
School of Health Administration, Texas State University, San Marcos, TX, USA
Background: Military veterans returning from a combat zone often face mental health challenges as a result of traumatic experiences. The veteran in the United States has been underdiagnosed and underserved. Since its advancement in the 1990s, telemedicine has become a more prevalent means of delivering services for post-traumatic stress disorder among veterans in the United States, but its adoption is not ubiquitous.
Objective: To clarify the association of telemedicine and the treatment of veterans with post-traumatic stress disorder through identification of facilitators and barriers to the adoption of the modality.
Methods: Reviewers analysed articles from CINAHL and PubMed databases, using relative key words, selecting the 28 most germane to the study objective.
Results: The most common adoption facilitators were: improving access to rural populations of veterans (22%), effective treatment outcomes (16%), and decreased costs related to care (13%). The most prevalent barriers were: veterans lacking access to necessary modalities (25%), availability of physicians competent in post-traumatic stress disorder treatment (20%), and complications with technology (20%). Five themes surfaced for facilitators: accessibility, effectiveness, cost reduction, positive patient perception, and supportive community; and 5 themes for barriers: access to technology, technical complications, physician availability, negative patient perception, and uninformed patients.
Conclusion: This literature review identifies cost and outcomes-effectiveness. The association of telemedicine with the treatment of veterans with post-traumatic stress disorder is feasible, beneficial and effective.
Key words: telemedicine; post-traumatic stress disorder; telerehabilitation.
Accepted Nov 7, 2017; Epub ahead of print Apr 26, 2018
J Rehabil Med 2018; 50: 385–392
Guarator address: Clemens Scott Kruse, School of Health Administration, 601 University Dr., San Marcos, TX 78666, USA. E-mail: scottkruse@txstate.edu
Telemedicine has faced several barriers over recent decades, including technological and equipment challenges, costs and regulation (1), but, recently, these barriers have decreased. Advances in technology and recent healthcare reforms, such as the American Recovery and Reinvestment Act (ARRA), the Health Information Technology for Economic and Clinical Health (HITECH) Act, and the Affordable Care Act (ACA), support the coordination and alignment of healthcare systems by means of such technology. In 2010 President Obama promoted “Connect America”, which, among other things, encouraged medical networks to leverage technology to improve medical care through remote services, such as telemedicine, within the field of mental health (2).
The US Department of Veteran Affairs (VA) reports that approximately 31% of Vietnam War veterans experienced post-traumatic stress disorder (PTSD), 10% of Gulf War veterans, 11% of veterans of the war on Afghanistan, and 20% of veterans of the Second Gulf war (3). This is high prevalence in comparison with 7.8% of all Americans with PTSD (3). Access to mental health services can play a pivotal role in a service member’s plan of care during this often vulnerable and difficult time. However, the VA system involves limited facilities and long waiting times, which can become overwhelming and discourage veterans from pursuing evaluation and treatment of PTSD.
In 2014, an independent review revealed that veterans endured significant waiting times before seeing a primary care provider, and that the VA was falsifying scheduling records to avoid retribution. Of the sample reviewed, the mean waiting time for a first appointment was 115 days, and although officials reported that less than half of patients waited for more than 2 weeks, findings showed that 84% waited at least that long (4). In response, President Obama passed the Veterans Access, Choice, and Accountability Act, which allocated approximately $15 billion US dollars to improving veterans’ access to healthcare through increased VA facilities, more providers, and alternative healthcare options in light of VA delays in care (5). Now, 2 years later, while improvements have been made, waiting times have not been significantly impacted.
Given the prevalence of PTSD among US veterans (30.9% for males and 26.9% for females) (5), additional modalities of care should be considered that can improve access to veterans in order to diagnose and treat veterans with PTSD. An evaluation of facilitators and barriers to telemedicine among veterans with PTSD could be of value. Pursuant with the World Health Organization (WHO), this systematic review uses the terms telemedicine and telehealth synonymously, defined as:
“The delivery of health care services, where distance is a critical factor, by all health care professionals using information and communication technologies for the exchange of valid information for diagnosis, treatment and prevention of disease and injuries, research and evaluation, and for the continuing education of health care providers, all in the interests of advancing the health of individuals and their communities (6)”
Telecare is a seldom-used term, used synonymously with telemedicine.
The US National Institutes of Mental Health, associates mental health comorbidities as depression, anxiety, and substance abuse as secondary diagnosis PTSD (7). Facilitators and barriers continue to be evaluated and considered within the industry. Overarching facilitators identified in the literature are: access, cost reduction, effectiveness, positive patient perception, and community support. Overarching barrier themes include: limited access to technology, physician availability, technology complications, and uninformed patients.
The objective of this systematic review is to clarify the association of telemedicine and the treatment of veterans with PTSD through the identification of facilitators and barriers to the adoption of the modality.
The structure of the review follows the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) (8). The review itself has not been registered. Studies were eligible for selection if they were published between the years 2010 and 2016, and whose topics were germane to the research question of this review. Articles had to make some association between telemedicine and PTSD for a veteran population as well as mention at least onez facilitator or barrier. This review collected data from articles published in the last 6 years relevant to the state of telemedicine since “Connect America” was promoted. The primary research question was to clarify the association of telemedicine with veterans diagnosed with PTSD through the identification of facilitators and barriers to adoption. The search and selection process conducted for the articles used for this review are illustrated in Fig. 1.
Fig. 1. Literature review process.
The review was structured from PRISMA, using the protocol outlined by the Assessment for Multiple Systematic Reviews (AMSTAR) (9). The authors structured and implemented a systematic review by searching CINAHL and PubMed databases. These databases were selected due to their common availability, making this review more duplicable, and because they have been used in other systematic reviews in the area of telemedicine (10, 11). The search string used for both databases was a combination of key terms, found in the Medical Subject Headings (MeSH) and Boolean operators: (telemedicine OR telehealth OR telecare) AND (PTSD OR post traumatic stress disorder OR post-traumatic stress disorder). Searches were conducted during the period 20–30 November 2016.
Prior to application of the publication date filter, the results totalled 220 articles. After application of the date filter, the number of articles reduced to 176. Among the 5 authors, abstracts for these 176 articles were distributed in a way that ensured that each article was read by at least 2 authors. Each author kept an independent record of recommendations and observations about each article for later discussion. During a consensus meeting, the authors shared their recommendations. If the recommendation to keep or discard was in agreement, then the recommendation stood. If there was disagreement as to whether to keep or discard, the notes were brought up for discussion. A consensus was reached by the end of the meeting. The final sample of articles for analysis was 28.
The goal was to identify facilitators and barriers to the adoption of telemedicine in the treatment of veterans with PTSD. Based on this aim, the data items sought were facilitators and barriers.
To overcome selection bias, each member of the review team was instructed to keep independent notes. This helped to control the tendency to focus in on 1 or 2 observations made by one member of the group early in the process. Publication bias was discussed early in the process. To control for publication bias, members of the review team read each article carefully to identify references to any unpublished studies, otherwise known as grey literature, but none were identified.
The search in both PubMed and CINAHL resulted in hundreds of relative articles. Collectively, the reviewers created a literature matrix to narrow the results down to the specific topic relating to veterans and PTSD. Abstracts were first reviewed by at least 2 reviewers and then, from the resulting sample, articles were reviewed by at least 2 reviewers. Articles were removed from eligibility for various reasons.
Articles were removed based on narrowness of topic (i.e. they did not encompass the PTSD and veteran-specific focus), articles that were too broad and not germane to the topic (i.e. veterans not mentioned), small sample size (less than 30), case studies, and if variables such as depression, general anxiety, smoking, and substance abuse were very prominent (which was not our primary research objective). If comorbidities were secondary to the reviewers’ primary focus of PTSD, respective articles were accepted. The first consensus meeting facilitated discussion and identified the final list of articles for analysis.
The remaining 28 articles selected for analysis were then divided up among members of the team so that each article was read by at least 2 authors. Independent notes were kept on facilitators and barriers for later discussion. At a second consensus meeting, the group shared their observations and a composite list of facilitators and barriers was compiled in a literature matrix. An affinity matrix was created to count the number of articles identifying each of the facilitators and barriers.
At this same meeting, the notes for each article were again reviewed among the group to help identify common themes. Through a careful discussion of what was read and observed, the team identified the common themes that ran through the entire sample. These 5 themes were then organized so as to enable inferences to be made.
Reviewers screened 220 results from both CINAHL and PubMed, applied filters for date published, and reviewed abstracts in detail to identify the final sample. A total of 28 works, published during the years 2010 to 2016, that focused on facilitators and barriers for telemedicine as a treatment method of PTSD in veterans, were identified.
These 28 articles were carefully evaluated for facilitators and barriers, followed by common themes. Five common themes were identified for both facilitators and barriers. Approximately 71% (20/28) used videoconferencing as the telemedicine intervention, while the others used the telephone. No other form of telemedicine was found in our search.
Reviewers recorded observations and findings from the literature in a thorough table that can be found in Table SI1. Out of a total of 90 factors, 68 were identified as factors of facilitation (75.5%) and 22 as barriers to adoption (24.5%). Authors created affinity matrices to illustrate the frequencies of the factors identified in the literature. These matrices are shown in Tables I and II.
Table I. Facilitators to adoption of telemedicine to treat veterans with post-traumatic stress disorder (PTSD)
Table II. Barriers to adoption of telemedicine to treat veterans with post-traumatic stress disorder (PTSD)
Facilitators. The most commonly discussed facilitator was “improved access for rural area veterans”, which was identified in 15 out of 68 total occurrences (22%) (12, 16–18, 20, 23, 26, 28–30, 33, 34–37). A benefit of telemedicine identified in the literature was its ability to increase access to care for patients. Veterans living in rural areas face increased difficulties and obstacles with regards to obtaining adequate care. Telehealth can provide faster and more convenient access to healthcare where shortages exist in rural areas, as it remotely delivers healthcare services and information via telecommunication technology.
“Effective treatment outcomes” was the second most discussed facilitator, which was found in 11 out of 68 occurrences (16%) (13, 14, 16–18, 21, 25, 32, 34–36). Telemedicine enabled a more rapid diagnosis and treatment process. This greater efficiency often resulted in improved symptom reduction of PTSD and related comorbidities, such as anxiety and depression.
“Decreased costs related to care (including travel, missed work, etc.)” was found in 9 out of 68 occurrences (13%) (12, 14, 16, 17, 25, 26, 33, 34, 37). Studies demonstrated that telehealth served as a means to reduce costs for both patients and providers. This was identified in direct costs, such as reduced clinic and waiting-room space, and indirect costs, such as time for the patient to take off work, drive to the appointment, and possibly have to arrange childcare.
Eight out of 68 (12%) occurrences discussed “increased feelings of comfort, safety, and privacy” as a facilitator, meaning that veterans were particularly at ease with the use of telemedicine as a form of treatment (12, 16, 17, 28, 31, 35–37).
“General interest/acceptance by veterans” was discussed in 7 out of 66 occurrences (10%) (13, 14, 27, 31, 33, 35, 36).
“Veterans have access to necessary modalities (mobile devices, laptops, computers, etc.)” was another facilitator observed in the literature. This facilitator was identified in 6 out of 68 (9%) occurrences (14, 18, 19, 27, 29, 30). Maintaining a good relationship between the provider and patient through telemedicine may be difficult, as the in-person contact is removed; however, 3 out of 68 occurrences (4%) identified “unaffected patient-provider relationship” as a facilitator to telemedicine adoption among veterans with PTSD (22, 27, 33). “Patient independence/autonomy” was identified in 3 out of 68 occurrences (4%) (14, 17, 36). Telemedicine allowed patients to feel more in control and aware of their symptoms. Lastly, both “ease of use” (9, 19) and “fewer scheduling conflicts for providers” were identified in 2 out of 68 occurrences (3%) (17, 25). The last 2 facilitators, each mentioned once out of 68 occurrences (2%) were “involvement of loved ones” (19) and “social network engagement” (17).
Barriers. Five barriers to the adoption of telemedicine to treat US military veterans for PTSD were identified in the literature. The barrier most commonly mentioned was “veterans without access to necessary modalities (mobile devices, laptops, computers, etc.)”, which was identified in 5 out of 20 occurrences (25%) (12, 16, 17, 26, 35). Veterans residing in rural populations, especially, had difficulty obtaining access to technology or high-speed internet. Another major barrier authors observed during the analysis was the “availability of physicians with competence in PTSD treatment”, identified in 4 out of 20 occurrences (20%) (26, 27, 36, 37). “Complications with technology” was another significant barrier, identified in 4 out of 20 occurrences (20%) (16, 30, 35, 36).
The barrier “providers with limited technology” was found in the literature 3 out of 20 times (15%), the barrier “negative expectations of outcomes by veterans” was identified 2 out of 20 times (10%) (21, 22). Finally, the barriers of “limited exposure/prior knowledge of telehealth” and “confidentiality concern” were only identified once out of 20 occurrences (5%); however, one article identified the former as under-reported (21). The latter barrier is rather surprising with the increased use of technology and cloud-based telehealth modalities (14).
Based on the facilitators and barriers identified in the literature, authors were able to identify 5 major themes for both facilitators and barrier regarding the adoption and utilization of telemedicine as a method of treatment for veterans with PTSD. The facilitator themes identified were: accessibility, effectiveness, cost reduction, positive patient perception, and supportive community. The 5 overarching themes identified for barriers were: access to technology, technical complications, physician availability, negative patient perception, and uninformed patients. These themes are described below.
Accessibility. The literature revealed that accessibility was the most prominent theme. With the use of telemedicine, the population of veterans residing in rural areas was able to receive easier access to treatment (12, 16–18, 23, 26, 28–33, 35). The use of telemedicine as the modality of care eliminated several common barriers from the traditional clinical setting, such as geographical isolation, transportation issues, and scheduling conflicts (22, 25, 31, 32). Similarly, telemedicine adoption resulted in earlier engagement and improved overall coverage of veterans with PTSD (31, 32).
Due to the various options of platforms for delivery of telemedicine (i.e. mobile devices, tablets, laptops, desktops) to which most veterans have access, telemedicine provides promising convenience to this population (6, 7, 9, 17, 18, 27). Similarly, the literature indicated that most veterans viewed telemedicine software on their devices as easy to use and helpful in their treatment, even when they were not communicating directly with a physician. Specifically, reminders and prompts of helpful coping skills as well as the ability to track and view progress and patient information created a sense of self-awareness and autonomy in the care process (9).
Effectiveness. In a variety of studies treatment through telemedicine proved to be equally as effective as traditional treatment. This equality of outcomes was demonstrated through symptom reduction related to PTSD, as well as reduction in symptoms of comorbidities related to PTSD, such as anxiety and depression (2–6, 13, 19–21, 24, 26). Although no difference in dropout rates was observed when comparing in-person treatment with telemedicine-based treatment, studies did show that dropouts engaged in the telemedicine method for a longer period of time before deciding to discontinue treatment (20, 25). In addition, telemedicine effectiveness was unaffected by age, ethnicity, or demographics of veterans (23, 24, 26).
Cost reduction. From the patient perspective, telemedicine reduced out of pocket costs due to the elimination of frequent hospital or clinic visits. Veterans also benefitted from decreased costs related to travel, such as fuel or bus tickets. Opportunity costs, such as missing work, travel time, and accommodation needed for veterans with small children also decreased due to the convenience of telemedicine-based treatment (1, 4, 5, 9, 13, 16, 20, 22, 25).
Providers experienced an overall reduction in the cost of treatment of veterans with PTSD, as well as the ability to engage more patients (21, 33).
Positive patient perception. Veterans’ perception of telemedicine was found to be a major theme associated with facilitation of telemedicine advancement. Based on surveys, veterans were generally interested and accepted telemedicine as a delivery method (3, 13, 15, 31–33, 35). They felt confident in positive outcomes and enjoyed the practicality of treatment through an easy-to-use electronic platform. Veterans also expressed that their comfort with telemedicine stemmed partially from the ability to bypass the stigma associated with receiving mental healthcare services (12, 16, 17, 26, 32–34, 35, 24). Not only were veterans more comfortable with the privacy offered by receiving treatment in their own homes, but they were also more comfortable that telemedicine enabled the avoidance of trauma cues (e.g. pictures, uniforms, other veterans) that are often present in VA clinics, as well as heavily populated areas or travelling long distances, which may bring about anxiety (3, 17, 19, 32).
The literature also revealed that the patient-provider relationship remained positive for most veterans. Veterans expressed that comfort, trust, connection, and helpfulness remained regardless of the lack of in-person contact (22, 27, 33).
Supportive community. Supportive community was the least prominent facilitating theme found in the literature, but emerged from 2 specific findings: the ability for loved ones to be involved and present during the care process due to telemedicine-based treatment, and group video teleconferencing allowing veterans to meet one another and develop a social network of individuals with similar issues (5, 7). Both act as supporting parties in the treatment process and may assist in adherence and effectiveness.
Access to technology. Limited access to technology was the most prominent theme discussed throughout the literature. Veterans without access to mobile devices or internet-capable devices able to support the software used in delivery cannot reap the benefits offered by telemedicine. Similarly, affordability of high-speed internet may be an issue for patients and providers, especially those in rural areas (12, 16, 17, 28, 35). Upfront costs of technology, devices, software, and other logistics (i.e. the ability to troubleshoot issues that arise with software) may surface as significant concerns for hospitals with limited resources (16, 28, 35).
Technical complications. Technical difficulties were another major barrier theme that authors identified. Complications, such as slow internet, software glitches, difficulties sending and receiving messages and homework assignments, and complicated installation, were all possible issues discussed in the literature. Similarly, providers must have the means to provide maintenance for software as necessary (16, 30, 32, 35).
Physician availability. A shortages of physicians is an ongoing problem that arises in healthcare, and there is no difference when it comes to mental healthcare providers. The availability of physicians with competence in the treatment of PTSD is a major concern for the advancement of telehealth (27, 28, 32, 22). As telemedicine allows providers to reach more veterans, the demand for physicians in mental health will continue to increase.
Negative patient perception. Negative patient perception and ideas about telemedicine was another prominent theme that may pose as a barrier to adoption. Studies found that some veterans had negative expectations of outcomes and did not believe that the delivery method would be as effective as in-person treatment (21–23). Although findings proved this to be false, these negative opinions may hinder the treatment process or prevent engagement in treatment completely (21).
In addition, some veterans, especially the older demographic, expressed technology as a nuisance or intolerable method of treatment. Confidentiality and privacy concerns also arose based on the articles reviewed (14).
Uninformed patients. Lack of knowledge about telemedicine was the last identified barrier theme. Limited or no exposure to telemedicine and unawareness of it as a modality of care can serve as a barrier to its request by veterans and its growth as a form of treatment (21). Similarly, this theme may fuel the above theme by allowing negative thoughts to perpetuate due to lack of knowledge of the benefits and effectiveness of telemedicine.
Findings from this review are relatively similar to that of other reviews conducted previously. The themes of the barriers and facilitators identified for veterans are parallel to themes identified pertaining to telemedicine delivery and utilization research not specifically focused on veterans (1). As expressed in the literature, telemedicine should not be viewed as a means to improve effectiveness or outcomes of treatment. Rather, it should be used as a tool to expand the reach of treatment and to engage more veterans in seeking treatment for PTSD. More specifically, although retention rates (based on percentage) have not been shown to improve by using telemedicine as a treatment method, the value of telemedicine remains, due to the fact that more veterans (based on raw number) are reached and therefore, more veterans overall are completing treatment for PTSD (22). Specific cost savings were not found in the literature on US veterans, but other studies on other populations have found specific numbers. In a review on telemedicine that focused on the American Native population, it was found that, for every US dollar spent on telemedicine, US$11.50 was saved in travel and child-care expenses by the patient, without any decrease in quality outcomes (38). A study of cancer support groups identified between 2 and 5 h of travel each way was saved for Native Americans, which saved a range of US$50 to $200 (39).
Authors were able to identify limitations that existed in this review. Literature focusing on the barriers of veterans specifically was fairly scarce, focusing more on why telemedicine would be a viable option for delivery of mental health services. Consequently, there was little discussion on the topic of stigma as barrier, which is a fairly common issue that veterans face, and which may play a more significant role either as a facilitator or barrier to adoption and utilization of telemedicine (14). Similarly, discussion of licensing issues and treatment across state lines were also absent in the literature pertaining to factors affecting veterans. This is a barrier commonly conveyed in the literature in regards to physician availability, that was not present in the findings of this review.
Another limitation of this study is the lack of availability of information regarding how the level of severity of PTSD symptoms or the presence of other severe comorbidities may affect the success of telemedicine as a treatment method. Studies included in this review often excluded individuals from the final samples if comorbidities were present or if the individual had a high level of severity of symptoms.
We noted that 71% of the interventions involved videoconferencing, while the others used the tele
phone. Although we identified a litany of facilitators and barriers associated with our review, it is well known that videoconferencing and telephone interventions have different facilitators and barriers. A limitation that this highlights is that the current study did not separate the facilitators and barriers, as was done in other research. In addition, although we identified several themes, we did not analyse them based on the modality of intervention.
Lastly, very little information was available on specific costs associated with telemedicine implementation, and therefore they were not quantifiable. It would have been helpful to compare savings between populations.
Based on findings from this review, further research may focus on barriers that veterans may face, in order to identify ways to overcome those barriers and improve adoption of telemedicine in this population. Future research may also focus on the effectiveness of telemedicine in more severe cases of PTSD, especially because these individuals may be more likely to avoid seeking treatment. In addition, telemedicine offers a solution to the lengthy waiting times discovered in the VA system, which ultimately discourage veterans from seeking care.
Telemedicine offers a means by which PTSD can be more rapidly diagnosed and treated among veterans. A review of facilitators and barriers reveals utilization challenges, while reinforcing realized and potential benefits. Outcome studies show that telemedicine is an effective and efficient treatment option for veterans who would rather receive care remotely or whose geographical locations leaves them with limited options and increased difficulties. As identified by the WHO, telemedicine can increase access to care, and many veterans with mobility issues need the treatment that telemedicine can provide.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize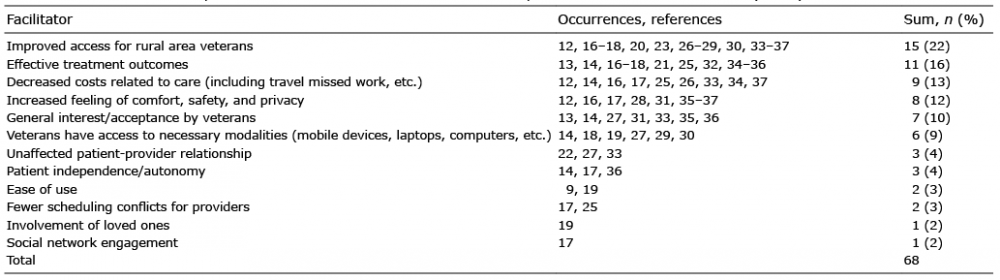 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize