), psychiatric disorder (33, 41), and substance-dependence treatment (42). In these studies, the social component of clinical organization was an important element in understanding both the delivery of care and the success or failure of the interventions. Where our work is somewhat distinct is that we have identified 3 specific elements of the social context of the clinical programme in the APCP at Walter Reed that we argue can be formally organized and are translatable into different clinical settings across treatment programmes.
Throughout this paper, the 3 translatable features are: the durable key relationships between patients and service-providers; patient access to the entire treatment team on a regular basis; and recovery alongside peers with similar illnesses/injuries. One of the advantages of these 3 features is that compared with the heavy financial investment in biotechnology associated with the Walter Reed programme these are relatively low cost given that they are part of the environment. For this reason we argue that they are applicable to both military and civilian healthcare environments. While many civilian and military inpatient stays are relatively brief, outpatient programmes often hold patients in their care for longer periods of time. This is the case for substance dependence treatment with its 28-day detoxification programmes and lengthier rehabilitation programmes, recovery from physical injury, such as amputation or spinal cord injury, day hospital care for patients with psychiatric disorders, as well as the periods in which oncology patients receive radiological or chemical therapies. In all these settings we would argue that relationships with key providers, provision of regular access to a patient’s whole treatment team, and recovering alongside similarly afflicted peers offers therapeutic benefits, such as an increased sense of autonomy and respect, that have continuing positive effects long after the immediate treatment experience is over.
Close, enduring relationships with clinicians, especially the physical and occupational therapists, played an important role in the narratives of former patients as they reflected on the way that the rehabilitation programme influenced their current situations. In the narratives we collected from former patients, physical and occupational therapists were represented in 2 ways. Firstly, they were seen as motivating and supportive “coaches,” and in this way symbolized the sports and athletics approach of the programme. Secondly, the civilian status of the majority of physical and occupational therapists meant that they occupied a safe space in which patients could share anxieties and concerns without worrying about any personal or professional consequences. Daily access to these “coaches”, in both a physical and emotional sense, ensured that, beyond the intense physicality of the clinic, patients knew where to go when seeking motivation or searching for an opportunity to be more vulnerable. Furthermore, as we will see in the discussion about routine access to the entire treatment team, this kind of sustained contact contributes to continuity of care by allowing both care-provider and patient to develop a shared narrative and timeline of recovery (34).
The results of this research also demonstrated that routine access to the entire treatment team was important in building confidence among participants as well as encouraging them to be self-advocates. In other longer-term healthcare situations the opportunity to address anxiety and foster confidence are not made so readily clear. The compartmentalization of medical care remains an issue facing patients in the USA. Having situations where patients are the sole conveyers of knowledge of their medical situation between specialists is not only stressful and anxiety provoking (43), it creates possibilities for miscommunication and error (44). Patients who have to worry about whether their treatment team and specialists are communicating efficiently, experience increased anxiety, not only over the need to engage in this uncertain monitoring, but also because they are put into the position of having to supplicate themselves for information and access (45). Adopting the approach of Walter Reed’s amputee rehabilitation programme to other clinical settings may offset some of the communication challenges described in the literature.
Finally, having access to and recovering alongside peers was a critical element in how former patients evaluated their recovery. Based on the results of the current study, the benefits of receiving care among peers is that individual patients are exposed to a living timeline of their own individual recovery and a chance to orient one’s own recovery trajectory. A peer-rich environment creates opportunities to be socialized into both the care setting and into post-injury life. In addition, working alongside peers gave participants the chance to be key patient peers towards newly recently injured and newly arrived patients as they moved through their own recovery.
This study has several limitations that it is important to address. First there are patients for whom the APCP is not an effective treatment plan. For some the intensely social atmosphere is inhospitable. For others outside factors impede their recovery (20). In addition to a need to explore other situations where the programme was not effective, other limitations to the study conclusions exist in 3 domains: the small sample size, the resource base that orthopaedic and extremity trauma patients and clinicians can draw upon in military health settings, and the status and prestige of military patients.
In order to understand these limitations better it would be useful for new studies to work with larger sample sizes using a mixed methods approach that offered the continued depth of ethnographic engagement with the generalizability of quantitative approaches. One of the key issues to explore in future studies is the role that resource availability plays. A key reason that participants can describe both significant relationships with care-providers, and being able to recover alongside patients at various stages of their own recovery stems from the extensive resources brought to bear on this problem by the US military. Not being attached to a private insurance model of care, the programme permitted lengths of stay that were dictated by meeting patient goals rather than a concern for overall costs. Lastly, in terms of translating the social components of this model of programme organization to other care situations, such as substance dependence, patient status plays an important, but not yet systematically researched, role in the success of the programme at Walter Reed. Being referred to as “combat wounded” or “a wounded warrior” is currently a very powerful identity in the USA, much more so than that of being a recovering substance abuser. One of the effects of this identity is that patients are in a strong position to take a lead in setting their clinical goals for their recovery. This would not be the case for civilian patients in general and for certain categories of patients more specifically (substance dependence is an obvious example).
In conclusion, beyond the explicit programmatic delivery of care, patients draw on additional, and previously unrecognized, benefits that have durable effects in their lives after rehabilitation. The 3 themes we have identified may provide a pathway for helping patients with chronic, but manageable, health conditions to develop feelings of success and confidence when they return to the community. Healthcare providers and designers of healthcare programmes can potentially learn from the Walter Reed experience, to conceptualize the delivery of care at other facilities that enable the social and psychological support identified here.
This material is supported by the Center for Rehabilitation Science Research, Department of Physical Medicine and Rehabilitation of the Uniformed Services University (HU0001-11-1-0004 and HU0001-15-2-0003) which is executed by the Henry M. Jackson Foundation, Bethesda, MD, USA. This paper is dedicated to Chris Evans.
The views expressed in this manuscript are those of the author and do not reflect the official policy of the Department of Army, Navy, Air Force, Department of Defense, or U.S. Government.


 Click to show fullsize
Click to show fullsize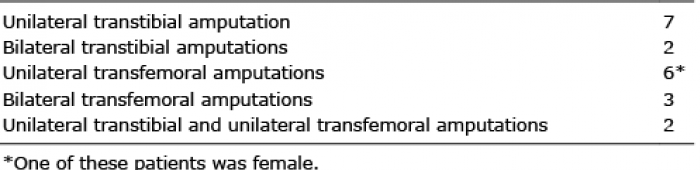 Click to show fullsize
Click to show fullsize