
From the 1Department of Physical Medicine and Rehabilitation, Ankara University Faculty of Medicine, 2Vocational School of Haymana, Physiotherapy Programme, 3Department of Biostatistics, Faculty of Medicine, Ankara University, Ankara, Turkey
Objective: To investigate the effects of kinaesthetic ability training with the Kinesthetic Ability Trainer (KAT) on unilateral neglect and functional outcomes in stroke patients.
Study design: An assessor-blinded, randomized controlled, clinical trial.
Methods: A total of 64 stroke patients with unilateral neglect (mean age 61 (standard deviation (SD) 12) years, 60.4% male, mean time since stroke 6.4 (SD 10.4) months, left hemiplegia 92.5%) were randomly assigned to a conventional rehabilitation programme (control group, n = 32) or KAT plus a conventional rehabilitation programme (KAT group, n = 32) for 4 weeks. Patients were assessed with the Behavioral Inattention Test (BIT) and Functional Independence Measure (FIM) before and after therapy.
Results: Both groups showed significant improvements in all subscales of the BIT (conventional and behavioural) (p < 0.001) and the FIM motor scale (p < 0.001) after therapy. Recovery from neglect was assessed, based on the BIT cut-off scores. The recovery rate for behavioural BIT was 40% in the KAT group and 17.9% in the control group (p = 0.07), whereas recovery rates according to the conventional BIT were 16% and 10.7% in the KAT and control groups, respectively.
Conclusion: Kinaesthetic ability training provides clinically meaningful improvement in stroke patients with unilateral neglect. It may be useful as an adjunctive therapy for rehabilitation in these patients.
Key words: stroke; neglect; rehabilitation; kinesthesia.
Accepted Nov 7, 2017; Epub ahead of print Dec 5, 2017
J Rehabil Med 2018; 50: 00–00
Correspondence address: Sehim Kutlay, Department of Physical Medicine and Rehabilitation, Ankara University Faculty of Medicine, İbni Sina Hastanesi, FTR AD, Kat 4, Sıhhiye, TR-06100 Ankara, Turkey. E-mail: skutlay@medicine.ankara.edu.tr
Stroke is a major cause of long-term disability, with implications for health status and clinical outcomes, including mortality, morbidity, and cost to the health services (1). Rehabilitation is a long and demanding process, both for patients and for rehabilitation teams. Clinical conditions, such as unilateral neglect (UN), are challenging for patients undergoing rehabilitation and can frequently hamper rehabilitative efforts (2).
While UN can occur in patients with right- or left-sided lesions of the brain, it is more common among those with right hemisphere stroke (3). The frequency of UN was reported to be 48% in a rehabilitation setting (4). Its most typical feature is failure to respond to stimuli from the contralateral space, including visual, somatosensory, auditory, and kinaesthetic sources. UN has negative impact on sensorimotor performance, which impedes mobility activities including gait and balance (5). Balance is a prerequisite for all functional activities and an essential part of sitting, sit-to-stand and walking activities. Patients with UN usually have decreased awareness of the deficit, which frequently limits activities of daily living (ADL). This also increases the complexity of the rehabilitation period, hospital stays, and risk of accidents (6–8). Some authors suggest a possible interaction between the damage to the special attentional system and a co-occurring deficit of the sustained attention system in patients with UN (9, 10). It is known that additional visual information can help these patients to become more aware of their body displacements and orientation in space (11).
While some obvious signs of UN spontaneously improved within a few weeks following diagnosis of stroke, most patients with UN need various treatment modalities, including visual scanning training, prism adaptation, neck-muscle vibration, optokinetic stimulation, vestibular stimulation, trunk rotation, etc., during rehabilitation (12, 13). Toglia & Cermak (14). used an interactive intervention method called “dynamic assessment” in patients with unilateral neglect. This interactive procedure measures the change that occurs in response to cues, strategies, feedback, or task-specific conditions that are applied during the therapy. The Kinesthetic Ability Trainer (KAT; LLC, Vista, CA, USA) is a balance and training system that provides visual feedback to control body posture on a movable platform. The KAT system works by altering the stability of a movable platform, on which an individual stands, and/or by varying the degree to which they alter their base of support by shifting their weight in response to visual feedback provided by a personal computer, in addition to the therapist’s guidance, encouragement and feedback. The use of visual motion and active motion of the trunk muscles in UN rehabilitation have been reported previously (15, 16). Although the KAT has been shown to be effective in improving balance in stroke patients, its effects on UN have not been investigated previously (17).
The aim of this study was to investigate the effects of the KAT on UN and functional outcomes in patients with stroke in a rehabilitation setting. We hypothesized that KAT as an adjunct to a conventional rehabilitation programme would result in better outcomes than conventional therapy alone.
This was an assessor-blinded randomized controlled clinical study. Ninety stroke patients with UN who were admitted for rehabilitation in the Department of Physical Medicine and Rehabilitation, Ankara University Medical Faculty, from February 2013 to December 2014 were screened. Stroke was diagnosed by a neurologist and confirmed via computed tomography (CT) scan or magnetic resonance imaging (MRI). The inclusion criteria were: having a first episode of stroke; diagnosed as having UN by Behavioral Inattention Test (BIT), such that BIT conventional score £129 or BIT behavioural score £67; ability to understand and follow commands; and ability to stand without assistance at least for 5 min. Exclusion criteria were: a history of other neurological diseases, such as polyneuropathy; impaired vision detected by visual field examination; and having cardiac, respiratory, or musculoskeletal disorders that might have hindered KAT.
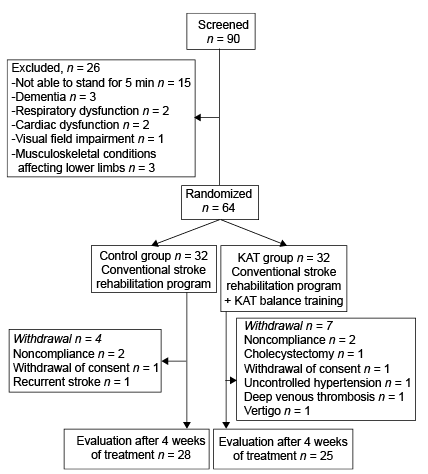
A total of 64 patients were randomly assigned to receive either a conventional rehabilitation programme (control group, n = 32) or KAT plus a conventional rehabilitation programme (KAT group, n = 32) for 4 weeks, 5 days a week. A block randomization method was used to ensure an equal number of patients were assigned to each group. The rehabilitation team evaluating the patients was blinded to group assignment. An independent research assistant (who was unaware of the baseline data) carried out the randomization procedure with a block size of 4 using computer software. Sequentially numbered, opaque, sealed envelopes were used to conceal the randomization sequence. During the study, 4 patients from the control group and 7 from the KAT group dropped out, due to several reasons. A final total of 28 patients in the control group and 25 in the KAT group completed the study. The flowchart of study participants is shown in Fig. 1.
The study protocol was approved by the ethics committee of Ankara University Medical Faculty. All patients provided informed consent and the study was carried out in compliance with principles of the Declaration of Helsinki.
Fig. 1. Flow chart of patients through the study.
Both therapy groups participated in a conventional stroke rehabilitation programme, 5 days a week, 2–3 h/day for 4 weeks. The conventional programme is tailored to the patient’s needs and consists of physical and occupational therapy. Physiotherapy was based on Bobath’s therapeutic approach and focused on positioning, postural control, weight-shifting, facilitation techniques, range of motion and progressive resistive exercises, and gait training. Physical therapy modalities were used and assistive devices were provided if necessary. Speech and language therapies were also provided if needed. Regarding the conventional therapy for UN, the patients were verbally instructed and encouraged to pay attention to the neglected part of the body and space during ADL. In addition, visuo-spatial scanning training by paper and pencil tasks (reading, copying and drawing, and analysing the form and content of complex visual stimuli searching for specified elements in pictures) were administered as a part of occupational therapy.
The KAT group received a 4-week balance training programme. 5 times per week. with a session-duration of 20–30 min. using the SportKAT® 2000. Balance training and testing were performed by the same physiotherapist. Patients wore trainers and stood on the platform without holding the handrails. The pressure bladder was placed under the platform. The level of platform stabilization varied according to pressure changes in the bladder. KAT was carried out with a high level of stability pressure until good balance was achieved, then pressure was reduced step by step as the balance improved. The movable platform was connected to a monitor displaying a cursor. Patients on the movable platform watched this cursor and shifted their weight forwards, backwards, left or right in order to keep the cursor central (static pattern) or to follow the moving cursor (dynamic pattern) on the screen.
All patients were assessed with the BIT and the Functional Independence Measure (FIM) before and after therapy. The Turkish versions of the BIT and the FIM have been validated previously (18, 19). Patient data, including demographics (age, sex), time since stroke, hemiparetic side (right or left), lesion type (haemorrhagic or ischaemic), and dominant hand were also recorded.
The BIT was designed for standardized assessment of unilateral spatial neglect, and supplied information about problems in daily life caused by neglect. It comprises 6 conventional pencil-and-paper subtests (line crossing, letter cancellation, star cancellation, figure and shape copying, line bisection, and representational drawing) and 9 behavioural subtests reflecting various aspects of daily life (picture scanning, telephone dialling, menu reading, article reading, telling and setting time, coin sorting, address and sentence copying, map navigation, and card sorting). Maximum scores for the conventional and behavioural tests are 146 and 81, respectively. The cut-off scores for the presence of UN are £129 and £67, for conventional and behavioural tests, respectively. These scores help us to understand the functional profile of neglect and set meaningful treatment goals for patients (20, 21). The recovery rate was calculated by percentage change compared with the baseline BIT cut-off values within each group. The BIT was performed within 72 h of admission by the same occupational therapist trained in neurophysiological testing.
The FIMTM was developed in 1984 by the American Congress for Rehabilitation Medicine and the American Academy of Physical Medicine and Rehabilitation (22, 23). It is used as a universal assessment tool for functional status in the Uniform Data System for Medical Rehabilitation (24). The physical/motor function and cognitive function include 13 and 5 items, respectively. These 18 items are also grouped in 6 subscales: self-care, sphincter control, transfers, locomotion, communication and social cognition. Each item with a 7-point scale is ranged from complete independence (score = 7) to total assistance (score=1). The FIM assessments were performed within 72 h of admission by our rehabilitation team, which included a physical therapist (who assessed transfers and locomotion), occupational therapist (who assessed self-care except bathing), speech therapist (who assessed communication), psychologist (who assessed social cognition) and nurse (who assessed sphincter control and bathing subscales of self-care). All members of the rehabilitation team are trained in the assessment of FIM instrument (version 4.0) since its adaptation into Turkish (19, 25).
Improvements in the classical and behavioural tests of the BIT and motor and cognitive scores of the FIM were compared within and between groups.
Median (25th–75th percentiles) for metric variables and frequency (percentage) for categorical variables were used for descriptive statistics. A complete case analysis approach was used. In order to compare groups in terms of improvements, percentage change [((after therapy-baseline)/baseline) × 100] was calculated. The χ2 test was used to compare 2 independent groups for categorical variables, and the Mann–Whitney U test was used for metric variables. The Wilcoxon signed-rank test was used to evaluate within-group changes. p < 0.05 was considered statistically significant. No adjustments for multiple comparisons were made. As there was no previous study using the BIT cut-off scores as the primary outcome measure for the recovery of neglect, a priori power analysis could not be performed. Post hoc analysis, based on the recovery rate of neglect, revealed a power of 0.14 for conventional BIT and 0.55 for behavioural BIT in the current sample of 25 patients in the KAT group and 28 patients in the control group.
Demographic and clinical characteristics of the patients are shown in Table I. The median ages of the control and KAT groups were 63 and 62 years, respectively. Thirty-two patients (60.4%) were men and 49 (92.5%) had right hemisphere stroke. No significant differences were detected between groups with respect to age, sex, education, time since stroke, hemiplegic side, dominant hand, and type of lesion.
Table I. Demographic and clinical characteristics of the 2 groups
The BIT scores of the 2 groups are shown in Table II. When baseline values were compared, the BIT conventional total score was found to be significantly higher in the KAT group compared with the control group (median: 98 in the control group and 110 in the KAT group, p = 0.022). There was no significant difference in terms of baseline behavioural BIT score between the 2 groups (median: 50.5 in the control group, 56 in the KAT group, p = 0.137). The conventional and behavioural BIT scores were significantly improved by therapy in both groups (p < 0.001) (Table II). Regarding the subtest results, 4 subtests of conventional BIT in the control group and 5 subtests in the KAT group significantly improved after therapy (Table II). Five subtests of the behavioural BIT in the control group and 7 subtests in the KAT group also improved significantly. When the percentage change in BIT scores (conventional and behavioural total scores) from baseline to after therapy were compared between the 2 groups, no statistically significant difference was detected in any of the tests and subtests.
Table II. Comparison of Conventional Behavioral Inattention Test (BIT) sub-tests scores before and after treatment
The results of the FIM scores at baseline and after therapy are shown in Table III. When baseline values between the 2 groups were compared, the median FIM® motor score was found to be significantly higher in the KAT group (median: 34.5 in the control group and 43 in the KAT group, p = 0.046), indicating better physical function at admission. The FIM scores improved significantly in both therapy groups except the FIM cognitive score in the KAT group. When percentage change in the FIM® scores from baseline to after therapy were compared, no significant difference was detected between the 2 groups (Table III).
Table III. Comparison of Functional Independence Measure (FIMTM) scores before and after treatment
The recovery from neglect by therapy, based on the conventional and behavioural BIT cut-off scores, is shown in Table IV. According to the behavioural BIT, the recovery rate was 40% in the KAT group and 17.9% in the control group. The recovery rates according to the conventional BIT were found to be 16% and 10.7% in the KAT and control groups respectively. Thus, the percentage of recovered patients was prominently higher in the KAT group based on both conventional and behavioural tests. Although the recovery rates did not reach statistical significance between the 2 groups, the higher improvement rate in the behavioural BIT in the KAT group was considered clinically important.
Table IV. Recovery of neglect
The percentage of patients who recovered from neglect was prominently higher in the KAT group compared with the control group, although this did not reach statistical significance. To the best of our knowledge this is the first randomized controlled trial investigating the effects of KAT in stroke patients with UN.
The balance system used in the present study has been shown to improve the symptoms of UN. We postulated that this effect might be caused by increased body awareness and motor responses by visual stimulation and gravitational inputs. Previously, it was demonstrated that gravitational inputs could modulate unilateral spatial neglect (26). In addition, body awareness induced by training has been shown to be an effective method in the treatment of visuospatial neglect (27). The balance platform enhances postural control system of the body by giving feedback to the patient for processing of visual, vestibular, and somatosensory inputs (28). The patient looks at a cursor on a screen and attempts to keep it at the centre by shifting their weight in various directions. Therefore, motor response to this visual stimulus on the screen requires a number of processes that integrate eye, head and trunk movements in order to adjust the centre of gravity. Previous studies suggest that a combined therapeutic approach is better than isolated therapy for UN (29, 30). In this study, we used the balance platform as an adjunct to conventional therapy, expecting better outcomes compared with conventional therapy.
Traditional procedures for assessing UN generally include visual aspects that focus on paper and pencil activities, such as line crossing, simple drawing and copying tasks (31–33). These traditional tests tend to ignore behavioural components of neglect that might seriously restrict ADL, as reported by many physicians and therapists (4, 34). Assessment of everyday problems faced by people with UN have become more important over time. Therefore, the BIT was developed in 1988, containing not only conventional, but also behavioural subtests, including picture scanning, telephone dialling, menu or article reading, telling and setting time, coin or card sorting, address copying, and map navigation (20). In fact, health professionals dealing with patients with UN consider the improvements in daily life to be more important for clinical follow-up and evaluation of treatment response. In accordance with this consideration, the improvement rates observed in the present study have been reflected prominently by the behavioural BIT rather than the conventional BIT. Despite the statistical insignificance, the recovery rate observed in the KAT group was almost 2.5 times greater than in the control group. Hence, it can be considered a clinically meaningful improvement. Post-hoc power analysis revealed that 40 patients in each group would be required to reach a power of 0.70 at a significance level of 0.05 for the recovery rate of behavioural BIT. In the present study, the improvement observed in ADLs by use of the balance system was not found to be superior to conventional therapy. This might be explained by several reasons. It has been reported that the conventional ADL measures, such as the FIM® and Barthel Index, do not provide direct information on recovery from UN (35–37). Therefore specific scales measuring neglect-related limitations on activity and participation are proposed (37). In addition, the relatively limited sample size might not have detected the changes that were small in magnitude.
The present study has some limitations. First, due to the nature of KAT, only patients who could stand without assistance for at least 5 min were recruited, and this limited inclusion of all stroke patients with UN. Secondly, there was a near significant difference at the baseline FIM motor scores between 2 groups, which could have affected the results. However, no statistically significant difference was detected between the 2 groups regarding changes in motor FIM from baseline to after therapy. Thirdly, as there was no previously established application of KAT for neglect, the duration and intensity of KAT used in the present study was compatible with the balance training. Whether the longer duration of therapy might have been more beneficial remains unanswered. Fourthly, as the study is considered underpowered based on the post-hoc power analysis, current results must be interpreted with caution against type II statistical error.
Kinaesthetic ability training may be an efficient intervention for the rehabilitation of neglect in stroke patients. As a promising new means of rehabilitation of stroke patients with UN, it may be useful as an adjuvant therapy to conventional neurorehabilitation practice. However, further studies with larger samples are needed to confirm its effectiveness and to determine the optimum duration and intensity of training, using UN-specific outcome measures for activity and participation.
Funding. This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize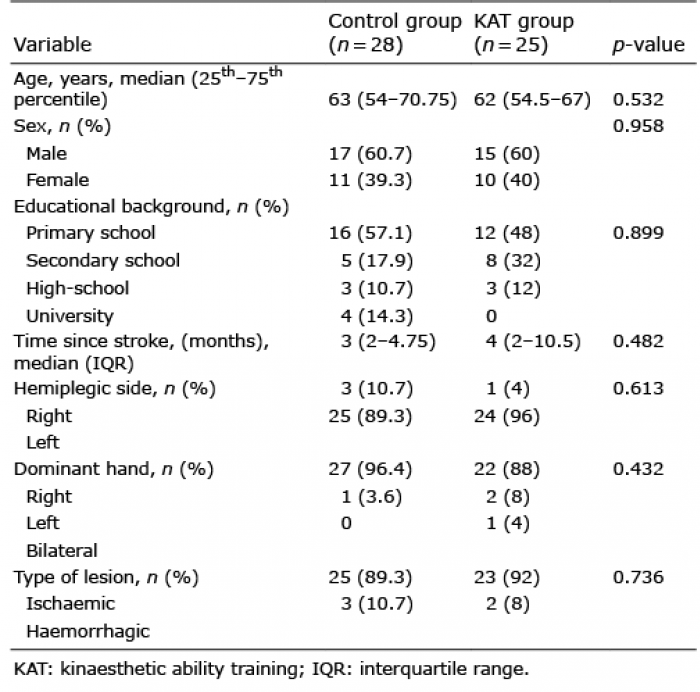 Click to show fullsize
Click to show fullsize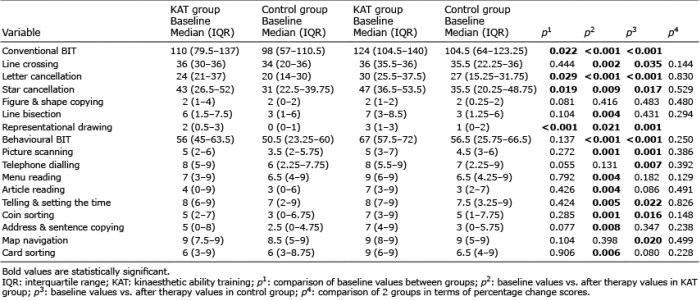 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize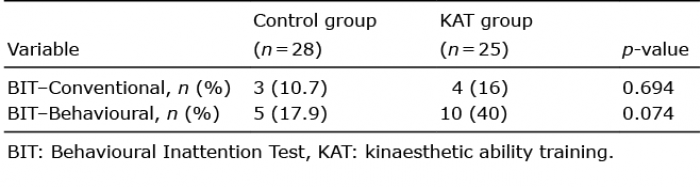 Click to show fullsize
Click to show fullsize