
From the 1Department of Physical and Rehabilitation Medicine, Hacettepe University Medical School and 2Department of Physical Therapy and Rehabilitation, Hacettepe University Faculty of Health Sciences, Ankara, Turkey
Background: Various studies have shown the efficacy of conventional isometric, Pilates and yoga exercises. However, data on the effects and comparison of these specific exercises on the cervical muscle morphology are insufficient or lacking.
Objective: To investigate the effects of different exercise treatments on neck muscles in patients with chronic neck pain.
Design: A randomized study.
Methods: Fifty-six patients with chronic neck pain were randomized into 3 groups as follows: Pilates group (n = 20), yoga group (n = 18) and isometric group (n = 18). Demographics and background information were recorded. The thickness and cross-sectional area of neck muscles were evaluated by ultrasound imaging. Cervical motions were measured with a goniometer. Pain severity was evaluated with the McGill Pain Scale, disability with the Neck Disability Index, quality of life with the Nottingham Health Profile, and emotional status with the Beck Depression Inventory. In addition to a conventional physiotherapy programme, 15 sessions of physical therapy, including hot pack, ultrasound, and transcutaneous electrical nerve stimulation (TENS), were provided to all patients. All groups performed the exercises for 6 weeks. The aforementioned assessments were performed before and 6 weeks after the treatment.
Results: Although pain, disability, depression and quality of life improved similarly within all groups (all p < 0.05), muscle thickness values as regards the semispinalis capitis were increased only in the Pilates group (p = 0.022).
Study limitations: The lack of complex (progressive resistive) exercise treatment protocols, short treatment duration and partial supervision.
Conclusion: All 3 types of exercise had favourable effects on pain and functional scores, but no differences were found among the groups, except for the Pilates group, in which the semispinalis capitis muscle increased in thickness.
Key words: neck pain; exercise; yoga; Pilates; ultrasound.
Accepted Sep 28, 2017; Epub ahead of print Nov 16, 2017
J Rehabil Med 2018; 50: 00–00
Correspondence address: Naime Uluğ, Hacettepe Üniversitesi Tıp Fakültesi Hastaneleri Zemin Kat FTR AD Sıhhıye, Ankara. E-mail: ulugnaime@gmail.com
Chronic neck pain is a major public health problem in western society (1, 2). In the general population, 71% of adults are affected by neck pain at some time in their life, and its annual prevalence in the general and working population varies between 30% and 50% (3).
The neck extensor muscles (from superficial to deep: trapezius, splenius capitis, semispinalis capitis, semispinalis cervicis and multifidus) connect the head/neck to the trunk. Postural control requires passive muscle properties for support/protection against non-physiological joint translations/overstretching, whereas broad-range movement necessitates muscular flexibility (4).
Exercise is one of the most important components of rehabilitation programmes for patients with neck pain (5, 6). Studies indicate that different exercise programmes including low load endurance, scapular muscle re-training, cervical, scapulothoracic and upper quarter strengthening or stretching are mostly used for management of chronic neck pain (5, 7–9). Recently, Pilates and yoga have also been included in this list (10, 11). Pilates and yoga comprise a physical and mental focus using breathing control, postural alignment and flexibility through various exercises. Pilates emphasizes core stability and postural alignment, while yoga includes specific postures, movement sequences, relaxation and meditation (11).
Structural changes, including increased fat in the muscle and variable cross-sectional area (CSA), have been detected in the deep cervical extensors of the patients with chronic neck pain (4). Although exercise has shown efficacy in activation of the cervical flexors and in reducing pain (8), cervical extensors might be equally important for the management of chronic neck pain. Herein, although various studies have shown the efficacy of conventional isometric, Pilates and yoga exercises; data as regards the effects (and comparison) of these specific exercises on the cervical muscle morphology is insufficient or lacking.
The aim of this study was to explore the clinical and morphological effects of isometric, yoga and Pilates exercises on neck muscles in patients with chronic neck pain. For this, ultrasound (US) imaging, which has proven to be a reliable, convenient, inexpensive and radiation-free tool, was used for the evaluation of neck muscles (12, 13).
Local institutional ethics approval was obtained from Hacettepe University Medical School for this prospective randomized study. The study was conducted between March 2015 and April 2016. Subjects aged 18–50 years and who had chronic neck pain (> 3 months of duration) were enrolled in the study. Those with a history of cervical spine surgery, cervical trauma, central nervous system diseases, cervical radiculopathy, acute inflammation and malignancy were excluded. Overall, a total of 60 subjects were randomly assigned into 3 exercise groups: Pilates, yoga and isometric. Demographic data, including age, sex, body mass index (BMI) and duration of pain, were recorded.
All of the assessment procedures were performed by the same physiotherapist (NU) who was blinded to the US measurements.
The Turkish version of the Short-Form McGill Pain Questionnaire (SF-MPQ) (14) was used to assess pain severity and related features. It consists of 11 items in the sensory dimension and 4 items in the emotional dimension. Patients have to identify their pain quality as none, mild, average, or severe. The sensory and affective scores are calculated by adding the sensory and affective intensity scores. The total score is the sum of the intensity scores. SF-MPQ also includes a visual analogue scale (VAS) for measuring the severity of pain. The total score is evaluated using a 6-point Likert-type scale (0 = no pain to 5 = intolerable pain).
The Turkish version of Nottingham Health Profile (NHP) (15) was used to measure the patients’ quality of life (QoL) from their own perspectives. This scale has 6 dimensions including 38 questions. It evaluates pain, physical mobility, emotional reactions, energy, social isolation and sleep. A higher score shows worse influence of QoL.
The Turkish version of the Neck Disability Index (NDI) (16) was used to assess disability. Active neck range of motion (ROM) was measured with a universal goniometer in the sitting position. The Turkish version of the Beck Depression Inventory (BDI) (17) was used to measure the presence and level of depression.
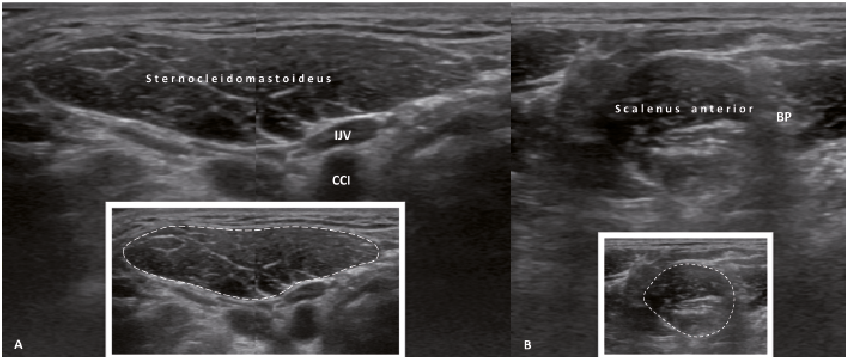
Muscle size measurements were performed using a 5–12 MHz linear probe (Logiq P5, GE Medical System, Milwaukee, WI, USA). All measurements were performed by the same physiatrist (LÖ), with >15 years of experience in musculoskeletal US imaging, who was blinded to the clinical data (Figs 1 and 2). CSA of scalenus anterior and sternocleidomastoideus (SCM) muscles (Fig. 1) and thicknesses of trapezius, semispinalis capitis and splenius capitis muscles (Fig. 2) were measured bilaterally in the sitting position.
Fig. 1. (A) Split-screen axial and (B) axial ultrasound views show the cross-sectional area measurements of the sternocleidomastoid and scalenus anterior muscles respectively. IJV: internal jugular vein; CCA: common carotid artery; BP: brachial plexus.
Fig. 2. (A) Longitudinal and (B) axial ultrasound views show the thickness measurements of the trapezius, splenius capitis and semispinalis capitis muscles, respectively.
After the initial assessment of the patients, all exercise groups received their exercise programme from a single physiotherapist (NU), using a written and photographic description. Patients were also supervised for the first 3 weeks (home-based thereafter). Before exercise training, all study groups were given information about chronic neck pain, the anatomy of the spine and postural alignment. Pilates exercises were applied in the first group, yoga exercises in the second group and conventional isometric exercises in the third group for 6 weeks. All the assessment procedures were repeated at the end of the sixth week.
In addition to the exercises, each group received physical therapy (5 days in a week, a total of 15 sessions over a period of 3 weeks) for neck pain, including hot pack, ultrasound and conventional transcutaneous electrical nerve stimulation (TENS).
In the first teaching session, patients were taught how to activate their deep abdominal muscles (transversus abdominis and multifidus). Some visual imagery, verbal cueing or demonstrations were used as facilitation methods. Five key elements of Pilates (18): lateral costal breathing, centering (pelvic placement), ribcage placement, shoulder blade placement, head and neck placement, were taught.
Four Pilates beginner mat exercises, including double-leg stretch level, shoulder bridge level, arm openings level and breast stroke level (18–20), were taught and patients were encouraged to perform these exercises in 2 sets of 10 repetitions per day. They were also told to pay attention and protect the neutral spine alignment and perform breathing control during all the exercises.
Four exercises from Iyengar Yoga asanas: Adho Mukha Virasana, Tadasana, Virabhadrasana and Chair Bharadvajasana (10, 21), were taught to the patients. They were told to maintain each yoga posture starting from at least 10–20 s in the following days. They were encouraged to do these exercises in 2 sets of 10 repetitions per day.
In the sitting position, the patients were instructed to place their hands firstly on the front (then the other sides) of their heads and push forward, but resist any movement of the head while maintaining the head and neck in the neutral position for 5 s. They were encouraged to do these exercises in 2 sets of 30 repetitions per day.
Data analysis was conducted using SPSS 21.0 package version. Distribution of data was evaluated using the Kolmogorov–Smirnov test. Comparison of the demographic characteristics was analysed using analysis of variance (ANOVA) for numerical data and χ2 or Fisher’s exact test for categorical data. For comparison of the dependent variables within the groups; paired t-test or Wilcoxon test was used, where appropriate. To determine which group was more effective, improvement ratios (%) ((after treatment value – baseline value)/(baseline value)× 100) with ANOVA/Student’s t-test (for parametric data), or Kruskal–Wallis/Mann–Whitney U test (for non-parametric data) were used. Bonferroni post-hoc analysis was performed to determine whether there were statistically different variables among the 3 groups. However, no adjustment/correction was performed for multiple comparisons among the number of outcome variables that were tested. A p-value < 0.05 was accepted as statistically significant.
The sample size was determined from the pilot study, whereby 5 subjects were used in each group. The difference in the thickness of the semispinalis capitis muscle between maximum and minimum change variation was determined. The mean difference was 0.17 cm and standard deviation was determined to be 0.12 cm. Using these data, for desired power of 90% and with 0.10 type I error, the sample size was generated as 15 subjects in each group to determine the difference among the 3 groups. However, taking into consideration the possible drop-outs, 20 subjects were included in each study group.
Sealed envelopes were used, which were opened immediately prior to intervention after the participant consented to be a part of the study. They were then randomized using the sealed envelope method and divided into 3 groups of 20 patients. Sixty envelopes were used and equally numbered with group names 1 (Pilates), 2 (yoga), and 3 (isometric). The patients were asked to choose 1 of these sealed envelopes. The CONSORT (Consolidated Standards of Reporting Trials) flow diagram of the study is shown in Fig. 3.
Fig. 3. CONSORT (Consolidated Standards of Reporting Trials) flow diagram of the study.
Two patients in the yoga group and 2 in the isometric group could not complete the study. Therefore, results from a final total of 56 patients (47 females, 9 males) were analysed. Clinical data for the patients are shown in Table I. There was a difference between the groups regarding age (p < 0.05). Subgroup analysis showed that age was higher in the isometric group than in the yoga group. The other data, including sex, body mass index and pain duration, were similar among the groups (all p > 0.05).
Table I. Clinical characteristics of 56 patients with chronic neck pain in 3 exercise groups
The US measurements are shown in Table II. Since values for both sides were statistically similar (all p > 0.05); right and left CSA and thickness values were analysed together. Overall, the semispinalis capitis muscle thickness increased significantly only in the Pilates group (p < 0.05). However, there were no differences between the 3 groups in terms of improvement in US measurements.
Table II. Comparison of the ultrasonographic measurements of the neck muscles
Active ROMs were increased after treatment within all groups (all p < 0.001). SF-MPQ scores are shown in Table III. After treatment, improvements were found in all subscores of the SF-MPQ in all groups (all p < 0.001). The NDI (all p < 0.001) and BDI (all p < 0.05) scores of the patients decreased in all groups after treatment (Table IV). Overall, no differences were found between the 3 groups in terms of improvement in ROM, SF-MPQ, NDI and BDI scores (all p 0.05).
Table III. Comparison of short form-McGill pain questionnaire (SF-MPQ) subscores for the 3 exercise groups in patients with chronic neck pain
The NHP scores are shown in Table V. Although the total scores of NHP decreased within all groups (all p < 0.01), there were no differences among the groups in these improvement ratios (p > 0.05). According to NHP subscores, energy level (within the Pilates and yoga groups), sleep scores (within the yoga and isometric groups) and pain scores (within all the groups) improved significantly (all p < 0.05). However, none of the groups had better improvement than the other(s) (p > 0.05).
Table IV. Neck Disability Index (NDI) and Beck Depression Index (BDI) scores for the 3 exercise groups in patients with chronic neck pain
Table V. Comparison of Nottingham Health Profile (NHP) scores
This study investigated the beneficial effects of conventional isometric, yoga and Pilates exercises on neck muscles and on pain, disability, depression (emotional state) and QoL in patients with chronic neck pain. While pain, disability, depression and QoL improved similarly within all groups, muscle thickness of the semispinalis capitis muscle, was increased only in the Pilates group.
Previous studies have shown that exercise is an effective and appropriate treatment for neck pain (5, 6). Meta-analyses suggest that therapeutic exercise for cervical dysfunction is most effective when it includes stretching, strengthening, and proprioceptive exercises for the neck and shoulder (6, 22, 23). People with chronic neck pain also/often prefer alternative or complementary methods for pain relief, as they do in other chronic painful condition (11). In this regard, Pilates and yoga have gained popularity in community wellness classes and, recently, in physiotherapy treatment and post-rehabilitation transition (24, 25). Evidence indicates that both Pilates and yoga contain cervical, scapulothoracic and upper quarter strengthening and stretching components for treatment of chronic neck pain (7). Thus, we included these 2 methods in addition to our conventional regimen of isometric exercises.
While there are many data showing the effectiveness of these exercises for low back pain, studies investigating their effects on chronic neck pain have been published recently (11, 19). However, their effects on muscle morphology (i.e. size or thickness) have not been explored using US until now. There is a single study that has investigated the effects of cranio-cervical and cervical flexion exercises on longus colli and SCM muscle dimensions (using US), which found that the muscle dimensions were significantly increased (26).
After a programme of 6 weeks of exercise (3 weeks supervised, 3 weeks home-based), the current study found a significant increase in the thickness of the semispinalis capitis muscle only in the Pilates group. Other muscles measured were the SCM, scalenus anterior, splenius capitis, trapezius and semispinalis capitis. The fact that 2 muscles increased in size in the aforementioned study, but that we could not demonstrate a similar increase in the sizes of other muscles in our study, may be related to the longer durations of exercises and of supervision (10 weeks) in the earlier study. In addition, the fact that progressive resistive exercises were applied in the earlier study would have further increased this size effect.
The semispinalis capitis is a massive, long cervico-thoracic muscle, which functions as the main head and neck extensor muscle. It originates from the skull and courses down to the lower cervical (C3–C7) and upper thoracic vertebrae (T1–T6) (27–29). Providing a long lever arm, it is functionally highly important and thus the favourable impact of Pilates exercises on this muscle should be noteworthy. By strengthening the trunk stabilizer muscles, Pilates exercises may help to improve body movement patterns (30). In addition, they contain closed kinetic chain exercises that include compressive and decompressive forces, which help the nutrition of joints and cartilage and reduce degeneration (31). Therefore, Pilates may play a role in alleviating chronic musculoskeletal pain caused by spinal instability (32).
The beneficial effects of Pilates and yoga exercises on pain and related disability have been shown previously (11, 19, 21, 33–35). Our results were in accordance with those studies showing improvement in the outcome as regards QoL, pain, disability and depression after 6 weeks.
This study has some limitations: the lack of complex (progressive resistive) exercise treatment protocols, short treatment duration and partial supervision. The underlying reasons for these limitations were the difficulty of complex exercises in patients with neck pain and the fact that the study group comprised only outpatients.
In conclusion, a semi-supervised 6-week programme of Pilates exercises increases the semispinalis capitis muscle thickness. Secondly, all 3 exercises (Pilates, yoga and isometric neck strengthening) exert favourable effects on pain neck ROM, disability, depression and QoL in patients with chronic neck pain. Last, but not least, US imaging may be useful for the convenient assessment and follow-up of various neck muscles under physical/exercise treatment.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize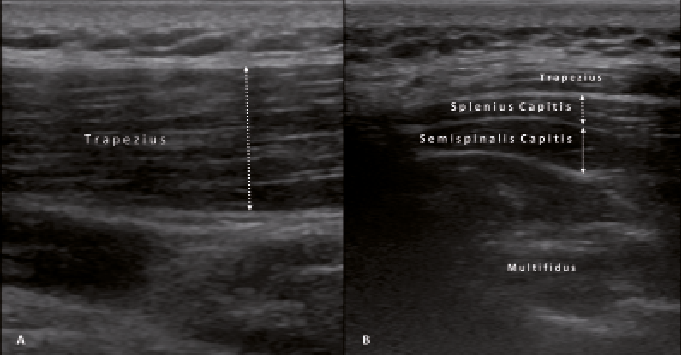 Click to show fullsize
Click to show fullsize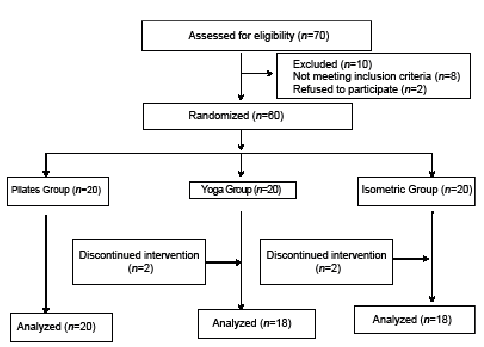 Click to show fullsize
Click to show fullsize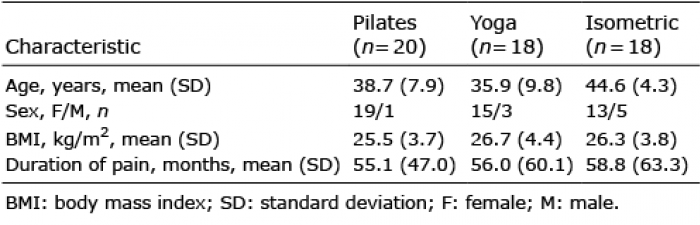 Click to show fullsize
Click to show fullsize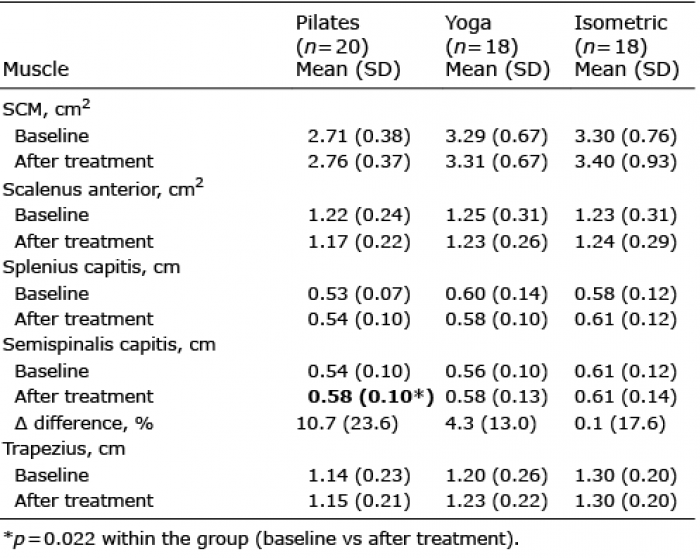 Click to show fullsize
Click to show fullsize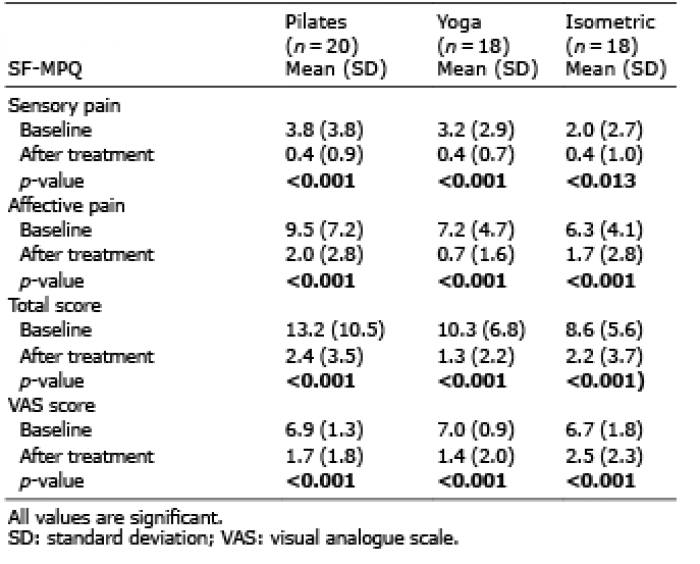 Click to show fullsize
Click to show fullsize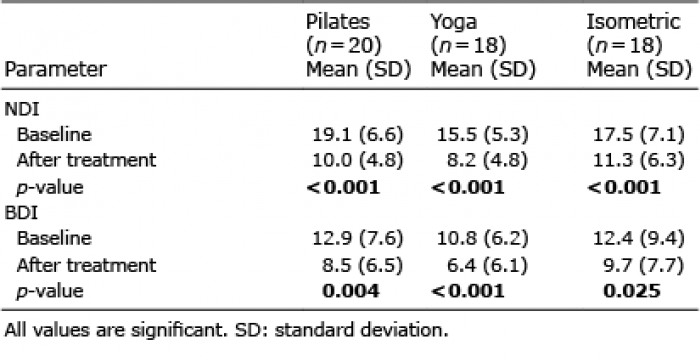 Click to show fullsize
Click to show fullsize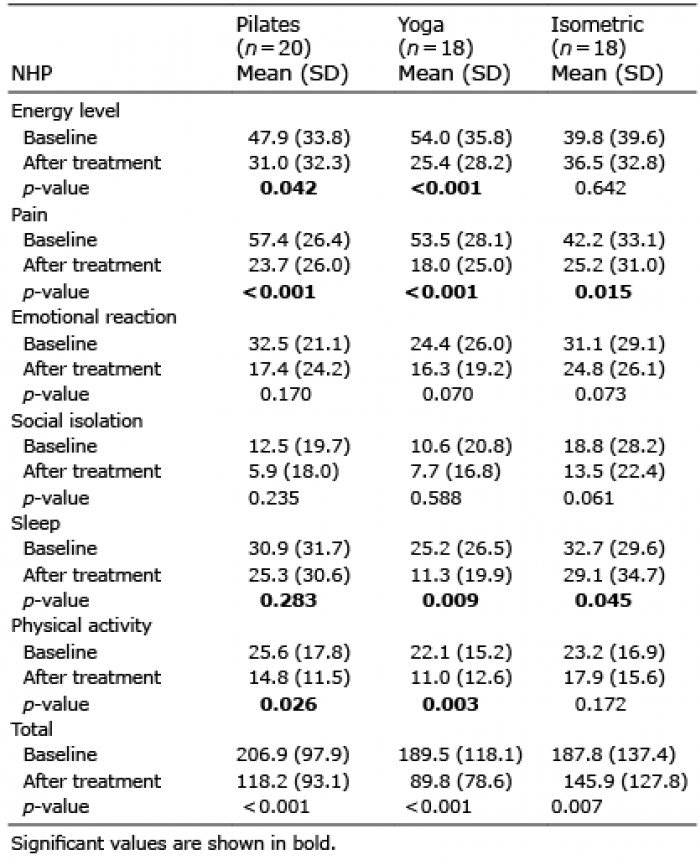 Click to show fullsize
Click to show fullsize