
From the 1Department of Rehabilitation Medicine, 2Australian Rehabilitation Research Centre, Royal Melbourne Hospital, Parkville, 3Department of Medicine (Royal Melbourne Hospital), The University of Melbourne, Parkville, Victoria, Australia, 4Center for Genomic and Precision Medicine, College of Medicine, 5Department of Medicine, 6WFNR- Blossom Specialist Medical Center, Ibadan, 7Department of Physiotherapy, College of Medicine and 8Department of Psychology, University of Ibadan, Ibadan, Nigeria
Objective: To identify potential barriers and facilitators for implementation of the World Health Organization Global Disability Action Plan (GDAP) in Nigeria and compare these with other low- and middle-income countries.
Methods: A rehabilitation team from the Royal Melbourne Hospital, Parkville, Australia, conducted intensive workshops at medical/academic institutions in Nigeria for healthcare professionals from various local Physical Medicine and Rehabilitation facilities. A modified Delphi method identified challenges for person with disability, using 3 GDAP objectives. Findings were compared with similar exercises in Madagascar, Pakistan and Mongolia.
Results: Despite differences in the healthcare system and practice, the challenges reported in Nigeria were similar to those in other 3 low- and middle-income countries, at both macro (governmental/policymakers) and micro levels (community/social/individual). Common challenges identified were: limited knowledge of disability services, limited Physical Medicine and Rehabilitation workforce, guidelines and accreditation standards; coordination amongst healthcare sectors; social issues; data and research; legislation and political commitment. Common potential facilitators included: need for strong leadership; advocacy of disability-inclusive development; investment in infrastructure/human resources; coordination/partnerships in healthcare sector; and research.
Conclusion: Disability care is an emerging priority in low- and middle-income countries to address the needs of people with disability. The challenges identified in Nigeria are common to most low- and middle-income countries. The GDAP framework can facilitate access and strengthen Physical Medicine and Rehabilitation services.
Key words: disability; rehabilitation; low- and middle-income countries; World Health Organization.
Accepted Aug 18, 2017; Epub ahead of print Oct 5, 2017
J Rehabil Med 2017; 49: 00–00
Correspondence address: Fary Khan, Department of Rehabilitation Medicine, Royal Melbourne Hospital, 34–54 Poplar Road Parkville, Melbourne VIC 3052, Australia. E-mail: fary.khan@mh.org.au
The World Health Organization (WHO) and the World Bank estimate that there are 1 billion dis-abled people worldwide (15% of the world’s population), which equates to 1 in 7 people (1). Of these, 110–190 million have significant difficulties, such as inability to walk, perform self-care, or communicate, or to participate in education or employment (1). An estimated 80% of persons with disability (PwD) live in low- and middle-income countries (LMICs) (1). The United Nations (UN) “Convention on Rights of Persons with Disabilities” (CRPD) offers a blueprint for a “rights-based” approach to mainstreaming PwD by highlighting disability as a human experience that occurs as an interaction of a person with a health condition or impairment with his/her environment, and personal factors (2). This is consistent with the International Classification of Functioning, Disability and Health (ICF) framework, that disability is a human condition and should not be viewed as a specific phenomenon affecting a limited group of people (3). The CRPD was the first UN treaty to protect the fundamental rights of PwD, and encourages all member states to adopt appropriate measures to eliminate discrimination and poverty, improve health, quality education and employment of PwD (1, 2). It identifies Physical Medicine and Rehabilitation (PM&R) as a fundamental process to support physical independence, mental, social and vocational ability (Article 26) and encourages Member States to identify and address the barriers faced by PwD (Article 31) (1).
The World Report on Disability (WRD) (WHO and the World Bank) indicates an escalating prevalence of disability, due to global population ageing, a rise in chronic conditions (including non-communicable diseases; NCDs) and an upsurge in natural/man-made disasters (1, 4).
The WRD supports implementation of the CRPD with special emphasis on PM&R (1), and highlights inadequacies in resources and access for PwD, especially in LMICs (5–7). In 2005, only 3% of individuals who needed rehabilitation globally received the service and a third of countries did not allocate specific budgets for PM&R services (1). Further, a 2006 global survey of government action (n = 114 countries) for implementation of UN Standard Rules on Equalization of Opportunities for PwD reported that rehabilitation policies were not adopted in 48 countries (42%), legislation on rehabilitation for PwD not passed in half (50%) member states, and rehabilitation programmes were not established in 46 countries (40%) (8). It is estimated that people needing prostheses or orthotic-related services represent 0.5% of the population in developing countries, whilst 30 million people in Africa, Asia, and Latin America require over 180,000 PM&R professionals to cater for the needs of PwD (9, 10). Ethnic minorities, elderly citizens, women, children, refugees and the displaced are more vulnerable amongst the PwD (11). The burden of disease and subsequent disability in Sub-Saharan Africa (including Nigeria) is colossal. The region is one of the least developed in the world in terms of rehabilitation opportunities (12, 13). In 2008, there were only 6 trained rehabilitation physicians listed in the region, all located in South Africa (12, 13).
The WHO “Global Disability Action Plan 2014–2021 (GDAP): Better Health for All People with Disability” (14), provides a list of specific actions and metrics of success to achieve 3 main objectives: remove barriers to health services; strengthen/extend rehabilitation, assistive-technology, support services, and community-based rehabilitation; and collection of disability data. The GDAP framework is a step forward in provision of PM&R services for PwD, and integrates PM&R into national and international policy development. However, it can be challenging for many LMICs and for the PM&R community, as it sets high standards requiring evidence-based rehabilitative care (15). The potential for successful implementation of GDAP is not clear, especially in LMICs, where provision of rehabilitations to PwD remains a challenge (7, 16–18). Our earlier reports highlight significant challenges in this area specifically in Madagascar (17), Mongolia (16) and Pakistan (18). These reports were based on the data collected during organized workshop-programmes in these countries to document challenges and strengths within the existing healthcare systems, corresponding with the established objectives listed in the GDAP. Although, these countries varied in terms of healthcare systems, nature and status of disability, healthcare work force and provision of PM&R services, there were many commonalities in terms of barriers/challenges in caring for PwD and the views of local healthcare professionals as to how to overcome these challenges (16).
This aim of this study was to identify potential barriers and facilitators for implementation of GDAP objectives in Nigeria and to compare the findings with those from other LMICs: Madagascar, Mongolia and Pakistan.
The authors (FK, MG), as a part of the Rehabilitation Flying Faculty from the Royal Melbourne Hospital (RMH) team, were invited as independent experts to run an organized 3-day intensive educational workshop programme by the College of Medicine, University of Ibadan and Blossom Neurorehabilitation Centre, Ibadan, Nigeria (affiliated with the World Federation for Neurorehabilitation) (March 2017)). The team previously conducted similar workshops in Madagascar, Mongolia and Pakistan (16–18). Within the Nigerian programme, a 1-day exercise concentrated solely on utilizing the GDAP framework to educate participants, build workforce capacity, develop PM&R standards and operational set-up for PM&R services within the country. This exercise was approved by the local institution and the Royal Melbourne Hospital.
The training programme at the Ibadan University was attended by 196 healthcare professionals from various hospitals, community and academic rehabilitation centres across Nigeria. These included: 21 neurologists, 98 physiotherapists (PT), 23 nurses, psychologists and social workers, 11 occupational therapists (OT) and prosthetists and orthotists (P&O), 7 speech pathologists and 31 resident medical doctors, research officers and students. The participants were from various PM&R facilities across the country (including rural areas, private sector).
Details of participants and methodology for the GDAP exercises in Madagascar, Mongolia and Pakistan have been described in previous reports (16–18).
Over the training period, the authors (FK, MG) assumed a facilitator role in conducting an intensive teaching programme and 1-day consensus meeting based on the objectives of the GDAP. Prior to the detailed workshops, the authors summarized the GDAP, evidence in the field of PM&R in various plenary and interactive panel sessions, which included: basic principles of rehabilitation, evidence-based practice and research methods, disability care planning, capacity building, leadership skills development, role of OT and speech pathologist for different neurological conditions, rehabilitation nursing; symptomatic management (spasticity, pain, wound care, etc.) and others. The lead medical team members from the “host” institutions provided information about the local health service and system, including specific challenges faced by the PM&R professionals. During these workshops, participants were divided into 3 panels to ensure that various specialist skill-base was as evenly distributed as possible, and each panel focused on one of the GDAP objectives. These panels were further divided into subgroups based on the specific content of the key GDAP objectives. All subgroups recorded their responses on a form with an overview of the GDAP. Participants in each panel, based on their experience and issues faced in service delivery, discussed their views and perspectives of various challenges and recorded specific barriers/problems and potential facilitators in line with the GDAP. At all times the GDAP was used as a blueprint for discussion and allowed the authors to educate the audience, many of whom were not familiar with the GDAP document (mainly junior doctors, nurses and some allied health professionals).
A modified Delphi-consensus method was used for the collective participant opinion. This involved a presentation by one speaker from each group, who presented on behalf of their designated panel, followed by a face-to-face large group discussion providing the opportunity to brainstorm additional and emerging issues, and to avoid the dominance of some participants that can occur in nominal group consensus methods. At the end, a formal iterative decision-making and consensus process (with ≥ 80% of participants agreeing) was conducted tabulating potential challenges/barriers and facilitators/enablers in implementation of the GDAP.
During the workshop, participants submitted their responses in writing for each GDAP objective. They were encouraged to document any emerging issues and present these in the large group interactive session. All information was supplemented with audio-recorded data and video-tape during the workshops. The author-facilitators recorded additional information, comments and recommendations provided by participants, where possible. All data were collated using a content analysis technique (19). Two authors (BA, FA) scrutinized each response and coded the information using a line-by-line process, which were further clustered into a common theme. Any discrepancies were resolved through discussion and consensus amongst all authors.
In addition, a desktop search (academic and grey literature using available medical and health science electronic databases, internet search engines and websites) was conducted for relevant publications (including academic articles, reports, related website contents, etc.) on the current status on disability and PM&R in Nigeria. All relevant information was discussed with participants in this context. Known experts in this field were contacted for further information in this area where possible.
The authors were not involved in the selection of participants in this report, as this was beyond their authority. The participants were invited by authorized delegates of the Nigerian Federation for Neurorehabilitation, in conjunction with the Blossom Centre (affiliate of the World Federation of NeuroRehabilitation) and the host institution.
Nigeria is the most populous country in Africa, with an estimated population of 182 million people (in 2015), 250 different ethnic groups and 500 different languages and dialects (20). Nigeria’s economy is one of the largest in Africa, with crude oil revenues dominating the fiscal profile and public finance (21). Like other Sub-Saharan countries, it is experiencing rapid urbanization, especially in Lagos, Kano, Abuja and Ibadan. Health service delivery, including healthcare for PwD is provided by a mixture of public and private health sectors. There are an estimated 20.1 skilled healthcare professionals and 4 physicians per 10,000 population in Nigeria. There are an estimated 3.3 million PwD in Nigeria, with a disability, prevalence rate of 2.3% (1, 22). Visual, hearing, physical, intellectual and communication impairments are common causes of disability (22). Although Nigeria ratified the CRPD in 2007, the Nigerian Constitution does not contain provisions that directly address disability (22). In 1993, the Nigerians with Disability Decree was passed by the Nigerian government, however, the Joint National Association of Persons with Disabilities is the official body in Nigeria that specifically addresses the violation of rights of PwD (23). Nigeria’s National Health Insurance Scheme (NHIS) was established in 1999, but according to the Nigeria Demographic and Health Survey Report (2008), over 97% of population have no health insurance (23). The majority of PwD receive rehabilitation from families, friends and, in a few cases, by governmental agencies (through institutional or custodial care) (23). Under the pretext of religio-cultural cover and support, many PwD undertake “begging” as their key livelihood. Even those who have received rehabilitation programmes and skills acquisition through the governmental agencies, many discontinue the application of what they have learnt (23, 24). There are no data on rehabilitation physicians in Nigeria and it is estimated that there are fewer than 2 PTs for 10,000 people. Despite the scarcity of rehabilitation resources (infrastructure and human resources), to date, there are limited systems to evaluate and/or build rehabilitation capacity (personal communication with workshop participants).
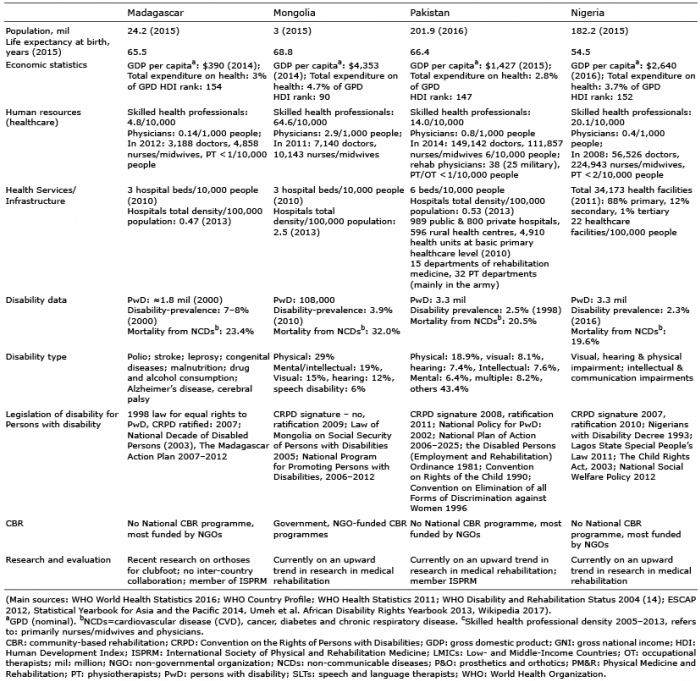
Based on the current World Bank Group’s classification to define income status of the countries (gross national income (GNI) in 2015), except Madagascar (categorized as a low-income country; GNI per capita ≤ US$1,045), all 3 countries of interest (Mongolia, Nigeria and Pakistan) are categorized as LMICs (GNI per capita: US$1,046–4,125) (25). There are significant disparities amongst the countries in terms of capacity, infrastructure and level of governance. Overall spending on healthcare by all 4 governments is low, with total mean expenditure not exceeding 3.5% of gross development product (GDP). Household out-of-pocket expenditure remains the largest source of health expenditure. Amongst the 4 countries, Madagascar has the highest prevalence rate of disability of 7–8%, while Nigeria has the lowest at 2.3%. There is limited epidemiological data on disability and disability-related burden in all 4 countries. In terms of PM&R needs and services, the picture is vague, due to lack of routinely collected disability data, limited information about the needs and unmet needs of PwD, and variability in definitions and/or ambiguous categories used for disability (e.g. physical, mental, behavioural, intellectual). In all 4 countries, the national development policies do not adequately address the concerns of PwD or include comprehensive PM&R and supportive services. Table I compares data on disabilities, disability legislation, healthcare infrastructures and resources, and support services in 4 LMICs of interest.
Table I. Summary of current health systems/resources for Disability and Physical Medicine and Rehabilitation in 4 low- and middle-income countries (LMICs)
All participants (n = 196) contributed to group discussions and the consensus method. Many (nurses, social workers) were not familiar with the GDAP, and had limited knowledge of disability programmes in Nigeria. The participants agreed that the GDAP provides comprehensive summary actions for the government, policymakers, clinicians and PwD. The participants provided multiple responses across each GDAP objective. For GDAP objective 1, participants specified 30 potential challenges/barriers and 37 potential facilitators/enablers; for objective 2: 23 challenges/barriers and 27 facilitators/enablers; and for objective 3: 18 challenges/barriers and 16 facilitators/enablers. As expected, there was significant overlap in responses regarding themes in the 3 GDAP objectives. (The complete set is available from the authors upon request).
Overall, 335 healthcare professionals participated in the GDAP reports, although the number of participants varied amongst countries: Madagascar = 29; Mongolia = 77; Nigeria = 196 and Pakistan = 33. Participants were a diverse range of healthcare professionals from various PM&R and healthcare centres. At all times, the authors as facilitators focused on appropriate strategies specific to the local situation and context, as the status of PwD differed between the countries. The number of responses across each GDAP objectives provided by participants varied amongst the countries (Table II).
Table II. Number of potential challenges and facilitators (reported by the participants) in implementation of the Global Disability Action Plan (GDAP) objectives by country
Despite variations in the healthcare systems (including PM&R) and practices amongst the 4 countries (Table I), many challenges reported by participants were common at both the macro- (governmental, policymakers) and micro-level (community, social, individual). Based on participant feedback and consensus agreement from each workshop, several common suggestive “themes” were coded, and a set of common themes were then collated using responses from all 4 workshops. The final set of common themes included 57 potential challenges/barriers and 56 potential facilitators/enablers categorized under specific headings (summarized in Table III).
This paper reports potential barriers and facilitators for the implementation of the GDAP in Nigeria and compares the findings with those from other LMICs: Madagascar, Mongolia and Pakistan. The aim was to gather information using a “bottom-up” approach in the context of national PM&R and disability status, met and/or unmet needs in rehabilitation care and potential enablers/facilitators in improving functioning and quality of life of PwD. The data include direct reports from the field with participants’ personal experiences in their specific health services, their perspectives of various challenges and specific barriers/problems relating to service provision, attitudes/approaches to PwD, rehabilitative care, education, etc., in line with the GDAP. The authors envisaged that this process would help build national PM&R capacity, and provide a much-needed conceptual framework for successful implementation of the GDAP.
Consistent with the worldwide pattern of population health transition, all 4 countries of interest are in a stage of epidemiological transition from communicable diseases to NCDs, which account for a predominant share of morbidity and mortality. Despite prioritization of PM&R as a key agenda by the governments, the level of funding, human resources and health infrastructure is suboptimal in all 4 countries, particularly in rural areas. Despite the exponential growth and development of healthcare facilities and programmes in many LMICs, the systems are explicitly hospital-centred, resulting in a fragmented and inefficient hospital sector (26). The primary healthcare sector and community-based services (such as PM&R services) are yet to develop optimally; with inadequate financing systems, human resources, planning and regulatory processes (26). For example, though PM&R departments exist in many major hospitals in Pakistan and Mongolia, most are ambulatory and operate in silos and most programmes are not integrated with other healthcare systems and processes. While PM&R services are mostly conjoint with and/or subjugated by traditional medicine in Mongolia, they are mostly based within military services in Pakistan, while in Nigeria and Madagascar comprehensive rehabilitation programmes are in their infancy. None of the countries have a universal healthcare system. In Mongolia PM&R is not covered by insurance. In all 4 countries, the national PM&R services are not well integrated within acute care systems and/or rural health departments, non-governmental organizations (NGOs)/ international non-governmental organizations (INGOs) and the private sector. Many provide these services mostly through vertically-managed disease-specific mechanisms (16–18). Similar to most developing countries, care of PwD (including CBR) in all 4 countries is predominantly funded by NGOs/INGOs and charitable organizations at a community level. There is poor coordination amongst these INGOs/NGOs working in the field of disability management and existing PM&R services. This is compounded by discernible urban-rural disparities in healthcare delivery and health workforce (27).
All 4 countries Madagascar, Mongolia, Nigeria and Pakistan have made some progress in building national health capacity in the acute healthcare sector, public health emergency preparedness, infection prevention and control. However, great disparities in health status exist and PM&R is less prioritized (16–18, 23). There appear to be contrasts and imbalances within operational healthcare systems in many LMICs, including in Madagascar, Mongolia, Nigeria, Pakistan, in terms of policies, funding structure/infrastructure, healthcare systems and capacity, human and physical resources, technology, etc. (Table I). Data for disability are scarce and there is variability in definitions and ambiguous categories used for disability. Despite these variations, many challenges for the PM&R sector in terms of implementation of the GDAP seem to be common to most LMICs. Key common potential challenges and/or enablers reported by the participants from 4 countries of interest in this report for implementation of the GDAP, particularly for PM&R service provision, are summarized below:
Governance, policy and planning. Similar to many LMICs, legislation for overall management of PwD has been adapted in all 4 countries; however, existing policies are under-funded, there is lag in implementation of PM&R policies and/or overall delivery of such services, as well as lack of coordination and collaboration amongst different sectors. Key barriers in healthcare service provision include lack of political commitment, inadequate funding and corruption.
There is need for a strong leadership role by national disability authorities to coordinate and provide standards for rehabilitative care, develop key performance indicators for PM&R to enhance capacity of national healthcare organizations, develop inter-disciplinary and inter-sectoral partnerships of all stakeholders for longer-term care planning of PwD. The GDAP recommendations need to be tailored to suit the local environment for relevance to mainstream services, policymakers and administrators.
Rehabilitation-inclusive healthcare infrastructure and human resources. Many PwD require specialized, efficient management and health services, which are often limited or lacking in most LMICs, particularly in rural areas. The PM&R services across countries vary, and most LMICs have limited or no organized PM&R services (1). Various PM&R services for PwD are funded by INGOs/NGOs and charitable organizations. There are limited sub-specialized PM&R services (such as stroke units, spinal cord injury (SCI) centres), and many such units, as in Pakistan and Mongolia, are restricted to urban areas (28). There is limited or lack of modern equipment (therapeutic and diagnostic), which hinders the provision of service delivery. Available resources, including workforce, in most LMICs are inadequate and inequitably distributed (1, 29). There is limited financial support for development of the PM&R workforce, with a shortage of allied health professionals (OTs, speech therapists, prosthetics, etc.) and few educational/training facilities for PM&R capacity building.
The LMICs need to develop a self-sustaining rehabilitation-inclusive healthcare capacity (at various levels) to cater for the needs of PwD. There is a critical need to build a system, integrating and linking healthcare services with other emerging sub-specialties including PM&R. Furthermore, there is a need to improve infrastructure for disabled access for transport and buildings, social support systems at a national level with leadership from government and relevant authorities for training and empowerment programmes for the PM&R workforce.
Health information and referral systems. Data on disability and PM&R are fragmented and often not disaggregated from other healthcare services information. Improvement in accessibility and overcoming information barriers are a priority for optimal planning and resource allocation. There is need for a system for collection of data by relevant services, with a lead governing agency facilitating and coordinating this information for dissemination to relevant authorities. An appropriate referral mechanism for PwD is lacking at many levels; this results in gaps in appropriate services and the care continuum in the community for PwD.
Education and awareness. Despite evidence of growing public acceptance of PwD in many LMICs widespread stigma and discrimination against these people persist and many are ostracized. Due to poor education and lack of appropriate information, many PwD are unaware of specialities such as rehabilitation. This hinders their active societal participation and opportunities to interact with their able-bodied counterparts (30). There is minimal awareness regarding rehabilitation amongst the general population and it is often confused with traditional or alternative medicine. Lack of trust of medical practitioners by PwD is prevalent in some cultures, particularly in rural areas, where many seek help from religious and traditional healers (1, 31).
Strong policy measures will eliminate discrimination, prejudice and barriers to the socio-political and economic well-being of PWDs. Increased public awareness and active inclusion of PwD (and their families) in decision-making and goal-setting is required. Capacity building for disability/consumer organizations on the rights of PWDs is needed in line with the UN CRPD.
Service delivery and costs. Whilst there are limited PM&R services in rural areas, access to such facilities in urban areas is often costly, time-consuming and difficult (32). The cost of access to PM&R services is a significant barrier, as most services are available only as an out-of-pocket payment. There is lack of universal health insurance systems and many private health insurance systems do not cover rehabilitation. This results in financial hardship and inequity in utilization of healthcare services (28, 33). There is still a large gap in provision of basic equipment and assistive devices (canes, crutches, prostheses, wheelchairs, etc.). Strengthening national capacity for integrated PM&R services at all levels by the national governments is required.
Community-based rehabilitation and consumer groups. There are a limited number of community-based rehabilitation facilities, professional, caregiver and consumer groups. The needs of PwD are often overlooked and many remain marginalized and their capabilities underestimated. Various community-based initiatives should be in place to empower and strengthen community-based organizations for longer-term rehabilitation of PwD. Governments should ensure the socio-economic security of these individuals and communities, where possible.
Research and evidence-based information. There is limited research capacity for disability issues in the majority of LMICs, preventing development of comprehensive country-specific policies and programmes. Furthermore, access to evidence-based information is not optimal. More funding and promotion for research should be initiated and all expertise/stakeholders (and related organizations) should be considered for knowledge transfer and education. Multi-stakeholder partnerships (national and international) can build and implement evidence-based management approaches. Governments should collaborate with healthcare organizations, academic and community organizations to implement existing and new research programmes.
This study has some limitations. It is a cross-sectional study and does not test specific hypotheses through systematic analysis. A content analysis technique was used to summarize subjective data derived from the interactive feedback based on personal opinions, interpretations, clinical practices, points of view and judgement from participants attending organized workshop programmes. This study was intended as a preliminary comparative study, with the aim of comparing PM&R efforts in 4 different LMICs based on the GDAP, and to identify barriers/challenges and facilitators from perspective of participants for the implementation of GDAP. Participants were invited by local institutions and many other relevant stakeholders (such as governmental, social work organizations, organizations of PwD) may have been missed, which may limit the generalizability and validity of findings. However, the study cohort, covered PM&R professionals from a wide geographical population in the country, and represented the health professionals currently operational in the community (both urban and rural). A modified Delphi method allowed all participants to express their views and contribute their opinion on potential barriers/challenges for successful implementation of the GDAP. Cultural and/or social demographic impact of the participating countries could not be assessed; this was beyond the scope of this article. Participant feedback was positive, and most were satisfied with the overall consensus process. Multidisciplinary input within the groups was beneficial, as groups were diverse in their areas of expertise. The group heterogeneity was reflected in the broad participant responses. Group discussion and consensus rounds served to remove duplicate or similar themes/issues and to formulate a final set of common barriers and facilitators. The authors believe the findings reflect the current issues faced by the PM&R workforce in LMICs.
In summary, there is a strong impetus to improve disability care and the PM&R sector in these countries. The GDAP provides comprehensive summary actions for disability and offers the government authorities, policymakers and other relevant stakeholders a blueprint for implementing new comprehensive programmes for long-term care of PwD. The UN and WHO are key global players for the care and management of PwD in LMICs. The International Society of Physical and Rehabilitation Medicine (ISPRM) (and the ISPRM-WHO-Liaison Committee) can play a role in the ISPRM-WHO Collaboration Plan (2014–2017) to develop appropriate, effective sustainable policies, strategies and plans to strengthen the provision of rehabilitation, specifically in LMICs (34).
The role of PM&R in the healthcare system in LMICs is expanding to address the needs of growing numbers of PwD. The GDAP provides a major boost for PM&R services to enhance the quality of life of PwD worldwide. There is opportunity for PM&R professionals, consumer organizations and NGOs to take a strong leadership role and to prioritize the challenges that need to be addressed for successful implementation of the GDAP.
The authors thank all Nigerian organizers and participants for contributing to this study. In particular, we thank Ms Ezinne Uvere and the University of Ibadan for their kind hospitality. We also acknowledge members of the Royal Melbourne Hospital Team, specifically Dr Geoff Abbott, Ms Lauren Fletcher and Ms Marlena Klaic for their assistance.
The authors declare no conflicts of interest.


 Click to show fullsize
Click to show fullsize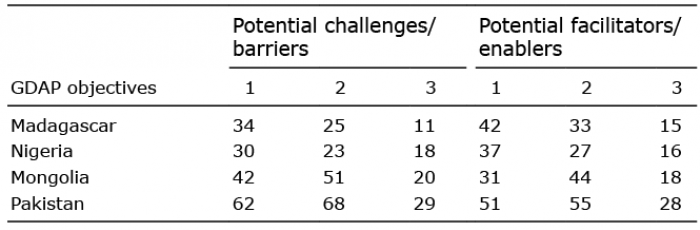 Click to show fullsize
Click to show fullsize