
From the 1University of Huddersfield, School of Human and Health Sciences, Department of Health Sciences, Health and Rehabilitation Division and 2University of Salford, School of Health Sciences, Salford, UK
Objective: To compare the randomized controlled trial evidence for therapeutic effects on walking of functional electrical stimulation and ankle foot orthoses for foot drop caused by central nervous system conditions.
Data sources: MEDLINE, CINAHL, Cochrane Central Register of Controlled Trials, REHABDATA, PEDro, NIHR Centre for Reviews and Dissemination, Scopus and clinicaltrials.gov.
Study selection: One reviewer screened titles/abstracts. Two independent reviewers then screened the full articles.
Data extraction: One reviewer extracted data, another screened for accuracy. Risk of bias was assessed by 2 independent reviewers using the Cochrane Risk of Bias Tool.
Data synthesis: Eight papers were eligible; 7 involving participants with stroke and 1 involving participants with cerebral palsy. Two papes reporting different measures from the same trial were grouped, resulting in 7 synthesized randomized controlled trials (n= 464). Meta-analysis of walking speed at final assessment (p = 0.46), for stroke participants (p = 0.54) and after 4–6 weeks’ use (p = 0.49) showed equal improvement for both devices.
Conclusion: Functional electrical stimulation and ankle foot orthoses have an equally positive therapeutic effect on walking speed in non-progressive central nervous system diagnoses. The current randomized controlled trial evidence base does not show whether this improvement translates into the user’s own environment or reveal the mechanisms that achieve that change. Future studies should focus on measuring activity, muscle activity and gait kinematics. They should also report specific device details, capture sustained therapeutic effects and involve a variety of central nervous system diagnoses.
Key words: electric stimulation therapy; foot orthoses; walking; foot drop; central nervous system; therapeutic effects; systematic review; meta-analysis.
Accepted Sep 29, 2017; Epub ahead of print Nov 17, 2017
J Rehabil Med 2018; 50: 129–139
Correspondence address: Sarah Prenton, Room RG/23, Ramsden Building University of Huddersfield, Queensgate, Huddersfield, West Yorkshire, HD1 3DH Huddersfield, UK. E-mail: s.prenton@hud.ac.uk
Foot drop is a common motor impairment associated with many central nervous system (CNS) conditions (1). An estimated 20–30% of stroke survivors experience foot drop; thus approximately 240,000–360,000 people might be living with it in the UK alone (2). Foot drop is an abnormal activation of the musculature of the lower limb, resulting in inefficient foot clearance during swing (3) and reduced stability in stance (4). These impairments negatively impact the function of walking, which may restrict participation in many aspects of life.
There are 2 demonstrably effective orthotic interventions for foot drop: ankle-foot orthoses (AFO) (5–9) and functional electrical stimulation (FES) devices (10). AFOs address foot drop by changing the effective stiffness and neutral point of the ankle joint (11). FES devices stimulate lower motor neurones, in this case the common peroneal nerve, to assist muscle contraction over appropriate phases in the gait cycle (12).
Recent randomized controlled trials (RCT) have sought to compare the direct effects of using each device on various walking behaviours (13, 14). These comparisons have been made both with and without the devices being worn, at the point of provision and at various time-points after a period of use (15). Clinically the devices are commonly prescribed as orthotics for long-term use (16); the difference between walking behaviours without the device at baseline and walking with the device being worn after a period of use is called the combined-orthotic effects (14). RCTs (14, 17–19) reporting these effects have found that both devices achieve the same improvement at various time-points up 12 months (18). The combined results of individual RCTs, demonstrating equal combined-orthotic effects of AFO and FES, have also been confirmed in a recent meta-analysis (15). However, given the clinical importance of attempting to achieve therapeutic benefits (20, 21) (i.e. improvement in measured walking behaviours without a device being worn relative to baseline, called the therapeutic effects (13)), further work is required to establish whether there are differences in the therapeutic effects of the 2 devices.
The first study of FES reported that some users, following a period of use, experienced improvement even after the device was removed (22). More recently, a number of studies have suggested a range of possible peripheral and central neural mechanisms to explain these observations (23–26). In contrast, an AFO is a purely mechanical device and there appears to be an assumption that the effects of AFO on walking are seen only when the device is worn (27). In addition, some studies suggest that AFO use may lead to muscle weakening (4, 28–31), whereas FES has been suggested to improve volitional muscle activation (25).
These studies appear to predict differential therapeutic effects between the 2 devices, which makes the findings (18) of an equivalent combined-orthotic effect of the devices somewhat surprising; as one might expect improvements in therapeutic effects to be positively correlated with combined-orthotic effects. Therefore a review of therapeutic effects is needed to help inform guidelines for clinical use.
While a number of AFO- and FES-specific reviews have been published, only 2 of these have attempted to draw direct comparisons (16, 32). RCT-based direct comparisons are particularly important as they summarize current thinking about mechanisms-of-effect and how these impact on function. This information can then be used to advance clinical guidelines, which is timely in the face of increasing market choice for both devices. However, neither of the existing reviews (16, 32) could be considered a gold standard meta-analysis, due to methodological issues, and hence there remains a need to pool RCT-level evidence to answer the following specific questions:
1. Are the therapeutic effects on the function of walking for CNS foot drop different for FES and AFO?
i) Does diagnosis impact these therapeutic effects?
ii) Does time of use impact these therapeutic effects?
2. What are the mechanisms of therapeutic effects of AFO and FES on walking for CNS foot drop?
By answering these questions this review aims to guide clinical decision-making and the direction of future research.
In line with best practice the full review protocol was developed a priori and registered with PROSPERO (http://www.crd.york.ac.uk/PROSPERO/display_record.asp?ID=CRD42015025967).
Eight electronic databases were searched: MEDLINE (EBSCO), CINAHL (EBSCO), Cochrane Central Register of Controlled Trials (CENTRAL), REHABDATA, PEDro, NIHR Centre for Reviews and Dissemination, Scopus and clinicaltrials.gov. Search terms included “walking”,”electric* stimulat*”, equinovarus and Nervous system disease* ; The full search strategy is available from the lead author (SP).
One reviewer (SP) assessed titles and abstracts against the inclusion criteria (Table I) and those deemed potentially relevant were considered by 2 independent reviewers (SP and PO). Any disagreements or ambiguity were resolved through discussion with a third reviewer (LK).
A pre-designed pro forma was used to extract data about the characteristics of the included trials, participants and intervention details. Trial authors were contacted by SP if data were not readily available (Appendix I).
Appendix I. Unpublished data from trial authors
The Cochrane Risk of Bias Assessment Tool (33) was used independently by the 2 reviewers (SP and PO), with a third reviewer (LK) available if necessary. In order not to disadvantage authors who did not respond to information requests, risk of bias was based only on published work. It is not possible to blind participants to which device they are given during the trial; therefore the performance bias criterion was removed. A post hoc sensitivity analysis was undertaken if 3 or more trials showed a high risk of bias, in which the meta-analysis was recalculated with those trials temporarily excluded to check whether they had influenced the results.
A range of outcome measures could evidence therapeutic effects; therefore any measure that captured walking behaviours when a device was not being worn following a period of use was extracted (Table I). In order to compare the therapeutic effects on the function of walking (question 1), measures that sat within the Activity or Participation domains of the World Health Organization’s (WHO) International Classification of Functioning, Disability and Health (ICF) model (34) were extracted. Activity monitoring was identified as the primary functional outcome measure (question 1) because, unlike more controlled functional walking measures, it captures actual performance (35, 36) as opposed to potential capacity (37).
Table I. Inclusion criteria
Although foot drop manifests itself in the same way for all CNS disorders, the possible impact of diagnosis on therapeutic effects (question 1i) was explored by performing, where possible, sub-group analysis on individual CNS pathologies. This aimed to provide specific clinical guidance regarding which patients may benefit most from which device.
The time course of therapeutic effects (question 1ii) was explored by pooling data from trials that compared the devices at similar time-points. Some authors suggest that a period of use of 3 months is required to observe any therapeutic effects of either device (24). Sub-group meta-analysis was therefore sought at 12–13 weeks, as an approximation of 3 months.
In order to evidence potential mechanisms-of-effect (question 2), measures reflecting the Body Functions and Structures (BFS) domain are required (38). Given the assumption that FES, but not AFO, has a therapeutic effect on volitional muscle activity, electromyography (EMG) was chosen as a primary BFS measure of interest. As another key measure of gait (quality) is its kinematics (39), which may be influenced by muscle activations in complex ways, we chose to complement the EMG analysis with gait kinematics as a second primary BFS measure. Any other walking measure was deemed secondary and categorized as a functional measure of walking or BFS measures by SP, using appropriate literature (34, 37, 40, 41). All primary and secondary end-point data were extracted.
Where possible, mean differences (MD) with 95% confidence intervals (95% CIs) were used, where outcome measurements were comparable. If data collection methods varied then standardized mean differences (SMD) with 95% CIs were used. RevMan 5.3® software was used.
Visual inspection of forest plot, χ2 test and I2 statistic were used to examine heterogeneity. Low heterogeneity (< 50%) resulted in a fixed-effects and high (> 50%) in a random-effects model being used.
Where meta-analysis was not possible a narrative summary of the overall effects was presented.
A total of 1,725 possible citations were found as a result of the searches. Following title, abstract and full-paper screening, a total of 8 papers met the inclusion criteria. Two of these papers (42, 43) reported results from the same trial, and so were grouped and referred to by the first publication date (42), resulting in 7 RCTs, which included a total of 464 participants (Fig. 1).
Fig. 1. Flowchart of trial selection. RCT: randomized controlled trial; FES: functional electrical stimulation; AFO: ankle foot orthosis.
Six (14) of the 7 trials had a parallel-group RCT design. The remaining trial had a cross-over design with 2 AFO arms. Only 1 AFO arm was used, to avoid any issues associated with multiplicity (44); arm 2 (AFO-FES) was chosen due to its larger size and comparability to the FES arm (arm 1, FES-AFO) and final assessment data was deemed to be at 6 weeks, pre-cross-over (45), given the carry-over observed by the trial authors (46). Two trials collected data from multiple sites (14, 17), with the other 5 based at a single site (Table II).
Mean age ranged from 8 (47) to 61.58 (17) years, all participants had unilateral foot drop with an even distribution of right and left foot drop (182 right, 50.3%, and 180 left, 49.7%). Where reported, more men than women were recruited (262 men, 62%, and 159 women, 38%).
Although Van der Linden et al. (47) included participants with cerebral palsy (CP) (n = 14), the majority of participants (n = 450) had had a stroke (Table II). This allowed for sub-group analysis of this pathology (question 1i). There were no trials that included any progressive CNS diagnoses. Medication was considered by 2 trials (Table II) (14, 17), with 1 screening based on no expected change in medication during the intervention period (14); compliance with medication was not reported by this trial.
Table II. Characteristics of included trials, participant and intervention details
Three trials (14, 17, 42) used “customized” AFOs that were either made or modified for the participant, by an appropriate clinician, on inclusion to the trial (Table II). Participants in 2 of the other trials used a variety of different types of AFO (29, 47) and participants in another trial used off-the-shelf orthoses (48), which was appropriate for the acute/sub-acute population they investigated (49). Four trials recruited participants who did not already use an AFO (12, 14, 42, 48), while the other trials recruited current AFO users (17, 29, 47). None of the trials reported any of the mechanical properties of the AFO (Table II).
All trials recruited new users of FES. One trial used an implantable FES system (29), while the others opted for surface systems from 3 different manufacturers. Set-up parameters were reported by only one trial (47) (Table II).
Four trials allowed use within the home/community setting (14, 17, 29, 47), whilst the remaining 3 trials provided devices only under supervision (12, 42, 48) (Table II).
Table III shows the results of the Cochrane Risk of Bias Assessment. Kluding et al. (17) and Van der Linden et al. (47) were deemed to have no areas of high risk with Kottink et al. (29) showing the most high risk areas (three). Selection bias, as determined by the ability to generate an appropriately random sequence (33), was the area of risk least well addressed by the included trials (Table III). Based on these findings the trials were deemed to be at a moderate or lower risk of bias overall.
Table III. Risk of bias
All 7 trials used outcome measures that could be categorized as functional and BFS (Table IV). Four of the trials utilized measures that we had deemed to be of primary interest (17, 29, 42, 47). The most commonly used secondary measure was walking speed, which was primarily captured over 10 m. This was captured by 6 trials (12, 14, 17, 29, 42, 48) (n = 450).
Table IV. Walking outcome measures and therapeutic effects
Therapeutic effects – meta-analysis of gait speed
Salisbury et al. (48) reported data that reflected orthotic and therapeutic effects in combination. Despite repeated communication no specific therapeutic data was shared and so their results could not be included in meta-analyses. Meta-analysis of final-assessment walking speed data (Fig. 2a) of the other 6 trials (n = 437) showed that both interventions had equivalent positive therapeutic effects (MD = 0.02 [–0.03, 0.06]: I2 0%; p = 0.46). A sensitivity analysis was undertaken excluding the 3 trials (12, 29, 42) that showed high risk of bias (Table III) with regards random sequence generation (selection bias). This showed no significant impact. Positive between-group comparability was also true for the stroke-specific analysis (question 1i) (n = 423) (MD = 0.02 [–0.03, 0.07]: I2 0%; p = 0.54) (Fig. 2b).
Sub-group analysis of walking speed was not possible at 12–13 weeks (question 1ii), as 1 of the 4 trials (17, 29, 43, 48) that collected at this time-point, Kluding et al. (17), were contacted by the lead author but could not access their unpublished AFO data and, as previously stated, Salisbury’s (48) data was not in an accessible format. Five trials (12, 14, 17, 29, 48) collected walking speed data at 4–6 weeks (n = 116); meta-analysis of 3 of those trials (12, 14, 29) at this time-point showed a positive therapeutic effect with between-group comparability (MD = 0.03 [–0.06, 0.12]: I2 0%; p = 0.49) (Fig. 2c). Kluding et al. (17) and Salisbury (48) could not be included in the analysis due the aforementioned lack of access to data.
Fig. 2. (a) Final assessment of 10-m walking speed (m/s). (b) Sub-group analysis of 10-m walking speed for stroke (m/s). (c) Sub-group analysis of 10-m walking speed at 4–6 weeks (m/s).
Two trials monitored activity levels by collecting the mean number of steps taken per day, the primary functional measure identified to evidence therapeutic effects on walking (question 1) (17, 42). Kluding et al. (17) found equal improvement over the period of use (AFO group 1,891 steps/day at week 6 to 2,069 steps/day at week 30; FES group 2,092 steps/day at week 6 to 2,369 steps/day at week 30), whereas Sheffler et al. (42) found an equal lack of improvement (3,270 ± 2,947 steps/day at baseline to 4,038 ± 2,848 steps/day at 24 weeks post device use for AFO vs 3,223 ± 3,134 to 3,738 ± 3,211 steps/day for FES). These could not be meta-analysed due to the lack of data spread reported and because activity was monitored during the intervention period by Kluding et al. (17). Given that it was therefore not clear whether activity monitoring was performed with or without the devices being worn, the ability to interpret the outcome of activity monitoring is very limited.
With regards the mechanisms-of-effect (question 2), only 1 trial collected EMG data (29) (Table IV). This trial calculated the root mean square during static maximum voluntary contraction (RMSmax) of a filtered EMG signal and found that FES enhanced volitional activity of the tibialis anterior (TA), whereas AFO did not. This between-group difference was significant when the knee was extended (p = 0.006), after 26 weeks’ use. The same was true for the gastrocnemius (GS) when the knee was in flexion (p = 0.002) and extension (p = 0.035), after 26 weeks’ use. The RMS of TA during swing (RMSswing) was found to significantly decrease for the AFO group (p = 0.036) with no change for the FES group, after 26 weeks use.
Two trials captured kinematic data (43, 47), but each collected different parameters (Table IV). Sheffler et al. (43) found a comparable lack of effect on most measures, but an equal decrease in peak DF during swing after the 12-week device use period (p = 0.002). This equal decrease in peak dorisflexion (DF) was again found 12 weeks after participants had finished using either device (p = 0.0001). When measured for the final time 24 weeks after participants had finished using their device the decrease in peak DF was no longer statistically significant, for either device (p = 0.058). By contrast, van der Linden et al. (47) found equal, but insignificant, improvement in all measures.
With regards to secondary measures, the lower extremity (LE) Fugl-Meyer test was a BFS measurement reported by 2 trials (17, 42). There were differences in their findings, with Kluding et al. (17) reporting improvement in both groups that, despite only the AFO group showing within-group statistically significant improvement (p < 0.05), was statistically comparable (p = 0.178). Sheffler et al. (42) found an equal between-group lack of improvement (p = 0.321) (Table IV).
Across other measures used by single trials there was a mixture of therapeutic effects results reported across and/or within trials (Table IV).
This review shows, for the first time, that AFOs produce an equally positive therapeutic effect on walking speed to that of FES. These improvements are observed for stroke alone and are seen after 4–6 weeks of use. These findings are based on meta-analysis of RCT-level evidence (33) and those RCTs were deemed to be of moderate (or less) risk of bias (33), meaning that there can be confidence in these findings. Equality of therapeutic effect on walking speed has not been demonstrated previously, as the focus of previous reviews (16, 32, 45, 50) and primary studies (51, 52) has been on the therapeutic effects of FES alone. What the RCT evidence does not answer is whether this improvement translates into activity within the person’s own environment.
It is essential to gain a better understanding of whether therapeutic effects on walking speed translate into activity in a home setting, and the mechanisms by which therapeutic effects are achieved, in order to better inform clinical guidelines about which device to use for which patients. However, the included trials do not provide the measures needed to identify the mechanisms by which the devices achieve speed increases (question 2). Narratively, there is a suggestion that FES, but not AFOs, lead to improvement in voluntary muscle activity (29), although both produce equal effects on kinematic gait pattern (42, 47).
One possible explanation is that remedying foot drop using either device allows increased time spent walking, thereby facilitating task-specific repetitive practice; which is widely accepted as leading to therapeutic improvement (21). However, from the activity monitoring results of the included RCTs it is unclear whether this occurs (17, 43), with non-RCT studies also finding variable results (53–55).
An alternative explanation for equivalent effects on walking speed may lie in how the increased walking speed is achieved; i.e. via restoration of motor function or compensation (56). True motor recovery is defined as the reversal of an impairment such that it results in the restitution of the functions governed by it (20). Compensation is a restoration of function achieved through adaptation or substitution of remaining motor elements (20). Being able to distinguish between recovery and compensation facilitates clinical decision-making and potentially increases intervention efficiency (21). Crucially, recognizing the distinction relies on an understanding of the mechanisms-of-effects.
The mechanisms-of-effects ascribed to FES are based on the fact that it is seen as an active orthosis, whereby volitional muscle activity is combined with lower motor neurone stimulation. This leads to a number of possible neuromuscular plastic mechanisms, including: repeated muscle contractions leading to increased oxidative capacity; increased number of micro-capillaries and change in fibre type at a muscular level; convergence of orthodromic/antidromic impulses at the anterior horn leading to strengthening of synapses at a spinal level, as well as cortical changes (23–25). Structural cortical changes result from increased cortical excitability (26) are thought to strengthen the residual descending connections from motor-related areas of the cortex (24). In the case of therapeutic effects this culminates in increased volitional muscle activity of the weak dorsiflexors/evertors of the ankle, which is thought to positively influence other biomechanical features and therefore the restitution of associated functions.
In contrast, FES literature has asserted that AFOs, as passive devices, mask the abnormal muscle activation associated with foot drop impairment and so, whilst range of movement is maintained, neuromuscular plasticity mechanisms result in a loss of volitional activity in those muscle groups over time (17, 29). This would mean that, in the absence of the AFO, other muscle groups will have to compensate for this deficit.
In order to provide evidence for the hypothesis of differential changes in volitional muscle activation between FES and AFOs, both EMG and kinematic data of walking are needed. Only 1 trial included in this review provided EMG outcome measures (29), finding that FES use was associated with an increase in voluntary RMSmax for TA and GS, whereas AFO use was not. Similarly, with FES use voluntary activation of TA during swing was maintained relative to baseline, whereas following a period of AFO use TA activation declined during swing. This suggests that the ability to voluntarily activate TA and GS muscles may be maintained, or even improved by a period of FES use compared with AFO. Previous non-RCT studies and systematic reviews support this suggestion, as they have shown increased TA muscle activity, force and size with FES use (57–60) with the opposite occurring in AFO (4, 28, 30, 31). Further trials examining EMG following FES and AFO use are therefore needed if this potential mechanism-of-effect is to be more fully understood.
Despite the potential for differing effects on volitional muscle activity, the RCT-evidence suggests that both devices have equal therapeutic effects on kinematic measures (43, 47); whether the effects are positive, negligible or negative is unclear. Non-RCT studies examining gait kinematics are limited with regards to FES (39, 61) and AFO (62). Further kinematic comparative study is therefore required to identify whether improvement is compensatory or restorative and to correlate EMG data with functionally meaningful improvements.
These trials should consider how they both measure and define therapeutic effects. For example, in the included trials (17, 43) it was unclear whether activity (number of steps) was measured during walking while wearing the device, during walking when the device was not being worn, or a combination of both. Furthermore, the current definition of improvement in measured walking behaviours without the device being worn following a period of use (13) may not be clinically relevant.
In all the reviewed RCTs participants used the devices for a period of time, with measurement occurring immediately at the end of that period; with or without interim data collection points. This aligns with the definition of therapeutic effects and is consistent with its interpretation by non-RCT studies (63). However, these effects are clinically relevant only if the motor recovery effect is sustained for a meaningful period of time for the individual. The intervention period for the participants within Sheffler et al.’s trial was 12 weeks, at which point they measured walking behaviours. In contrast to the other included trials, they also invited participants to additional data collection sessions 12 and 24 weeks after they had finished using the devices (42). They found that the lack of effect on most measures reported after the intervention period was, unsurprisingly, sustained at these time-points. However, the equal decrease in peak DF during swing was sustained 12 weeks post-use, but not 24 weeks post-use. Justification of data collection time-points that align with an understanding of the mechanisms-of-effect and their clinical relevance are therefore needed. Only then will the time course of effects and the sustained therapeutic effects of the devices on measures, including kinematics, be understood.
This review adhered to the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) criteria (64, 65) and guidance from the Cochrane Collaboration (33). This, coupled with the specific questions and inclusion of RCTs only (66), enhances its validity.
Our findings can only feasibly be generalized to a non-progressive CNS population, as data comes only from participants with stroke and CP. Further investigation into progressive CNS disorders is necessary, as the potential for therapeutic improvement has been shown to be limited with such conditions (54). Given that most individuals with CNS disorders will be on medication (e.g. anti-spasticity medication (67)), which could confound results, future trials should also consider how to control and report this variable.
Possible variability in the device design could limit the viability of the comparisons made by the primary trials and, by extension, this review. Lack of description of key aspects of either device means that the impact of pooling data from different FES set-up parameters and AFO mechanical properties cannot be explored (11, 25). However, given that both types of device were prescribed by qualified professionals, combining data from different trials reflects clinical practice and arguably improves the clinical validity of the findings.
The risk of selection bias in the included trials was the greatest threat to the internal validity of our findings. This could mean that the estimates of effect are exaggerated (68, 69) but the inclusion of a sensitivity analysis excluding trials with high selection bias (12, 29) as a result of un-randomized sequence generation suggests there was no impact. Care should be taken to avoid this risk in future RCTs. There were a number of areas deemed to be unclear areas of risk across and within the RCTs; detailed reporting might have avoided this. Overall however, the RCTs were of at only moderate (or less) risk of bias, providing confidence in our findings.
Two trials could not be included in the meta-analysis because data was reported in such a way as to not allow analysis for the purpose of obtaining therapeutic effects. One of these trials would have provided additional participants’ data for only 6 FES and 3 AFO, and so the effects are probably negligible (48). The absence of the full data-set from the 6- and 12-week data collection points from the other trial (17), n = 198, meant that no sub-group analysis of walking speed could be performed at the 12–13-week point. It may also have impacted the 4–6-week analysis, meaning that this aspect of therapeutic effects comparison (question 1ii) could not be explored. Future RCTs should report the raw results for all planned primary and secondary end-points and separate data relating to different effects (70).
This meta-analysis shows, for the first time, that FES and AFO are statistically proven to have the same therapeutic effect on walking speed in CNS foot drop. This effect has also specifically been shown to occur for foot drop caused by stroke and is observed after 4–6 weeks’ use. Nevertheless, whether this increase in walking speed translates into increased activity in the person’s own environment, and how this improvement is achieved, remain unclear. Future research should therefore focus on the measures suggested in this review in order to address this gap in the evidence base and, with regards activity monitoring, address when the measures are captured. In addition to measurement, future trials must also report specific device details, capture sustained therapeutic effects and should involve a variety of CNS diagnoses with justified primary and secondary end-points. Only then can clinical decision-making be significantly advanced and supported by a robust evidence base.
We would like to thank the corresponding authors from Kottink et al. (Anke Kottink), Kluding et al. (Keith McBride) and van der Linden et al. (Mariette van der Linden) for generously providing their unpublished results.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize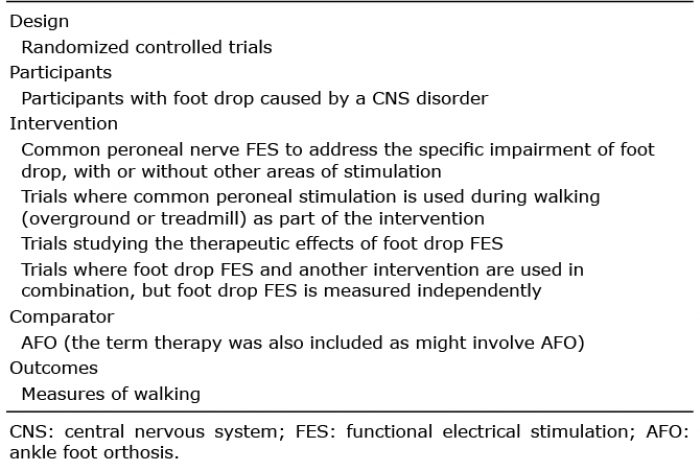 Click to show fullsize
Click to show fullsize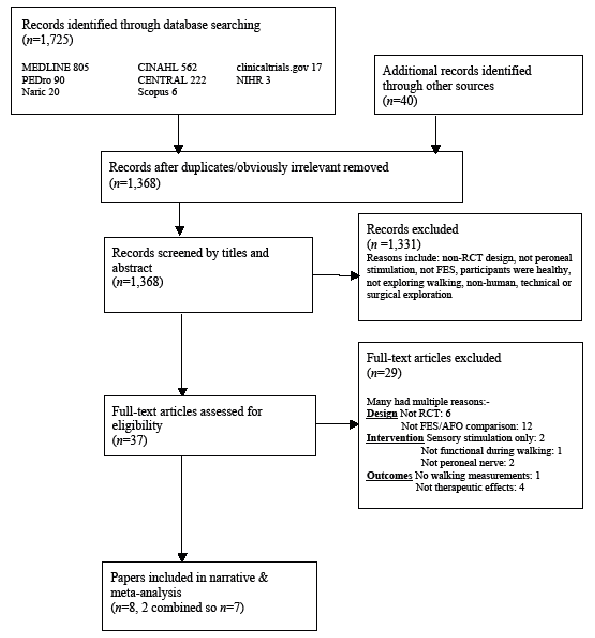 Click to show fullsize
Click to show fullsize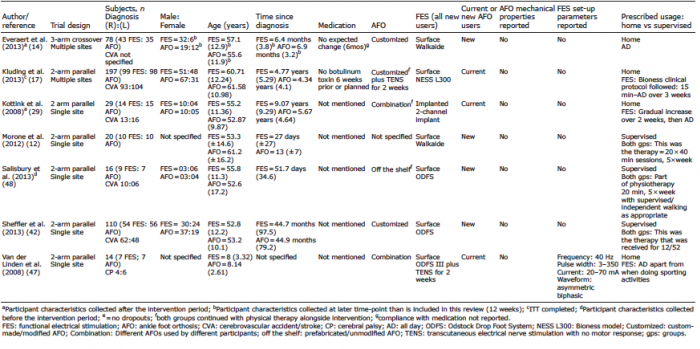 Click to show fullsize
Click to show fullsize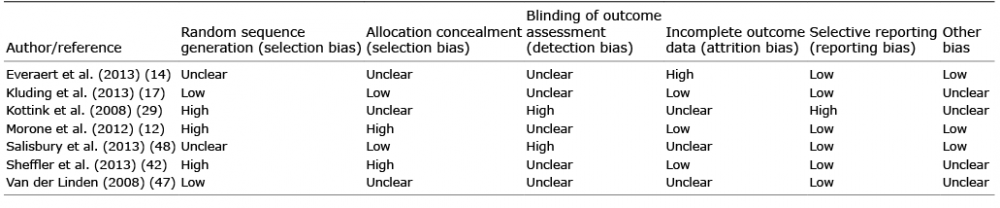 Click to show fullsize
Click to show fullsize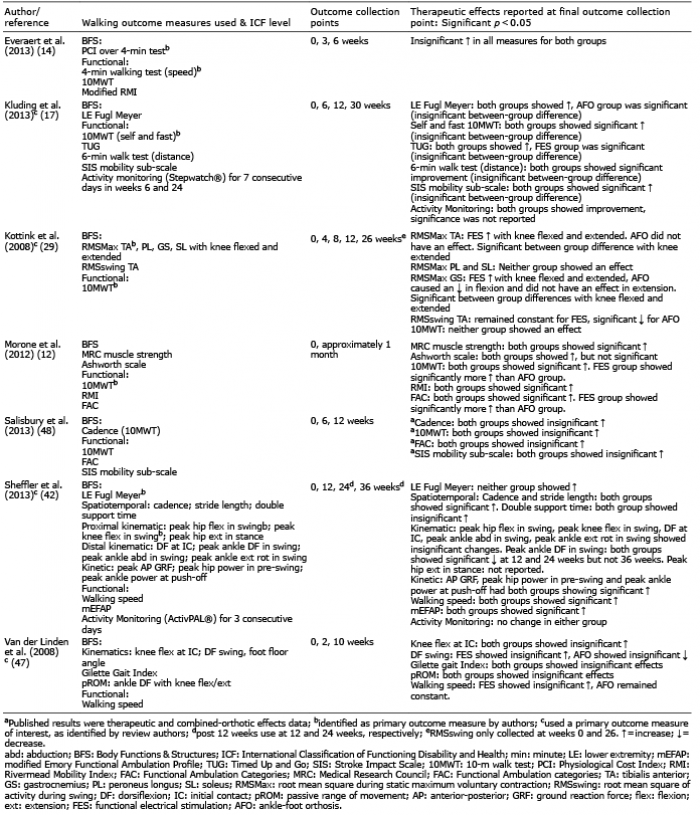 Click to show fullsize
Click to show fullsize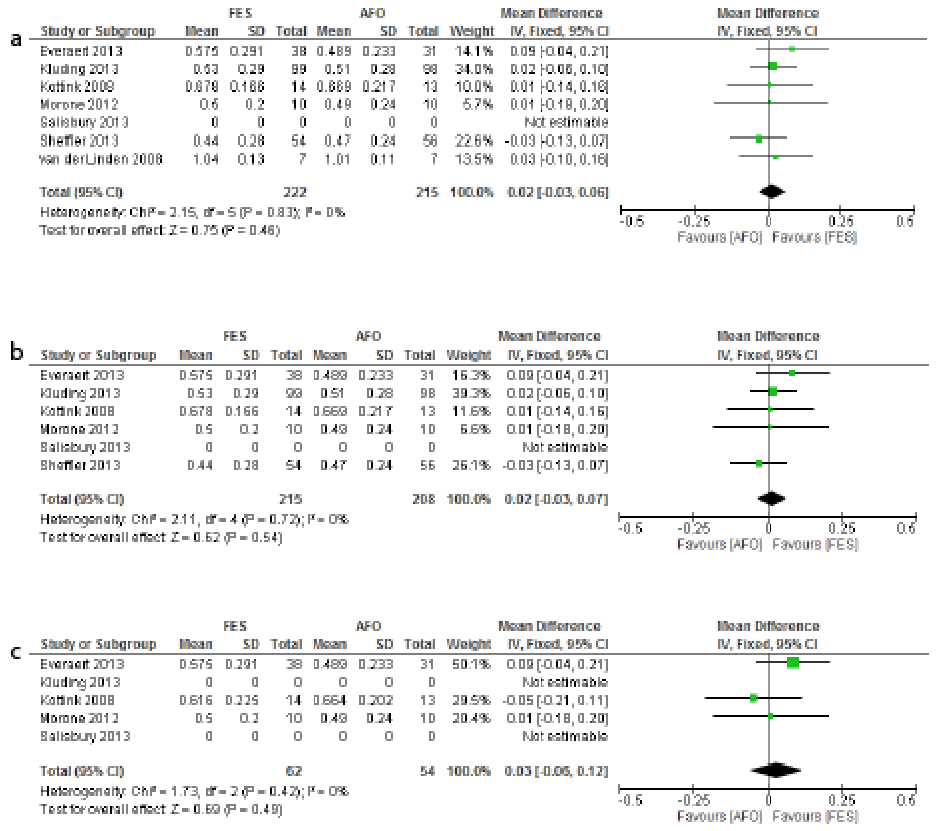 Click to show fullsize
Click to show fullsize