
From the 1Amsterdam Rehabilitation Research Center, Reade, 2VU University Medical Center, Department of Rehabilitation Medicine, 3VU University Medical Center, Department of Psychiatry, 4VU University Medical Center, Department of Rheumatology and 5Jan van Breemen Research Institute, Reade, Amsterdam, The Netherlands
Objective: Muscle weakness is common and strongly related to clinical outcome in patients with knee or hip osteoarthritis. To date, there is no clear overview of the information on factors associated with muscle strength in knee and hip osteoarthritis. The aim of this paper is to provide an overview of current knowledge on factors associated with upper leg muscle strength in this population.
Design: The framework of a scoping review was chosen. MEDLINE database was searched systematically up to 22 April 2017. Studies that described a relationship between a factor and muscle strength in knee or hip osteoarthritis were included.
Results: A total of 65 studies met the inclusion criteria. In studies of knee osteoarthritis, 4 factors were consistently found to be associated with lower muscle strength. Due to the low number of studies on hip osteoarthritis no conclusions could be drawn on associations.
Conclusion: Lower muscle quality, physical inactivity, more severe joint degeneration, and higher pain are reported to be associated with lower strength in the upper leg muscles in knee osteoarthritis. Future research into knee osteoarthritis should focus on other potential determinants of muscle strength, such as muscle quantity, muscle activation, nutrition and vitamins, and inflammation. In hip osteoarthritis, more research is needed into all potential determinants.
Key words: hip joint; knee joint; osteoarthritis; muscle strength.
Accepted Sep 11, 2017; Epub ahead of print Nov 29, 2017
J Rehabil Med 2018; 50: 00–00
Correspondence address: Arjan de Zwart, Amsterdam Rehabilitation Research Center | Reade, Dr, Jan van Breemenstraat 2, NL-1056 AB, Amsterdam, the Netherlands. E-mail: a.d.zwart@reade.nl
Muscle weakness is common in patients with knee or hip osteoarthritis (OA) (1, 2). Upper leg muscle strength is reported to be approximately 20–40% lower compared with healthy age-matched controls (1, 3). Muscle weakness in knee or hip OA is strongly related to the patient-reported outcomes pain, activity limitations and falls, and has been linked to symptomatic progression of the disease (2, 4–8). Moreover, muscle weakness has been reported to be a risk factor for radiographic progression and the development of knee OA (9, 10).
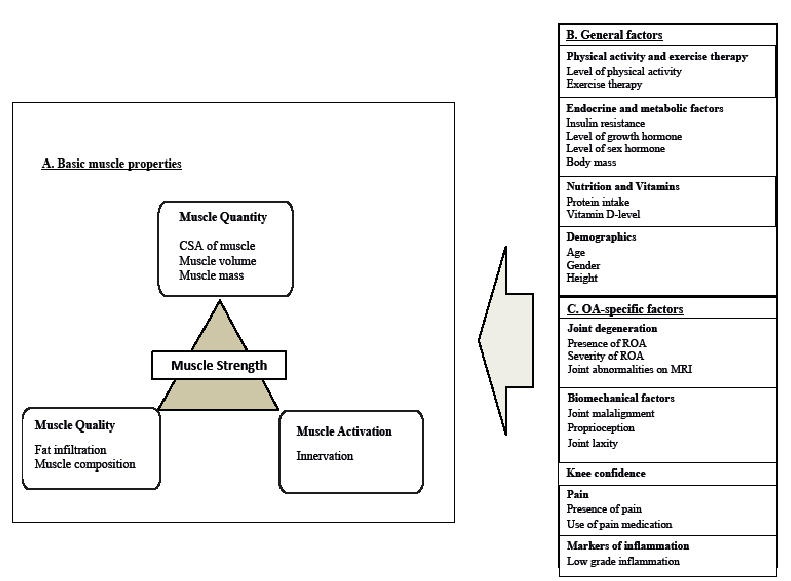
Muscle strength is the ability to exert a physical force (11). The force generated by a muscle is determined mainly by basic properties of the muscle itself, such as quantity, quality and activation (Fig. 1A) (12–14). Muscle quantity refers to the amount of available muscle tissue, muscle quality is the amount of force generated per unit of muscle, and muscle activation is the amount of muscle tissue activated during a contraction in relation to total available muscle tissue for that contraction (12–14). In addition, task-specific conditions, such as the speed and type of contraction, and the length of the muscle during the contraction co-determine the force generated (11).
Muscle strength in the general population decreases with age due to degeneration of basic muscle properties (Fig. 1A) (15). Normal ageing is associated with approximately a 1% loss of muscle mass per year from 30 years of age, and this loss tends to accelerate after the age of 70 years (16). Lower muscle quality, resulting from fibre-specific atrophy and infiltration of fat in and around the muscle, further decreases muscle strength in older adults (15). Moreover, muscle activation is lower in older adults as a result of denervation (15).
A number of general factors (Fig. 1B) may be responsible for the changes reported in these basic muscle properties. Systemic, metabolic, and endocrine changes have been linked to muscle weakness (15, 17, 18). Insulin resistance, lower levels of growth hormone, lower levels of sex hormones, and chronic low-grade inflammation in older adults were found to be related to impaired muscle protein synthesis, resulting in muscle weakness (15). Lifestyle-related changes in nutrition (e.g. low protein intake), vitamin status (e.g. vitamin D deficiency), and physical inactivity have also been linked to muscle weakness (15). Finally, the presence of a disease, and related factors, can influence muscle strength (15, 17, 18).
In patients with knee or hip OA, muscle weakness may also be attributed to several OA-specific factors, such as joint degeneration, and the presence of pain and inflammation (Fig. 1C). To date, there is no clear overview of the information on factors associated with muscle strength in knee and hip OA. The framework of a scoping review is recommended for creating an overview of the current state of knowledge and is of major importance for setting future research priorities (19). The aim of this scoping review is to provide an overview of the current state of knowledge on factors associated with upper leg muscle strength in knee and hip OA.
Fig. 1. Hypothetical model of potential determinants affecting muscle strength. CSA: cross-sectional area of the muscle.
A protocol for conducting the scoping review was developed. Where appropriate, aspects of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines were implemented (20).
All literature on the PubMed (MEDLINE) database up to 22 April 2017 was searched systematically. A broad search strategy was chosen to minimize the chance of missing relevant studies. Details of the search strategy are shown in Appendix 1.
Inclusion criteria for the present study were: (i) the study population consisted of hip or knee OA patients; (ii) the study described a relation between a factor and upper leg muscle strength; (iii) the study was performed in vivo; (iv) the study was published in English; and (v) the study was available in full-text. In the present study upper leg muscle strength is defined as all muscles that are responsible for knee or hip movements, including the flexors and extensors of the knee and hip, the hip adductors and abductors, and the hip external and internal rotators. Studies were excluded if: (i) the patient population consisted of patients with hip or knee arthroplasty; or (ii) when exercise therapy was evaluated. However, a study was included when, in addition to exercise therapy, the relationship between a factor and muscle strength was studied separately. For instance, when, in addition to exercise therapy, the association between medication use and muscle strength was studied. Because systematic reviews on the impact of exercise therapy on muscle strength are available, it was decided, a priori, to use reviews to describe the determinant exercise therapy. The systematic reviews were searched with the same search strategy, to which the search filter for systematic reviews was added. In addition, the authors’ own database was searched.
The reference lists in all included studies were checked for additional studies that met the inclusion criteria.
Selection of the studies was performed by 1 reviewer (AdZ). In case of doubt, a second reviewer was consulted (MvdL). Relevant information from all included studies was extracted. When available the adjusted results were extracted from the article. If no adjusted results were presented, the unadjusted results were used. Factors associated with muscle strength are organized in 3 main categories (Fig. 1):
When multiple factors were reported in a study, each factor was added to the most appropriate category.
Appendix 1. Schematic overview of search terms
The literature search resulted in a total of 4,446 hits (Fig. 2). After removing duplicates, 4,245 hits were screened on title and abstract. This resulted in 184 full-text studies that were checked for eligibility, of which 45 studies were included. Reference lists were checked, resulting in 17 additional studies and 3 studies were added from the exercise therapy. In total, 65 studies were included in this review. The basic characteristics of each study are described in Table I.
Fig. 2. Screening for study eligibility.
Table I. Study characteristics
Table I cont.
Muscle quantity. In knee OA patients, smaller cross-sectional area (CSA) of thigh muscles was associated with lower muscle strength in 2 studies (21, 22). In contrast, 1 study showed that quadriceps muscle volume was not associated with knee extensor strength (23). The authors suggested that homogeneity of the sample, type of strength measurements, and not correcting for intramuscular fat may have limited the ability to find associations in this study (23).
Muscle quality. In knee OA, specific muscle strength (i.e. muscle strength expressed per unit of muscle) was reported to be lower compared with controls (21, 24, 25). One study found significantly lower muscle quality in patients with knee OA, as a result of a relative decrease in type 2b and type 1 fibres (but not of other fibre types) (25). Higher fat infiltration in and around the thigh muscles of patients with knee OA was reported (23, 24, 26). Three studies reported that fat infiltration was negatively associated with muscle strength in knee OA (23, 24, 26). In 1 of these studies this association was no longer significant after controlling for covariates (26).
Muscle activation. In knee OA, mixed results were reported on the association between the level of muscle activation and muscle strength. Lower muscle activation in patients with knee OA was reported to be associated with lower muscle strength in 4 cross-sectional studies (21, 27–29). In contrast, 2 other studies found no difference in muscle activation and muscle strength in patients with knee OA compared with age-matched controls (30, 31).
One study reported that patients with knee OA recruit larger motor units and have lower firing rates compared with controls. This resulted in muscle strength that was 22% lower in patients with knee OA compared with controls. However, this difference was not found to be statistically significant (32). Furthermore, the sodium/potassium pump activity, responsible for creating an action potential in muscle cells, was not associated with the observed difference in muscle strength between the group with knee OA and controls (33). Moreover, although co-contraction (i.e. the simultaneous activation of agonist and antagonist muscles) is a proposed mechanism to stabilize the knee joint that may result in a reduction in force output, the presence of co-contraction in patients with knee OA was not associated with a decrease in muscle strength (30). Finally, one experimental study reported that gamma loop dysfunction may contribute to muscle weakness via a decrease in muscle activation in patients with knee OA (34).
The results of a longitudinal study showed that baseline quadriceps activation did not predict changes in muscle strength (29). The change in quadriceps activation over time did, however, predict the change in muscle strength in patients with knee OA following exercise therapy (35).
Muscle quantity. In knee OA patients, smaller cross-sectional area (CSA) of thigh muscles was associated with lower muscle strength in 2 studies (21, 22). In contrast, 1 study showed that quadriceps muscle volume was not associated with knee extensor strength (23). The authors suggested that homogeneity of the sample, type of strength measurements, and not correcting for intramuscular fat may have limited the ability to find associations in this study (23).
Muscle quality. In knee OA, specific muscle strength (i.e. muscle strength expressed per unit of muscle) was reported to be lower compared with controls (21, 24, 25). One study found significantly lower muscle quality in patients with knee OA, as a result of a relative decrease in type 2b and type 1 fibres (but not of other fibre types) (25). Higher fat infiltration in and around the thigh muscles of patients with knee OA was reported (23, 24, 26). Three studies reported that fat infiltration was negatively associated with muscle strength in knee OA (23, 24, 26). In 1 of these studies this association was no longer significant after controlling for covariates (26).
Muscle activation. In knee OA, mixed results were reported on the association between the level of muscle activation and muscle strength. Lower muscle activation in patients with knee OA was reported to be associated with lower muscle strength in 4 cross-sectional studies (21, 27–29). In contrast, 2 other studies found no difference in muscle activation and muscle strength in patients with knee OA compared with age-matched controls (30, 31).
One study reported that patients with knee OA recruit larger motor units and have lower firing rates compared with controls. This resulted in muscle strength that was 22% lower in patients with knee OA compared with controls. However, this difference was not found to be statistically significant (32). Furthermore, the sodium/potassium pump activity, responsible for creating an action potential in muscle cells, was not associated with the observed difference in muscle strength between the group with knee OA and controls (33). Moreover, although co-contraction (i.e. the simultaneous activation of agonist and antagonist muscles) is a proposed mechanism to stabilize the knee joint that may result in a reduction in force output, the presence of co-contraction in patients with knee OA was not associated with a decrease in muscle strength (30). Finally, one experimental study reported that gamma loop dysfunction may contribute to muscle weakness via a decrease in muscle activation in patients with knee OA (34).
The results of a longitudinal study showed that baseline quadriceps activation did not predict changes in muscle strength (29). The change in quadriceps activation over time did, however, predict the change in muscle strength in patients with knee OA following exercise therapy (35).
Physical activity. Lower levels of physical activity have been reported in patients with knee OA (36). Three studies found that avoidance of activities was associated with lower muscle strength (37–39). In contrast, one study reported no association between several measures of physical activity and upper leg muscle strength (40). Negative affect (e.g. low vitality and depression) was directly, and indirectly (via the avoidance of activities), associated with lower muscle strength (37).
In systematic reviews on knee OA, exercise therapy (i.e. an increase in physical activity) was associated with improved muscle strength (41–43). Resistance training led to improvements in upper leg muscle strength of approximately 18% (41, 43). High-intensity resistance training resulted in greater benefits than low-intensity resistance training (43). The quality of the evidence was, however, reduced by the risk of bias and imprecision in the included studies.
Endocrine and metabolic factors. Higher body mass was associated with higher absolute muscle strength in patients with knee OA (30, 44). Two intervention studies (45, 46) reported the result of body weight loss on muscle strength. In both these studies, weight loss resulting from a low-energy diet alone or in combination with exercise, was associated with increased muscle strength normalized for body weight.
Nutrition and vitamins. In 2 studies in patients with knee OA, low levels of vitamin D were found to be associated with lower muscle strength in unadjusted analyses (47, 48). In the study by Koeckhoven et al., the association was no longer significant after adjusting for body mass index (BMI) (48). According to the authors, this may be explained by the lipophilic character of vitamin D, resulting in vitamin D storage in fat tissue. Hence, more adipose tissue (higher BMI) could result in lower levels of vitamin D in serum.
Creatine supplementation was studied in 1 intervention study. No additional increase in muscle strength was found when comparing creatine supplementation plus resistance training with resistance training alone (49). Glucosamine use was investigated in 2 studies, which both failed to find an association between glucosamine use and muscle strength in patients with knee OA (50, 51).
Demographics. Age has been shown to be associated with muscle strength in patients with knee OA in 3 studies (26, 52, 53). In contrast, 2 studies did not find an association between age and muscle strength (33, 54). This may be a result of small sample sizes and limited age distribution of the participants in these studies.
Gender was associated with muscle strength in patients with knee OA (21, 44, 52, 54–56). Women had lower muscle strength compared with men. After normalizing for muscle volume or body weight, the association between gender and muscle strength remained in 2 studies, but only approached significance in one study (21, 44, 52).
Height was associated with extensor strength in one study in patients with knee OA (44).
Joint degeneration. Several cross-sectional studies reported that radiographic OA (ROA) was associated with lower muscle strength in knee OA (21, 24, 26, 28, 31, 57–61). Although in all joint compartments the presence of ROA was associated with quadriceps weakness, the strongest relation was found when a combination of tibiofemoral (TF) and patellofemoral (PF) ROA was present (57, 58). Interestingly, also in asymptomatic patients, ROA was associated with lower muscle strength (58, 62). No association was found between knee joint ROA and hip muscle strength (63–65), except for low hip abductor muscle strength (64).
In addition to the presence of ROA, a higher level of radiographic severity was reported to be associated with lower muscle strength in 5 studies (26, 44, 55, 57, 60), but in one study the association was no longer significant after controlling for confounders (44). Three studies did not find an association between radiographic severity and muscle strength (29, 54, 66). In addition, in a longitudinal study by Ruhdorfer and colleagues (62), an increase in joint space narrowing was not associated with a decrease in muscle function.
Magnetic resonance imaging (MRI) showed bone marrow lesions, cartilage lesions, synovitis and/or effusion, loose bodies, cysts in the anterior cruciate ligament (ACL), and meniscus maceration to be associated with lower extension and flexion strength in patients with knee OA (26, 57, 60, 61, 67). In an exercise intervention study, also using MRI to detect joint degeneration, it was found that PF abnormalities were associated with less improvement in upper leg muscle strength over a 12-week exercise programme (68). The severity of other MRI features was not related to the effect of exercise therapy on muscle strength (68).
Biomechanical factors. In knee OA, deformities of the knee joint have been studied in relation to muscle strength. Surprisingly, greater varus malalignment of the knee joint was associated with higher muscle strength (23, 69). It was suggested that the higher muscle strength may result from a compensatory mechanism to counteract the greater knee abduction moment in patients with malalignment (69). Impaired proprioception and higher joint laxity were found to be associated with lower muscle strength in 2 studies (70, 71), whereas one study did not find an association between proprioception and muscle strength (53).
Skou and colleagues reported that worse self-reported knee confidence, which is a person’s belief as to how troubled they are by lack of confidence in the support of the knee joint, is associated with lower quadriceps strength (72). Similar findings have been reported in a study by Knoop and colleagues for self-reported knee joint instability (73).
Markers of inflammation. In patients with knee OA, systemic inflammatory markers are elevated compared with age-matched controls (74–76). Three studies reported that higher levels of inflammatory markers (serum C-reactive protein (CRP), erythrocyte sedimentation rate (ESR), interleukin 6 (IL-6) level) were associated with lower muscle strength in knee OA (77–79). In 1 study, however, this association was no longer present, after controlling for BMI (77). It was suggested that the effect of BMI on the association of inflammatory markers with muscle strength may be explained by the link between inflammation and obesity. Furthermore, in 2 studies the presence of effusion and synovitis (indicators of a local inflammation), detected by MRI, was reported to be associated with lower muscle strength (57, 61).
One intervention study that targeted inflammation was included. In this study, patients performed a 12-week exercise programme, and those patients with knee OA who received non-steroidal anti-inflammatory drugs (NSAIDs) in addition to the exercise programme reported an increase in muscle strength compared with patients with knee OA who received placebos (51).
Pain. In several studies on knee OA, the presence of pain has been reported to be associated with lower muscle strength (22, 24, 37, 57, 59, 80–82). One study found an association between pain and muscle strength in the quadriceps muscles, but not in any other thigh muscles (22). Petterson and colleagues found no difference in muscle strength between the symptomatic leg and the non-symptomatic leg (21). Steidle-Kloc and colleagues reported low muscle strength in both legs, which was more pronounced in the affected leg (82).
Fitzgerald et al. reported that patients with knee OA using over-the-counter analgesics had lower muscle strength than those not using analgesics (54). In contrast, Scopaz and colleagues found no association between medication use and muscle strength (29). No correction for pain on the association between medication use and muscle strength was performed in either study (29, 54).
In an intervention study targeting pain, injection of either bupivacaine or saline (placebo) in patients with knee OA had similar effects on the reduction in pain, which resulted in an increase in muscle strength in both groups (80). In an intervention study by Shakoor and colleagues, reduction in pain over time was directly associated with an increase in muscle strength in patients with knee OA following an 8-week home exercise programme (83).
The use of hyaluron injections has been associated with a short-term increase in muscle strength in 3 studies involving patients with knee OA (84–86). After hyaluron injections, a significant reduction in knee pain, which is the suggested mechanism for the increase in muscle strength, was reported in 2 studies (84, 85), but was not assessed in the third study (86).
Disease duration. There have been inconsistent findings on the association between the duration of the disease and muscle strength in knee OA. The duration of symptoms was found not to be associated with muscle strength in a study by Pap et al. (28). Scopaz and colleagues did find, however, that time since diagnosis was associated with muscle strength (29). These conflicting findings might be caused by the different definitions used to determine the duration of the disease.
In hip OA, basic muscle properties were studied in 2 studies. Reduction in CSA, a measure of muscle quantity, was associated with lower hip muscle strength by Suetta and colleagues (56). In contrast, Arokoski and colleagues did not find muscle quantity to be associated with muscle strength (3). They suggested that other factors, such as muscle activation or muscle quality, determined hip muscle strength (3). Muscle quality of the quadriceps muscle was reported to be significantly lower in the affected leg compared with the non-affected leg in the study by Suetta and colleagues (56).They found a higher fraction of non-contractile tissue in the affected leg compared with the unaffected leg, resulting in lower muscle quality (56). In addition, they reported that impaired muscle activation was more pronounced in the affected leg, and associated with lower hip muscle strength (56).
Regarding general factors, physical activity and gender were studied in relation to muscle strength in hip OA. In 2 studies, physical activity was found not to be associated with upper leg muscle strength in patients with hip OA (87, 88). However, one study reported a relationship between avoidance of activities and a decrease in muscle strength (38). In a systematic review by Runhaar and colleagues it was shown that, out of the 3 studies on exercise in hip OA, 2 studies found significant improvements in muscle strength (42). In a systematic review by Zacharias, a significant improvement in abduction strength was found after a multi-model approach that included exercise, but no significant effect on hip extension or internal rotation strength was found (43). Male gender was associated with higher muscle strength (56).
From the OA-specific factors, only ROA of the hip joint and pain were studied in relation to muscle strength. In one study, it was found that more severe ROA of the hip joint was associated with lower hip extension and abduction muscle strength (3). In that same study, no association was found between pain and hip muscle strength (3).
The aim of this scoping review was to provide an overview of the current state of knowledge on potential determinants of muscle strength in knee and hip OA. With respect to basic muscle properties (Fig. 1A), there are a limited number of studies with inconsistent findings regarding the relationship between muscle quantity and muscle strength in knee OA (21, 22). More studies are needed to clarify this relationship. However, lower muscle quality was consistently found to be associated with lower muscle strength in knee OA (21, 22, 24–26, 56). Similar findings were reported for the general older population (15). For muscle activation, mixed results have been reported on the association with muscle strength in knee OA (21, 27–31). These conflicting findings may be the result of methodological differences between studies in measuring muscle activation (30). For example, insufficient rests between trials, no verbal encouragement, different knee angles while testing or no warm-up trials could have led to differences between studies. In hip OA, similar findings were reported for the basic muscle properties; however, there is an insufficient number of studies to enable conclusion to be drawn on the associations (3, 56).
A number of general factors were associated with muscle strength in the knee and hip OA population (Fig. 1B). Physical inactivity was associated with lower muscle strength in patients with knee OA (37, 38, 41–43). These findings are in accordance with those reported for the general older population (15). In addition, exercise therapy was found to improve muscle strength in knee OA (41–43). In hip OA, mixed results were found for physical activity (38, 87, 88). A positive effect of exercise therapy on muscle strength has been found in hip OA (42, 43). However, further research is needed to confirm the effect of exercise therapy on muscle strength in hip OA.
Relationships with other general factors were less studied. There are too few studies on the association between factors related to nutrition and vitamins and muscle strength in the knee and hip OA population (47–51). The importance of these factors with respect to muscle strength has, however, been shown in the general older population (15). For instance, food intake is reported to decrease with age, resulting in insufficient caloric and protein intake in the majority of older adults, which contributes to loss of muscle mass and function (15). Similarly, endocrine and metabolic factors (i.e. testosterone, steroid hormone, growth hormone, and body mass) have been associated with muscle strength (15). In patients with knee OA, however, only bodyweight has been studied in association with muscle (30, 44–46). The data suggests that higher bodyweight is associated with higher absolute muscle strength (30, 44). In contrast, a decrease in bodyweight was associated with an increase in muscle strength corrected for bodyweight (30, 44–46). Thus, both higher and lower bodyweight are associated with higher muscle strength. Note that these findings are the result of 2 different measures of muscle strength (absolute and corrected for bodyweight) used in these studies. Bennell and colleagues have stated that strength varies with body size in patients with OA and therefore advise correcting muscle strength for body size (1).
From the OA-specific factors, radiographic severity was a factor associated with lower muscle strength in knee OA (3, 21, 24, 26, 28, 31, 57–60). In hip OA only 1 study reported this association (3). The limited number of studies on biomechanical factors, such as joint proprioception and joint laxity, precluded conclusions on the association with muscle strength (53, 70, 71). Pain is reported to be associated with lower muscle strength in several studies involving patients with knee OA (22, 24, 37, 57, 59, 80, 81), and in one study involving patients with hip OA (3). For interventions targeting pain, including the use of analgesics and injections, inconsistent findings were found in knee OA (29, 54, 80, 84–86). There is some evidence for the association of higher levels of inflammation with lower muscle strength in knee OA (57, 61, 77–79). Both systemic inflammatory markers (e.g. IL-6, ESR and CRP) and indicators of local inflammation (e.g. synovitis or effusion) were reported to be associated with lower muscle strength in patients with knee OA (57, 61, 77–79). In addition, in 2 intervention studies anti-inflammatory medication was associated with an increase in muscle strength in knee OA (51, 89). In the general older population, chronic inflammation is suggested to be a potential contributor to muscle loss (15). Moreover, IL-6 has been shown to negatively affect levels of growth hormone, which are linked to increased lean mass and reduced fat mass (15). In the OA population, higher levels of low-grade inflammation are reported compared with in healthy older adults (74–76). Hence, in the knee and hip OA population the negative effect of systemic and local inflammatory factors on muscle strength might be greater than in the general older population. More in-depth research on the effect of systemic and local inflammation on muscle strength is needed in this population. With regard to the above-mentioned factors associated with muscle strength in knee and hip OA, shared mechanisms, from degenerative processes at the cellular level to pain at the patient level, appear to be involved in the process of muscle weakness.
The findings of the present study suggest that more studies are required to create a clear overview of all factors associated with muscle strength in patients with knee or hip OA. Especially modifiable factors that can be targeted to optimize muscle strength, such as nutrition and vitamins and level of inflammation should be studied in future.
Several points should be taken into consideration for future research. The majority of the included studies had a cross-sectional design, which limits the ability to identify potential determinants of muscle strength. To reveal causality more longitudinal and experimental studies are needed in patients with knee and hip OA. In addition, muscle strength should be reported in both absolute value and the value normalized for body weight, in order to be able to compare values between studies (1). Similarly, the variety of how muscle strength is measured (i.e. isokinetic, isometric or with different test apparatus) in the included studies complicates the comparison of study outcomes and might even result in measuring different aspects of muscle strength per study. In hip OA, there is no consensus on which muscle group should be measured to reflect overall hip muscle strength, in the way that quadriceps strength is commonly used in knee OA. Furthermore, corrections for relevant confounders, such as gender and age, should be performed for adequate interpretation of results. Finally, it should be noted that the literature search to identify factors associated with muscle strength in knee and hip OA was performed in only one database. Although MEDLINE, as one of the largest databases in medical science, is expected to cover the majority of studies, we acknowledge this as a limitation of our study.
In conclusion, lower muscle quality, physical inactivity, more severe joint degeneration, and higher pain have been shown to be associated with lower upper leg muscle strength in knee OA. Future research on knee OA should focus on other potential determinants of upper leg muscle strength, such as lower muscle quantity, muscle activation, nutrition and vitamins, and markers of inflammation. In hip OA, more research is needed on all potential determinants.
This study was funded by the Dutch Arthritis Association. The authors thank R. du Toit for his assistance in correcting the manuscript.


 Click to show fullsize
Click to show fullsize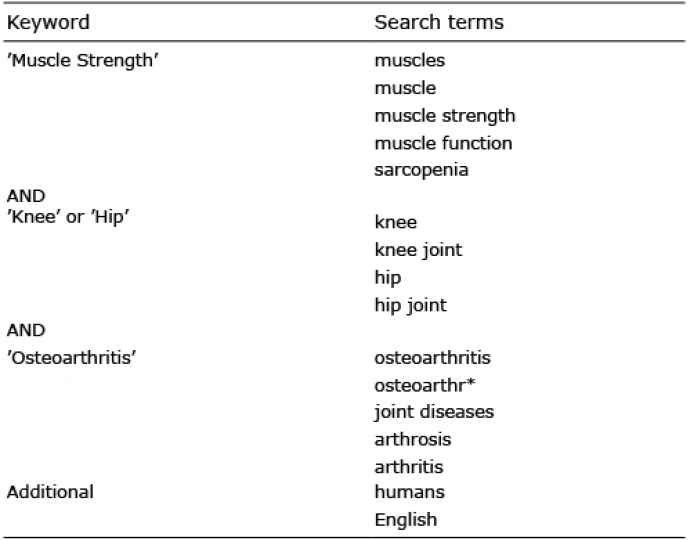 Click to show fullsize
Click to show fullsize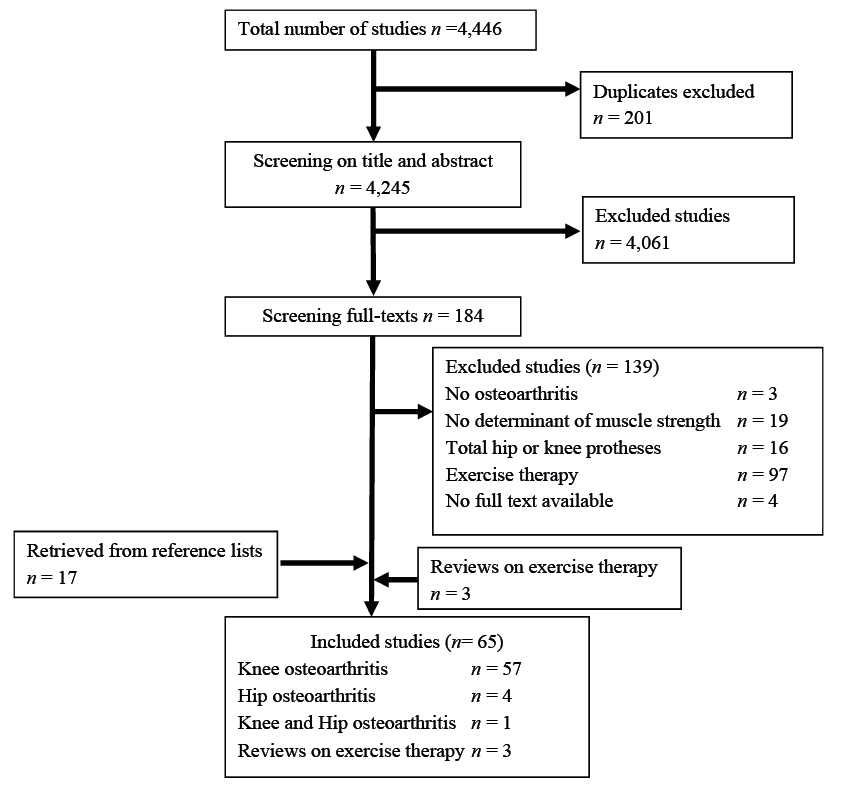 Click to show fullsize
Click to show fullsize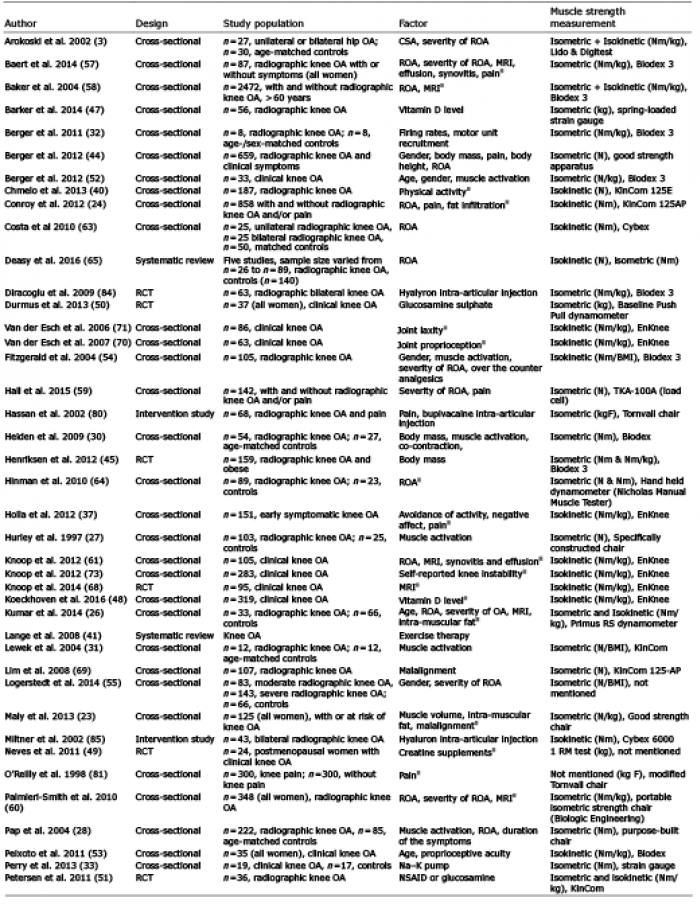 Click to show fullsize
Click to show fullsize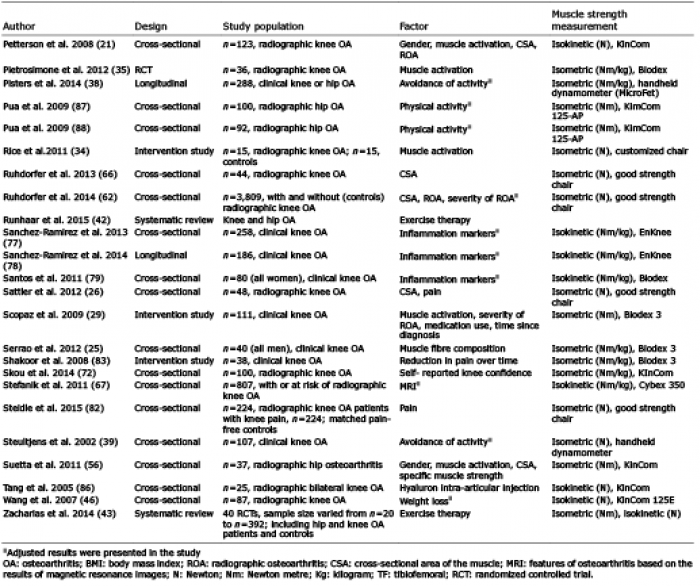 Click to show fullsize
Click to show fullsize