
From the 1Institute of Health and Society, CHARM Research Centre for Habilitation and Rehabilitation Models & Services, 2Institute of Clinical Medicine, Faculty of Medicine, University of Oslo, Oslo, Norway, 3Department of Physical and Rehabilitation Medicine, Hannover Medical School, Hannover, Germany, 4Department of Physical Medicine and Rehabilitation, 5Department of Clinical Neuroscience in Children, Oslo University Hospital, Oslo, Norway, 6Norwegian Association for Persons with Injuries, LTN, 7Norwegian Federation of Organizations of Disabled People, 8Norwegian League against Rheumatism, 9The Norwegian Cerebral Palsy Association, 10Department of Neurohabilitation, Oslo University Hospital, Oslo, Norway and 11Department of Rehabilitation Medicine, Coordination Centre for Rehabilitation Research, Hannover Medical School, Hannover, Germany
Objectives: To apply the Classification of Service Organization in Rehabilitation (ICSO-R) classification of services to different target groups, include the user perspective, identify missing categories, and propose standardized descriptors for the categories from a Norwegian perspective.
Design: Expert-based consensus conferences with user involvement.
Subjects: Health professionals, stakeholders and users.
Methods: Participants were divided into 5 panels, which applied the ICSO-R to describe the habilitation and rehabilitation services provided to children with cerebral palsy and people with Huntington’s disease, acquired brain injuries (traumatic brain injuries and stroke) and painful musculoskeletal conditions. Based on the Problem/Population, Intervention, Comparison, Outcome (PICO) framework, the services were described according to the ICSO-R. Missing categories were identified.
Results: The ICSO-R was found to be feasible and applicable for describing a variety of services provided to different target groups in Norway, but the user perspective was lacking, categories were missing, and a need for standardized description of the categories was identified.
Conclusion: The present work supports the need to produce an updated version of the ICSO-R and to encourage national and international discussion of the framework. The ICSO-R has the potential to become a tool for the standardized assessment of rehabilitation services. For such purposes, more standardized descriptions of subcategories are necessary.
Key words: habilitation; rehabilitation; health services; classification.
Accepted Oct 30, 2017; Epub ahead of print Dec 20, 2017
J Rehabil Med 2018; 50: 00–00
Correspondence address: Cecilie Røe, Department of Physical Medicine and Rehabilitation, Oslo University Hospital, Kirkevn 166, 0407 Oslo, Norway. E-mail: eller@medisin.uio.no
The World Report on Disability (1) identifies major deficits in rehabilitation care for people with disabilities as an important barrier to achieving optimal functioning and participation in society. To develop the capacity and quality of rehabilitation services, we need a uniform language to describe and classify existing rehabilitation services. Recently, a draft for an International Classification of Service Organization in Rehabilitation (ICSO-R) was proposed by Gutenbrunner et al. (2). The proposal is based on the conceptual model of rehabilitation services developed by Meyer et al. (3) and the categories expanded on a series of international frameworks regarding health service delivery, health professional classification and classification of diseases and functioning (4–7). A 3-level classification targeting the meso level of service provision was originally intended. Here, “meso level” refers to services that target patient or user groups and offer intangible products within an organizational setting (3). However, a 2-level classification using dimensions (level 1) and categories (level 2) was launched, urging the rehabilitation community to discuss and test the classification as a basis for developing a third level and definitions of value sets or standardized descriptors for the levels (2).
To improve the description and evaluation of rehabilitation services, classifications should comprise well-defined, mutually exclusive categories (8). Furthermore, rehabilitation includes a broad spectrum of services that varies across countries and user groups and should be covered by a classification. The European Union of Medical Specialists, Physical and Rehabilitation Medicine section (UEMS PRM) conducted a workshop focusing on the feasibility and applicability of the ICSO-R (9). However, the narrative description of services within each category varied, and there were overlapping descriptions for the categories (9). Similar to the development of the International Classification of Functioning, Disability and Health (ICF) classification (5, 10), the ICSO-R will require the development of more specific definitions for the categories. This approach will facilitate the use of the classification system as an indicator of quality and service outcomes (11).
Norway is a welfare state, and its habilitation and rehabilitation health services are public (12). Nevertheless, in the Norwegian welfare system, the content and organization of services differ across age groups and according to the nature of the disability and the underlying disease (www.fhi.no). The delivery of habilitation and rehabilitation is provided by the Ministry of Health through 4 health regions (North, Middle, West and South-East) and 428 municipalities, termed specialized and community-based health services, respectively (13, 14). The services may be institution-based or outpatient-based in both the specialized and community-based settings and vary across regions (15, 16). Due to the lack of a common framework for assessment and classification, knowledge about the optimal organization of rehabilitation services in terms of access, disease phases and target groups is generally lacking (17).
The aim of the present paper was to describe the rehabilitation services provided to different target groups in Norway according to the ICSO-R classification, to identify challenges in the classification, and to include the user perspective. We also aimed to identify missing categories and propose standardized descriptors for the categories from a Norwegian perspective.
Persons involved in national multicentre studies or registers with experience in a variety of habilitation and rehabilitation services were invited to participate. Their experience included services for children with cerebral palsy and people with Huntington’s disease, acquired brain injuries (traumatic brain injuries and stroke) and painful musculoskeletal conditions; and users (people with medical conditions). The health professionals comprised physicians (n = 5) (3 physiatrists 1 neurologist, 1 paediatrician, nurses (n = 2), neuropsychologists (n = 1), occupational therapists (n = 3), physiotherapists (n = 5) and a social worker (n = 1). The stakeholders (n = 4) represented university community, heads of clinical departments or research departments and persons involved in national studies or registers. The users, defined as people with medical conditions and/or their relatives and/or their user organizations, (n = 4) were invited to participate. The users included a person with rheumatism, a relative of a person with cerebral palsy, a person from the user organization for persons with severe injuries including traumatic brain injuries, and a person from the Norwegian Federation of Organizations of Disabled People (which represents 82 specific user organizations). The conditions, which comprise both trauma- and disease-related disabilities, were chosen to include a wide range of habilitation and rehabilitation services, age groups, and rehabilitation institutions to test the comprehensiveness and applicability of the ICSO-R classification.
In the first workshops, the health professionals, stakeholders and users were familiarized with the concept of the ICSO-R framework (2) and the results from the UEMs workshop (9). Subsequently, they were divided into panels according to their respective expertise. Based on a Problem/Population, Intervention, Comparison, and Outcome (PICO) framework (18), each panel was instructed to provide a narrative description of the services provided (P) according to the ICSO-R (I). The panels were also asked to discuss the description with a larger group of experienced clinicians, to report the challenges involved in this task (C), and to identify missing categories and suggest descriptors for the categories (O).
Subsequently, 2 new workshops were undertaken that pertained to children with cerebral palsy, Huntington’s disease, acquired brain injuries and painful musculoskeletal conditions. The challenges of applying the ICSO-R, the narrative descriptions and the suggested missing categories and proposed descriptors for the categories from each target group were shared with all panels and discussed. Similarities and disparities across the groups were discussed and tested on the other target groups. Finally, a consensus-based proposal for additional categories and value sets was elaborated, with the aim of retaining the greatest possible diversity of categories and descriptor groups while standardizing their wording as much as possible.
The main challenge for the panels throughout the process was shifting from the micro to meso level of healthcare (from the patient to the service level) and from describing individual rehabilitation programmes instead of services to groups. Secondly, the wordings of the dimensions and categories were unfamiliar, and the guidance from the ISPRM discussion paper needed to be thoroughly emphasized to provide a meaningful common platform for describing the different services.
In general, the dimensions of the ICSO-R were found to be mutually exclusive, although one of the panels noted some ambiguity regarding the difference between the provider and delivery dimensions. This is illustrated by the fact that several of the panels used “multidisciplinary team” as a descriptor in both the Provider (in the category of Human Resources) and Delivery dimensions (under Team Structure). Furthermore, the Mode of Production category was also discussed, as “inpatient” and “outpatient” may also characterize the provision of services.
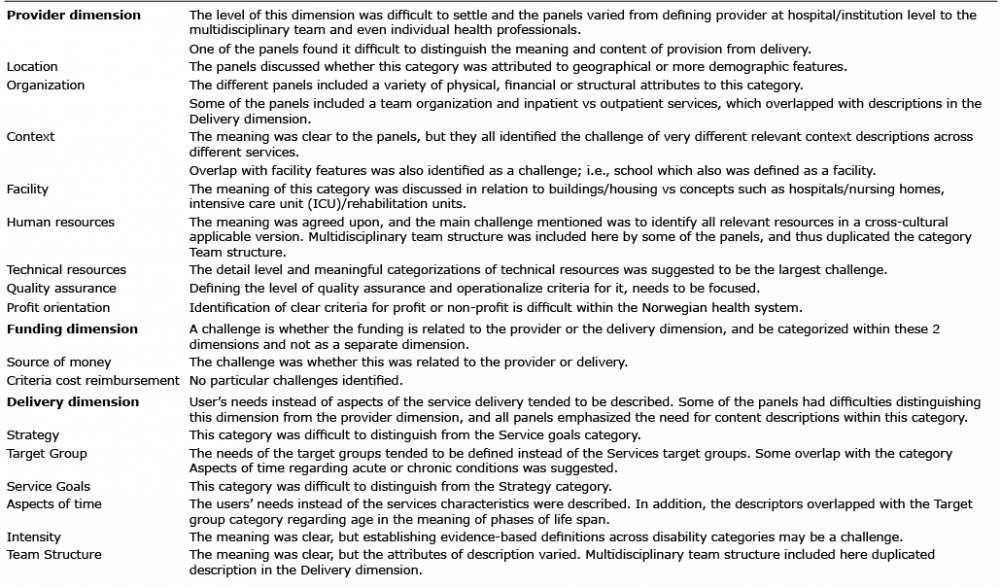
However, the main discussions were related to the levels and sizes of services to which the ICSO-R could and should be applied. For example, the panels discussed whether it would be meaningful to describe the national rehabilitation services within the framework of the ICSO-R or whether an additional framework for the health services sector at the macro level should be applied. At the least, the meaningful descriptors will vary considerably compared with the description of services within a single unit; for example, a rehabilitation unit at a local hospital or within a nursing home. The main challenges identified by the panels in the dimensions and their categories are summarized in Table I.
Table I. Key challenges in defining the content of the dimensions and categories, as evaluated by the panels
All the panels used a wide variety of narratives to describe the categories. To some extent, the meanings could be interpreted as identical or overlapping, but the content of the descriptions also varied. A keyword-based synthesis of the narratives used by the groups is provided in Table II. As presented, the descriptors of the different categories in this dimension are not mutually exclusive. Furthermore, the groups reported problems capturing the meaning of the Context category in relation to the services, as well as difficulty distinguishing the descriptions in that category from those in the Facility category and, to some extent, from the Organization category. Important features of the services provided to the present target groups that the panels found difficult to categorize were rehabilitation provided within the educational and health system, whether institutions were solitary or part of enterprises, and whether the services were delivered by rehabilitation departments or units or integrated into other services. The panels also found it difficult to describe buildings in terms of the Facility category in relation to the services provided in Norway. It was also suggested that the building aspect was more related to the delivery dimension than to the provider dimension. All the panels interpreted the meanings of human resources and technical resources similarly, although they found it difficult to describe these resources in a uniform way. Furthermore, the panels generally agreed on the meaning of quality assurance and profit orientation, although they outlined different attributes for these categories (Table II).
Table II. Summary of the key elements of the narrative descriptions provided by the 5 panels based on service provision to people with traumatic brain injuries, elderly people with stroke, children with cerebral palsy, and people with Huntington’s disease and painful musculoskeletal conditions, and the suggested standardized descriptors for the categories
The panels noted that research and education are important parts of service provision. They suggested defining these aspects as additional categories. The strong position of users (people living with diseases and disabilities and their relatives) and their organizations in rehabilitation may also justify making this a separate category within the Service delivery dimension. For example, user panels or councils are statutory for medical and rehabilitation institutions in Norway. The alternative would be to include user involvement as part of the descriptors for all categories.
Even in a rather uniform and publicly oriented system such as Norway’s, there may be separate financial bases for the provider and the actual service delivery. Hence, the use of the public budget mixed with public or private cost reimbursement and personal deductible charges is common. There is debate as to whether funding is a separate dimension or should be included as categories within the provider and delivery dimensions.
Switching from the users to the services as the object of description was particularly challenging in this dimension. Furthermore, a main challenge was to distinguish the Strategy and Goal categories, as exemplified by overlapping narrative descriptions in these 2 categories (Table II). Aspects of time were attributed to the lifespan perspective, with different service delivery needs for people in different age groups (e.g. preschool or school age, teenage, young adults, adults, older adults), the acute vs chronic phase of the disability, as well as to the time aspects of service provision (Tables I and II). The panels also commented on difficulties with defining the intensity category, although all panels had described it according to high, intermediate and low attributes. The lack of a category for the content of the services, as well as information about family and user involvement was noted.
The variety of attributes presented in the different narrative descriptions of categories represents a challenge for producing more standardized descriptions. Hence, the panels suggested grouping the descriptors into subcategories or a third level (Table II). Ideally, descriptors from all subcategories should be applied when characterizing service systems and the descriptors of the different subcategories should not overlap. The panels also emphasized that more detailed descriptions should be developed within a digit or tree of subcategories (as in the ICF).
For the category Location, all panels suggested that country was important and should be specified. This will allow aggregation by continent, industrialized countries, etc., according to the purposes of an investigation. Furthermore, elements related to population density and infrastructure were considered relevant. As the definitions of city, village and countryside may vary, the panels suggested using the terms urban, rural and intermediate according to the European Commission definition (Statistics in Focus 16/2013; Author: Regional statistics team. ISSN:2314-9647, Catalogue number: KS-SF-13-016-EN-N),
The category Organization was rather more challenging given the variety of narratives applied and the overlap with Context and Facility. After considerable discussion, 5 subcategories with sets of standardized descriptors were agreed upon (Table I), including the description of whether rehabilitation services delivery is isolated or integrated with other medical services. The public and private subcategories were defined according to whether services are organized for governmental or non-governmental purposes (19). Service provision in Norway is divided between the community level and the regional health enterprises, and this categorization is important.
The Context category was also challenging to subcategorize and specify, but the panels suggested 3 subcategories and a fourth category describing the catchment population (in number). Furthermore, within this category, further subdivision is clearly needed and would be meaningful. For example, “community” should be specified according to whether the context is a nursing home or the patient’s home.
The panels expressed even greater challenges in defining meaningful standardized subcategories and descriptors for Facility, given the understanding of facility as buildings. Overlap with the Context category was evident in the narrative descriptions. The panels suggested some important aspects of service provision, such as the type of unit for delivery, presenting an open question regarding redefinition in this category.
The category Human resources should be specified with the main relevant rehabilitation professions and checked according to its presence/involvement in particular services according to the International Standard Classification of Occupations (ICSO-08) (http://www.ilo.org/public/english/bureau/stat/isco/isco08/). Informal care may be added as a subcategory.
Panel members suggested dividing the Technical resources category into diagnostic and rehabilitation resources. Further subdivision into laboratory and radiological resources and rehabilitation resources into individualized adaptive equipment, training equipment (including assistive devices), cognitive technology and environmental resources (lift, ramp, door opener, car, etc.) will be needed.
The panels agreed that it is important to redefine the Quality assurance category into official quality systems that may be specified at the hospital and department level.
The categories within the Funding dimension were similarly specified by all the panels, and few choices of descriptors were found necessary (Table I). It is worth noting that, for the Norwegian context, individuals generally pay a deductible charge for both private and publicly funded services. It is also worth emphasizing that government reimbursement is based on diagnosis-related groups.
The panels generally agreed on subcategories and standardized descriptors for the categories within the delivery dimension despite some challenges with overlap between the Strategy and Goal categories, which are closely related (20). However, the panels also emphasized the huge problems of attaching clear definitions to the descriptors, for example, within the Intensity category.
Regarding the Strategy category, multiple narrative descriptions were suggested. Several subcategory sets were discussed. One solution was to build on the terminology applied in the Action axis of the International Classification of Health Interventions (ICHI) (http://www.who.int/classifications/ichi/en/).
There are several important aspects of the Target group, and 5 subcategories were suggested. For the severity category, the panels emphasized that descriptors of severity must be closely related to the relevant diagnostic group. For example, mild, moderate and severe descriptors based on the Glasgow Coma Scale score may be applied to the traumatic brain injury group (21), whereas for stroke and other diagnostic groups, severity should be defined using disease-specific criteria (22, 23).
For the Service goals category, the panels agreed that prevention, maintenance and improvement are relevant descriptors. To avoid overlap with the strategy, the panels suggested focusing on the ICF-related descriptors. The group discussed independence and health-related quality of life, but agreed that these goals are more individual than service related.
The individual panels had very similar suggestions for descriptors for Aspects of time and Intensity, but emphasized the need to define the values related to these descriptors. For example, it is necessary to determine how many hours a day defines the service delivery as high intensity.
Agreement was also easily reached regarding the descriptors of Team structure, although other aspects, such as a well-coordinated team and a flat vs hierarchical team structure may be relevant. The panels also consented regarding reserving the home, school and work descriptors for service provision and describing 24-h, day-based or polyclinic services here. The term “patient” may be misleading in several contexts, but the panels did not find a more appropriate term to use at present. Family-, user- and peer-based involvement in service delivery were suggested as additional descriptors within the “other” category.
The present approach builds on narrative descriptions of services within the ICSO-R framework. In contrast to Kiekens et al. (9), we defined the target groups and included all phases and types of services. Based on the differences and similarities between the different target groups, we identified possible common descriptors and subgroups for them.
In accordance with the experiences of the UEMS workshop (9), a wide variety of narrative descriptions were applied. The variations were, to some extent, related to the lack of criteria for the content of the categories, and the panels provided the same information, but related it to different categories. Secondly, similar content, but different wording, was applied. Finally, real differences in the service provision to the different target groups were reflected in the descriptions. The ICSO-R is based on the conceptual definition of rehabilitation services proposed by Meyer et al. (3) and intends to meet the needs for standardized description and classification at the meso level. It is clearly a challenge to apply the ICSO-R to very different services to define categories within the dimensions in a meaningful and comparable way; the 1-level dimensions were easier to apply. Ideally, clear definitions and inclusion and exclusion criteria for the categories within a 2-level structure would be preferable. Several different attributes that are important for the services were described within each category, supporting the need for a 3-level classification system, as was originally intended.
However, the present work also revealed the challenges of a universal conceptual basis for the third level and, to some extent, the second level. For example, specialized vs community-based service provision is a very important aspect of rehabilitation in Norway. The cooperation reform (White Paper 47, 2008–2009) and currently, the planned reform (White Paper 14, 2014–2015), which intend to allocate the delivery of rehabilitation services to larger municipalities, are heavily discussed in Norway. It is feared that moving rehabilitation from the specialized level to the community level could compromise the quality of service, based on the assumption that less knowledge and fewer resources are available at the community level. From an assessment perspective, it is a problem that the Norwegian system does not fit into “The World Health Report 2000’s” definition of specialized care (http://www.who.int/whr/2000/en/), which suggests that these terms are subject to country and cultural differences. Hence, we suggest omitting this term from the classification. The health, education and social sectors may be relatively universal entities, but an international discussion of, and consensus for, terms and definitions is clearly needed.
We emphasize the potential importance of whether rehabilitation is integrated into other medical services. This factor may be important for the quality of services, as documented within stroke and traumatic brain injury care (24, 25). Integration into larger enterprises may also influence quality systems and eventually outcomes at the patient level (26). However, the criteria for these factors need to be elaborated.
The panels found the Context category challenging. In the ICF, context is related to the entire background of a person’s life and comprises both personal and environmental factors; however, only the latter are classified (5). Translated into the ICSO-R, the context would comprise the complete financial, organizational and facility and resource background for these services. Although the panels suggested a series of important elements for this category, we suggest that this category should be redefined. The panels also found the Facility category difficult to describe in a meaningful way in terms of service provision to the chosen target groups in Norway. The panels emphasized the importance of describing hospital, department and unit level of service delivery; it is possible that these features could be pinpointed as a fourth level below the hospital in organization, and that the Facility description could be more closely related to the building elements. Health professions constitute the major source of human resources and could be classified according to the ICSO-08 (http://www.ilo.org/public/english/bureau/stat/isco/isco08/); however, family, friends and volunteers may also contribute to the quality of the services (27). There were general agreements among the present panels regarding the subdivision of technical resources, quality assurance and profit orientation. However, the panels emphasized the need for quality assurance in reference to official systems in accordance with the comments by Van de Velde et al. (28). The integration of education and research into service delivery was identified as a missing category, as also indicated by Kiekens (9). Rehabilitation is publicly funded in Norway, thus there was no disagreement in the reporting of categories in this dimension. However, the categories in this dimension need to be tested in more diverse financial settings.
The diversity of service delivery across habilitation and rehabilitation services and across children, adults and the elderly in Norway became evident when the panels were asked to describe the services and propose descriptors or value sets for the categories in the service delivery dimension. Choices and compromises need to be made to achieve a universal classification. The present panels agreed that the categories and third-level subcategories should refer to the established classifications when possible, as proposed for the strategy, target groups and goals. We were less certain about the use of reference documents for the intensity and time categories. Team structure could refer to the interdisciplinary and multidisciplinary aspects that are of major importance in rehabilitation (29). Finally, user involvement should be included and defined in service delivery (30).
The capacity and performance concept has not been emphasized in relation to the ICF, but may be of importance regarding service delivery (31). A uniform description of the existing services, along with documentation of the users’ needs, may also provide a platform for negotiation with stakeholders regarding necessary scale-up of rehabilitation services (32). The users involved in the present project emphasized that access to, and the content of, the services may be more important than several of the categories described in the ICSO-R; hence, combining the ICSO-R with measurements of these features may be needed to develop better quality indicators. Finally, the panels also suggested that the revised version of the ICSO-R classification could be used in a normative way in describing the necessary levels of service provision and delivery.
The ICSO-R was found to be feasible and applicable for describing a variety of services provided to different target groups in Norway. The present work supports the need to discuss the proposal nationally and internationally and to launch an updated version. The framework also has the potential for classification and analytic approaches that aim to identify quality indicators for rehabilitation services. For such purposes, more standardized descriptions of subcategories are necessary. We also recommend the combined use of the ICSO-R with other frameworks to capture a broader spectrum of quality indicators that are important to users.
The present project was conducted by CHARM Research Centre for Habilitation and Rehabilitation Models & Services, which is financed by the Norwegian Research Council.
The authors have no conflicts of interest to declare


 Click to show fullsize
Click to show fullsize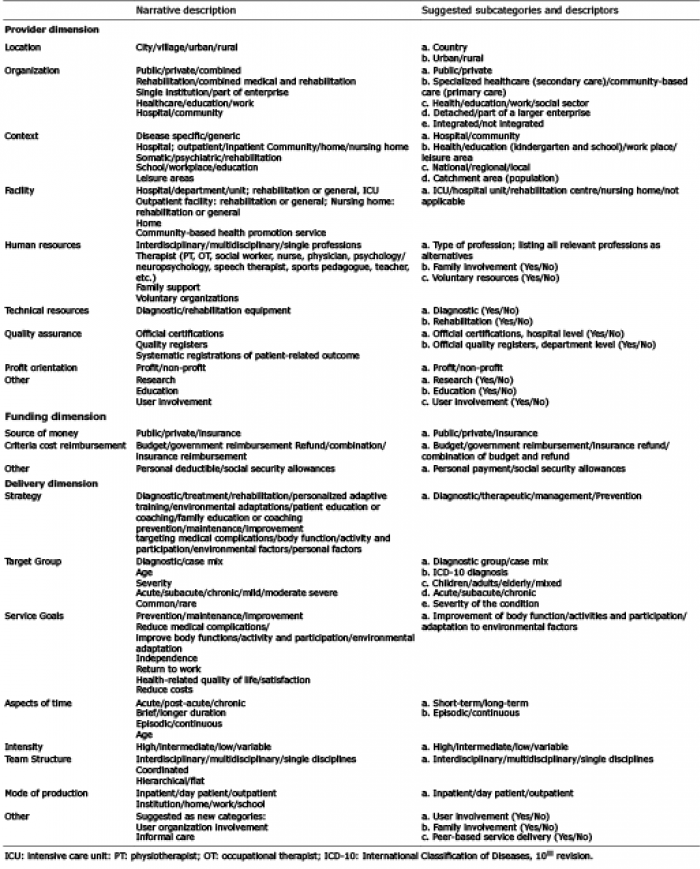 Click to show fullsize
Click to show fullsize