
From the ¹Inserm Unit 1179, Team 3: Technology and Innovative Therapies Applied to Neuromuscular Diseases, University of Versailles Saint Quentin en Yvelines, 2Department of Physical Medicine and Rehabilitation, R. Poincaré Hospital (AP-HP), Garches and 3Laboratory LAMHESS, University Côte d’Azur, Nice, France
Objective: Fatigue and fatigability are common problems in patients with multiple sclerosis, which might be improved by rehabilitation. The aim of this pilot study was to assess changes in the fatigue and fatigability of knee extensors in patients with multiple sclerosis after a short intensive, combined rehabilitation programme (including physiotherapy primarily focused on gait and balance, endurance and resistance training).
Methods: Twenty-three patients with multiple sclerosis (10 men, 13 women) underwent isokinetic evaluations of fatigability of the knee extensor muscles during concentric contractions and rated a self-reported fatigue scale (Modified Fatigue Impact Scale; MFIS) before and after a rehabilitation programme. Patients performed rehabilitation for 150 min, 4 days per week for 4 weeks, with physiotherapy focused primarily on gait and balance, endurance training and resistance training.
Results: After rehabilitation, perception of fatigue decreased significantly (median MFIS scores [1st; 3rd quartiles], pre: 44 [33; 53] vs post: 33.5 [16; 43]; p < 0.00025). Moment fatigue index increased (pre: 37.70 ± 13.40 vs post: 48.10±9.39; p < 0.0125), but end-test moment did not change. After rehabilitation, strength increased during both isometric and concentric contraction (mean first 5 and mean 50 contractions of the fatigue protocol) (p < 0.0125). After rehabilitation, neuromuscular efficiency improved (p < 0.0125).
Conclusion: After a short, intensive, combined rehabilitation programme, fatigue decreased but fatigability increased (moment fatigue index). Indeed, fatigability increased because strength in the initial state increased and strength in the fatigued state did not change. Although the rehabilitation programme was designed so that resistance training was carried out after endurance training to specifically train muscles in a fatigued state, no improvements in strength in the fatigued state were measured.
Key words: muscle fatigue; quadriceps muscle; rehabilitation; endurance training; resistance training; isokinetic assessment.
Accepted Aug 14, 2017; Epub ahead of print Oct 5, 2017
J Rehabil Med 2017; 49: 00–00
Correspondence address: Sophie Hameau, Inserm Unit 1179, Team 3; Department of Physical Medicine and Rehabilitation 104 Bd R. Poincaré, FR-92380 Garches, France. E-mail: sophie.hameau@aphp.fr
Patients with multiple sclerosis (pwMS) report that fatigue is one of their worst symptoms, severely affecting daily activities and reducing quality of life (1, 2). Fatigue is defined as “the subjective sensation of a lack of physical and/or mental energy which interferes with usual and desired activities” (3), whereas fatigability is defined as any contraction-induced reduction in the ability to generate maximal muscle force or power output (4, 5). Forty percent of pwMS describe fatigue as their worst symptom (6) and studies have demonstrated that fatigability is greater in pwMS than in healthy subjects (7, 8).
A Cochrane meta-analysis showed that exercise therapy is safe and effective for the treatment of fatigue in pwMS (9). Few studies have investigated the impact of rehabilitation on fatigability in pwMS, and the results are disparate, making it difficult to draw conclusions. For example, fatigability assessed with an index decreased significantly, from 55% to 41%, after an aquatic fitness programme (10), while a combined 6-month rehabilitation programme including endurance and resistance training decreased the fatigability of the knee extensor muscles in women, but not in men (11).
The optimal method to reduce fatigue and fatigability in pwMS has not yet been determined. A Cochrane meta-analysis suggested that endurance training and combined training were more effective than resistance training to reduce fatigue (9). Moreover, studies in patients with other chronic conditions have suggested that combined training reduces fatigability more effectively (12, 13). Nevertheless, there have been few studies of combined programmes in pwMS (14). This approach appears to be pertinent, since it could improve both aerobic capacity and muscle strength (15). Most studies of rehabilitation in pwMS have involved long rehabilitation programmes (several months to one year). However, it is very difficult to implement such long interventions in clinical practice. Short rehabilitation programmes have been shown to effectively increase aerobic capacity (16); however, the impact on fatigability has not yet been assessed. Short, intensive rehabilitation programmes are more realistic in the hospital setting, particularly for patients who are still working. The aim of the present study was to assess adaptations of fatigue and fatigability of knee extensors after a short intensive, combined rehabilitation programme in pwMS (including physiotherapy primarily focused on gait and balance, endurance and resistance training). To that end, the Modified Fatigue Impact Scale (MFIS) was completed, and peak moment and electromyographic (EMG) activity of the rectus femoris (RF), vastus lateralis (VL), biceps femoris (BF), and semitendinosus (ST) muscles were recorded during 50 maximal concentric contractions, before and after a 4-week rehabilitation programme. We hypothesized that fatigue and fatigability would decrease after the short, intensive, combined rehabilitation programme.
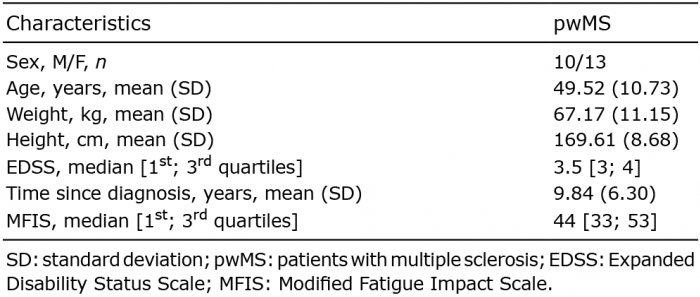
Twenty-three pwMS were enrolled in this study. Inclusion criteria were: a diagnosis of MS with an Expanded Disability Status Scale (EDSS) ≤ 6; no relapse within the last 3 months; no changes in MS-medication; and no participation in a rehabilitation programme within the last 6 months. The characteristics of the included pwMS are shown in Table I. This study was performed in accordance with the ethical codes of the World Medical Association (Declaration of Helsinki) and was approved by the local ethics committee (CPP Ile de France XI–St Germain-en-Laye). All subjects provided written informed consent. Clinical trial registration number: NCT02352194.
Table I. Characteristics of the patients with multiple sclerosis
PwMS were assessed before (the week before) and after (the week after) the rehabilitation programme. They completed the MFIS, a measure of the impact of fatigue on daily life. This scale, which is a short form of the 40-item Fatigue Impact Scale (2), assesses the impact of fatigue on physical, cognitive and psychosocial aspects of the patient’s life. Higher scores indicate higher levels of fatigue. An isokinetic evaluation of strength and fatigability of the knee extensor muscles of the weakest limb was then carried out. In multiple sclerosis, symptoms such as muscle weakness occur asymmetrically; therefore the investigation was targeted on the weakest limb.
Before and after the rehabilitation programme, instantaneous isokinetic moments were recorded using a ConTrex-MJ isokinetic dynamometer (Contrex, CMV AG, Dübendorf, Switzerland). The set-up has been described elsewhere (17). Gravity correction was performed during the trials using the ConTrex-MJ software (Contrex, CMV AG, Dübendorf, Switzerland). All subjects completed a dynamic warm-up that consisted of concentric sub-maximal contractions of the knee flexor and extensor muscles at 60°/s in order to familiarize themselves with the procedure. Maximal voluntary strength was then measured for 5 s during isometric contractions (ISO) of the knee extensor muscles, with the knee flexed at 90° (EXTMVIC). Next, 5 concentric maximal voluntary contractions of the knee flexor muscles (CONC) were performed at 60°/s in order to calculate the degree of co-activation during the fatigue protocol. The voluntary isokinetic fatigue protocol consisted of 50 maximal concentric contractions of the knee extensor muscles at 60°/s with a passive return to the initial knee position. This protocol has previously been shown to effectively fatigue the knee extensor muscles in patients with neurological diseases (18). After the fatigue protocol, isometric maximal voluntary contractions of the knee extensor muscles (EXTMVIC) were again performed. Verbal encouragement was given to the subjects to ensure that they produced a maximal effort during each contraction.
Electromyographic (EMG) activity of the RF, VL, BF, and ST of the weakest limb were recorded simultaneously during each isokinetic session. Four bipolar surface electrodes with built-in pre-amplification (SX230 Active EMG Sensor, Biometrics, Ladysmith, VA, USA) were placed directly on the skin, according to SENIAM recommendations (19). Prior to electrode placement, the skin area was shaved, abraded and cleaned with alcohol in order to reduce skin impedance and ensure adhesion of the electrodes. The EMG sensors comprised 2 circular, stainless-steel, dry-button electrodes with double-differential preamplifiers. The 2 active electrodes measured 12 mm in diameter and the inter-electrode distance was 17 mm. A ground electrode was placed on the subject’s wrist during measurements. All EMG signals were sampled at 1000 Hz and pre-amplified by a factor of 20, at the electrode site. Before analysis, the raw EMG data were band-pass filtered between 3.5 and 350 Hz.
The short, intensive, combined programme included for each session: (i) 1 h of physiotherapy with exercises focused primarily on gait and balance; (ii) 40 min of endurance training on a cycle ergometer supervised by an exercise specialist; and (iii) 40 min of resistance training on a isokinetic dynamometer supervised by a physiotherapist. This programme was performed 4 times per week (150 min per session) for 4 weeks. The first hour focused mainly on balance and gait training, with lower limb muscle stretching, and strength training with weight-bearing exercises and activities, such as learning to get up from the floor, stand up and sit on a chair. Gait training (15 min) was carried out in 3 conditions that changed at each session: inside, outside and on a treadmill. Balance training (15 min) was adapted to the patient’s capacity, in 3 conditions that changed each session: one in the standing position, one in different positions of standing upright, and one with extrinsic destabilization (foam, balls) (all of them with eyes open/closed, variation of the support polygon (tight feet, tandem...) and intrinsic destabilization). Next, subjects performed 30 min of continuous endurance exercise on a cycle ergometer at 60% peak power output (Wmax) (power output was previously determined during a cardiopulmonary exercise test), with a 5-min warm-up and a 5-min cool-down at 30% of Wmax, as recommended by Dalgas et al. (15). This intensity was largely used for endurance training and has shown an increase in power output and maximal aerobic capacity, which prompted us to choose this protocol (16, 20–22). Subsequently, 40 min of resistance training of the knee flexor and extensor muscles of both lower limbs was performed on an isokinetic dynamometer. A warm-up was performed with concentric sub-maximal contractions of the knee flexor and extensor muscles at 60°/s. Then patients executed 6 sets of 6 maximal voluntary contractions of knee flexor and extensor muscles. There was a 2-min rest period between sets. As the resistance training was performed on an isokinetic dynamometer, the resistance was adapted to the moment developed by the patient, so fully adapted to the patient’s progression.
The results of the MFIS were expressed as a total score, as well as the score of the physical subscale (9 items). For the concentric trials, only data (moment and EMG in the load range that is the constant velocity portion were analysed (23). All isokinetic and EMG data were exported to text files and processed using custom algorithms developed in MatLab version 9.0 (The MathWorks, Inc., Natick, MA, USA). Maximal peak moment for each contraction was determined by the peak value in the moment curve. The best performance was analysed. The percentage decrease in moment between PRE fatigue EXTMVIC and POST fatigue EXTMVIC was calculated. The mean root mean square (RMS) value of the RF, VL, BF and ST muscles (respectively RFRMS, VLRMS, BFRMS and STRMS) was calculated over a 500-ms period around the occurrence of the peak moment (i.e. 250 ms before and 250 ms after).
For the fatigue protocol, peak moment was: (i) expressed as raw data (N*m); (ii) normalized to the peak moment value of first 5 concentric contractions of the fatigue protocol (normalized moment (%max CONC)); and (iii) normalized to the PRE EXTMVIC (normalized moment (%max ISO)). RMS values were normalized to the highest value recorded during the 50 concentric contractions for each subject (RMSnorm). Neuromuscular efficiency (NME) was calculated for each repetition by dividing the peak moment by the corresponding normalized RF and VL RMS values (RFNME and VLNME) (24). BF and ST co-activation (BFCOACT and STCOACT) was calculated as the ratio of EMG activity during the maximal extension contraction of the fatigue protocol (60°/s) to the EMG activity during the maximal flexion contraction (PRE test at 60°/s)*100. Mean peak moments, co-activation and RMSnorm from the first and the last 5 contractions and mean moment of the 50 contractions were calculated. Moment fatigue index was also calculated: Moment FI (%) = 100 – (Moment final [mean 5 last contractions]/Moment initial [mean 5 first contractions]*100). The fatigue index was also calculated for RMS, NME and co-activations.
Discrete variables were expressed as median values [1st; 3rd quartiles] and continuous variables were expressed as mean and standard deviation (SD). Shapiro–Wilk tests were conducted before the statistical analysis and showed that the data were not normally distributed. A Friedman’s 2-way analysis of variance (ANOVA) was performed. Paired Wilcoxon tests were performed on all significant results. The analysis involved the comparison of results from 4 evaluations (before rehabilitation (PRE and POST fatigue protocol) and after rehabilitation (PRE and POST fatigue protocol) the level of significance p < 0.05 was divided by 4 and was set as p < 0.0125 for each ANOVA (*p < 0.0125; **p < 0.00025).
Peak moment during EXTMVIC (PRE fatigue) increased significantly after the rehabilitation programme, (p < 0.0125, Table II).
Table II. Impact of rehabilitation on strength, fatigability, neuromuscular efficiency and co-activation
For the concentric contractions, the mean moment (raw data) during the first 5 contractions and the mean moment during the 50 contractions both increased significantly (both p < 0.00025, Fig. 1).
Fig. 1. (A) Moment (raw data), (B) Normalized moment (% max CONC), and (C) normalized moment (% max ISO) developed by the knee extensor muscles during fatigue protocol before and after rehabilitation.
Normalized moment during the first 5 contractions (%max ISO), expressed as percentage of PRE EXTMVIC, increased significantly after rehabilitation (p = 0.007). RFRMS and VLRMS during the first 5 contractions were not modified after rehabilitation (respectively p = 0.12 and p = 0.049, Table II). The RFNME and VLNME during the first 5 contractions were both increased after rehabilitation (p < 0.0125, Table II).
Peak moment during EXTMVIC decreased significantly from PRE to POST fatigue protocol, both before and after rehabilitation (respectively p = 0.001 and p = 0.005) (Table II). The percentage decrease from PRE to POST fatigue protocol did not change after rehabilitation (p = 0.28). Moment fatigue index in men with pwMS was not statistically different from women with pwMS (respectively 39.4 (14.6) and 36.4 (12.8); p = 0.47). This allows us to pool results for men and women for the statistical analysis. After rehabilitation, the moment fatigue index increased (p = 0.0068) (Table III). During the concentric contractions, mean moment (raw data) and normalized (%max ISO) of the last 5 contractions did not change after rehabilitation (respectively p = 0.028 and p = 0.37). Normalized moment during the last 5 contractions (%max CONC) decreased significantly after rehabilitation (p = 0.008). Peak extensor moment (raw data) and normalized moment (%max CONC and %max ISO) decreased from the first 5 to the last 5 contractions of the fatigue protocol, both before and after rehabilitation (p = 0.0002) (Fig. 1).
Table III. Fatigue indexes before and after rehabilitation
The RFNME and VLNME during the last 5 contractions both increased after rehabilitation (p < 0.0125). RFRMSnorm, VLRMSnorm, RFNME and VLNME fatigue indexes were not modified after rehabilitation (respectively p = 0.017, p = 0.058, p = 0.76 and p = 0.71). RFRMSnorm, VLRMSnorm, decreased significantly during the fatigue protocol both before and after rehabilitation (respectively p = 0.006; p = 0.001; p = 0.0087; p = 0.00028). RFNME and VLNME decreased significantly during the fatigue protocol both before (p = 0.00008 and p = 0.00006) and after rehabilitation (p = 0.001 and p = 0.0009). BFCOACT and STCOACT did not change during the fatigue protocol.
The median MIFS fatigue score decreased significantly after rehabilitation (44 [33; 53]; 33.5 [16; 43]; p < 0.00025). The median scores of the physical domains of the MFIS also decreased significantly (25 [22; 28]; 17 [12; 23]; p < 0.00025).
These results show that a short, intensive, combined 4-week rehabilitation programme involving physiotherapy primarily focused on gait and balance, endurance and resistance training, increased both strength and neuromuscular efficiency. Contrary to our hypothesis, fatigability was not improved after the rehabilitation. Fatigability increased because moment increased at the beginning of the fatigue protocol (non-fatigued state), but there was no change in the moment produced at the end (fatigued state). As we hypothesized, perception of fatigue (MFIS score) decreased significantly.
After the short, intensive, combined rehabilitation programme, knee extensor muscle moment and NME of RF and VL improved, with no change in co-activations. This improvement in strength (17% for MVIC) was similar to that found in previous studies involving longer rehabilitation programmes for pwMS (25–27). This confirms that an intensive, short rehabilitation programme of 4 weeks’ duration can significantly improve voluntary muscle strength. Moreover, normalized moment (% max ISO) during the first 5 concentric contractions was significantly increased after rehabilitation. Before rehabilitation, pwMS produced only 81% of the EXTMVIC moment during the first 5 concentric contractions. This is lower than that reported in healthy subjects (≈90%) (28). This exaggerated decline in normalized moment between isometric and concentric contractions (60°/s), has also been found in patients with hemiparesis. It has been attributed to a reduction in neural drive, resulting in insufficient activation of agonist muscles during concentric contractions (29). The discrepancy between isometric (0°/s) and concentric contractions (60°/s) could also be explained by the selective non-use of fast twitch fibres, and overuse of slow twitch muscle fibres in upper neurone lesions (30). After the rehabilitation, the pwMS produced 90% of their EXTMVIC moment, which is close to values reported in healthy subjects. If the increase in strength was due to a learning effect, it would be observed at the beginning and end of the fatigue protocol, but the increase in strength was present only at the beginning of the fatigue protocol, thus it appears to be due to adaptations of the rehabilitation programme. This improvement was not related to changes in co-activation, but appeared to be the result of increased NME without changes in RMS. NME is the ability to generate force with the same level of muscle activation (RMS) (31). These results are important because activities of daily living frequently involve concentric contractions at low velocities, such as rising from a chair or walking upstairs. In conclusion, the short, intensive rehabilitation programme increased the strength of the knee extensor muscles, with an increase in the value of the moment–velocity relationship (%max ISO).
According to Gandevia’s definition (4), the significant decrease in moment during the fatigue protocols, and between the PRE and POST isometric contractions, confirmed that fatigue was achieved. Our results showed that the relative decrease in moment during repeated maximal concentric contractions was greater after rehabilitation than before (moment fatigue index). This is contrary to our hypothesis. Previous studies have reported conflicting results regarding fatigability (10, 11). However, since most studies used different testing procedures (isometric vs concentric contractions (11) or low vs high velocity (10)), it is difficult to compare studies. Indeed, the dominant mechanism producing fatigability depends on the task (32). In our data, no correlation between strength during isometric and concentric contractions and moment fatigue index were found (data not presented). Since the correlation between strength and fatigability has been shown in healthy persons where stronger subjects were also less resistant to fatigability (33, 34) in persons with MS, mechanisms of fatigability appear to be more complex and probably involved more parameters.
Analysis of only the moment fatigue index showed that fatigability increased after rehabilitation. However, close analysis of the raw and normalized moments (%max ISO) showed that there was no change in strength at the end of the fatigue protocol after the rehabilitation programme, thus moment produced in the fatigued state remained unchanged. The similar end-test moment suggests that the critical moment remained the same during the maximal concentric contractions. Although the moment at the beginning of the fatigue protocol increased, the moment at the end of the test was unchanged. These results are consistent with previous studies that hypothesized that there is a critical moment during maximal contractions, above which rapid fatigability will occur, and below which the exercise can be continued for an extended period (35). NME was reduced at the end of the fatigue protocol, both before and after the rehabilitation, suggesting that peripheral fatigue occurred during the fatigue protocol (24). Since neither NME nor the RMS fatigue index changed after rehabilitation, the rehabilitation did not change the type of fatigue that occurred during the fatigue protocol. In conclusion, the moment fatigue index was higher after rehabilitation because (i) moment at the beginning of the fatigue protocol was increased; and (ii) moment at the end of the fatigue protocol did not change after rehabilitation (same end-test moment). In order to decrease fatigability, the resistance training could have been more focused on strength-endurance with more repetitions and less resistance.
In the current study, 56% (13/23) of patients were categorized as having fatigue (MFIS total score higher than 38), before rehabilitation (36). This is similar to a previous study, which reported a prevalence of 58% (26). After 4 weeks of intensive, combined rehabilitation, fatigue (MFIS) decreased significantly. Results in the literature are conflicting. Previous endurance training programmes failed to show differences in fatigue (20, 22), while some studies involving progressive resistance training demonstrated decreases in fatigue (26, 37). In our study, the decrease in fatigue was particularly related to decreases in the physical domains of the MFIS. The decreases in physical fatigue and total fatigue were greater than the minimal clinically important differences (respectively 3.85 units (–7) and 7.9 units (–10.5)) (26). These results are significantly greater than the results of pharmacological or psychosocial treatments for fatigue (38). Fatigue strongly affects daily life and is a significant factor that influences both work capacity and health-related quality of life (39). The present results showed that a combined rehabilitation programme could have a positive impact on patients’ quality of life. A short (4-week), combined rehabilitation programme therefore seems to effectively decrease fatigue.
This study has some limitations. The results must be interpreted with caution because of the small sample size and lack of a control group. Indeed, this was a pilot study; a randomized controlled study is needed to confirm the results. RMS data have not been normalized with M waves so must also be interpreted with caution. Moreover, NME is an interesting parameter; however, the measure of voluntary activation ratio by the interpolated twitch technique was not conducted to specifically differentiate central from peripheral fatigue. This assessment was not included in our study design.
A short, intensive, combined rehabilitation programme could effectively decrease fatigue in pwMS, particularly physical fatigue. Knee extensor muscle moment (ISO and CONC) increased, and the reduction in torque between isometric and concentric contractions decreased. Moreover, the moment fatigue index during concentric contractions increased. The combined programme did not lead to a change in the end-test moment of the fatigue protocol, suggesting that it was a critical moment. Although the rehabilitation programme was designed so that resistance training was carried out after endurance training to specifically work muscles in a fatigued state, the results showed an improvement in strength in the non-fatigued state, but not in the fatigued state. Further studies should investigate the impact of combined rehabilitation programmes on locomotor performance and activities of daily living in pwMS.
The authors thank Johanna Robertson for revising the English in this manuscript.
The authors declare no conflicts of interest.


 Click to show fullsize
Click to show fullsize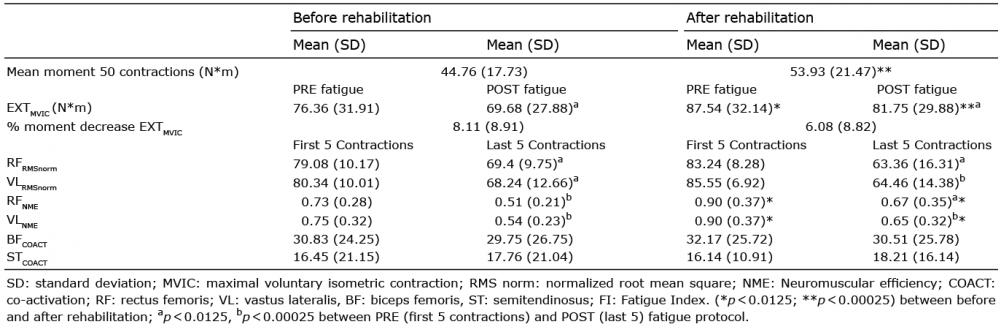 Click to show fullsize
Click to show fullsize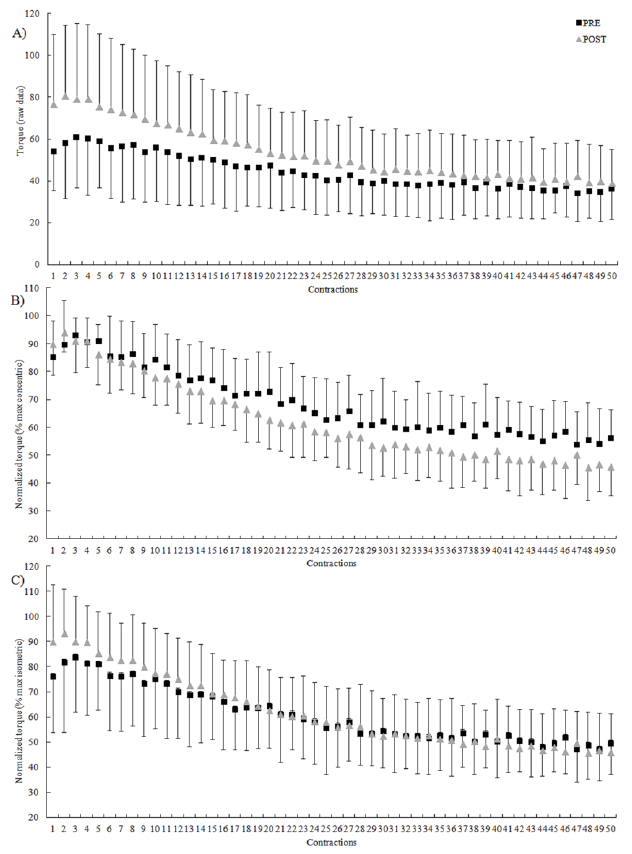 Click to show fullsize
Click to show fullsize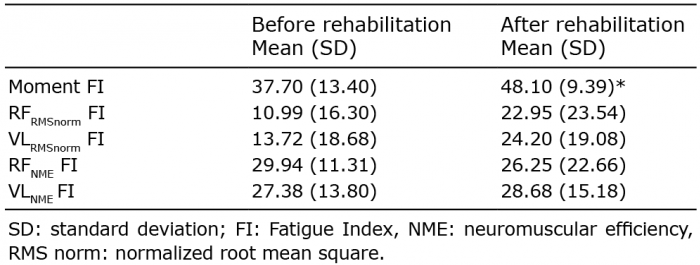 Click to show fullsize
Click to show fullsize