
From the 1Department of Orthopaedics and Traumatology, The Chinese University of Hong Kong, Shatin, New Territories, 2Department of Orthopaedics and Traumatology, Queen Elizabeth Hospital, Kowloon, and 3Department of Medicine and Therapeutics, Prince of Wales Hospital, Shatin, New Territories, Hong Kong SAR, China
Objective: To investigate the effectiveness and cost of an 18-month multi-disciplinary Comprehensive Fragility Fracture Management Program (CFFMP) for fragility hip fracture patients.
Design: Prospective cohort study.
Patients: Elderly patients with hip fracture were recruited at their first postoperative follow-up in 2 district hospitals. The intervention group comprised patients from the hospital undergoing CFFMP, and the control group comprised patients from another hospital undergoing conventional care. CFFMP provided geri-orthopaedic co-management, physician consultations, group-exercise and vibration-therapy. Timed-up-and-go test (TUG), Elderly Mobility Scale (EMS), Berg Balance Scale (BBS) and fall risk screening (FS) were used to assess functional performance. Incidences of falls and secondary fractures, the cost of the programme and related healthcare resources were recorded.
Results: A total of 76 patients were included in the intervention group (mean age 77.9 years ((standard deviation; SD) 6.1) ) and 77 in the control group (79.9 (SD 7.2)), respectively. The re-fracture rate in the control group (10.39%) was significantly higher than in the intervention group (1.32%) (p = 0.034). The intervention group improved significantly in TUG, EMS and FS after a 1-year programme. The overall healthcare costs per patient in the intervention and control groups were US$22,450 and US$25,313, respectively.
Conclusion: Multi-disciplinary CFFMP is effective, with reduced overall cost, reduced length of hospital stay and reduced secondary fracture rate. The rehabilitation community service favours rehabilitation and improved quality of life of hip fracture patients.
Key words: fragility hip fracture; functional outcome; cost; multidisciplinary management programme; secondary fracture.
Accepted Nov 17, 2017; Epub ahead of print Dec 20, 2017
J Rehabil Med 2018; 50: 00–00
Correspondence address: Kwok-Sui Leung, Department of Orthopaedics and Traumatology, 5/F, Lui Che Woo Clinical Sciences Building, The Chinese University of Hong Kong, Shatin, New Territories, Hong Kong SAR, China. E-mail: ksleung@cuhk.edu.hk
Fragility hip fracture is one of the most serious consequences of falls, accounting for most deaths and costs of fall-induced injuries in elderly patients. Most patients with fragility hip fractures need surgery to facilitate early recovery and regain independence. However, impaired mobility and lack of support services (e.g. escort to hospital) in the early discharge period discourage further rehabilitation, thus adversely affecting complete functional recovery. Sustained rehabilitation is needed for maximal functional recovery and prevention of secondary fractures. Hospitalization, rehabilitation and post-fracture care require a high level of healthcare resources. The World Health Organization (WHO) (1) report the mean management costs of falls and fractures range from US$6,646 in Ireland to US$17,483 in the USA. The impact on the healthcare system is even greater if secondary fractures occur. This cost is increasing with the ageing population, and is forecast to rise dramatically, to US$240 billion worldwide, by 2040.
The effectiveness of multidisciplinary fragility fracture management programmes, including geri-orthopaedic co-management, osteoporosis treatment, physical training, continuous physician consultation and fall prevention education, have been verified (2–8). A recent study by Williams et al. (7) (FEMuR) reported that enhanced rehabilitation after hip fracture could result in an improvement in quality-adjusted life years compared with a control group; Milte et al. (6) revealed the incremental cost-effectiveness ratio of individual nutrition and exercise therapy for hip fracture patients, as $AUD28,350 per quality-adjusted life year gained in Australia; Lahtinen et al. (8) also showed the total 1-year costs of physical rehabilitation for hip fracture patients was significantly more cost-effective than routine treatment. The goal of these programmes was to maximize recovery and minimize secondary fracture rate, thus improving quality of life of patients and relieving the healthcare burden. Many countries have established different kinds of multidisciplinary fragility fracture management programmes, including the UK, USA, Canada and Switzerland (9–11).
In Hong Kong, there are no official multidisciplinary fragility fracture management programmes. However, some fall prevention programmes, including elderly talks and Tai-Chi groups, have been implemented in some elderly community centres (12), which successfully enhance fall and fracture prevention awareness of elderly people (12, 13). Hence, there is a pressing need for a comprehensive rehabilitation programme focusing on fragility fracture. We have established a Comprehensive Fragility Fracture Management Program (CFFMP) since 2007, providing a multidisciplinary programme with standardized clinical management, and a holistic care programme from the acute phase, rehabilitation phase and post-fracture phase up to 18 months. The aim of this study was to compare the effectiveness (primary outcome) and total costs from the healthcare system’s perspective (secondary outcome) of the 18-month multi-disciplinary fracture management programme with the conventional care programme for elderly patients with fragility hip fracture in Hong Kong.
This is an 18-month prospective cohort study of 2 groups of patients admitted to 2 acute hospitals with different fracture management programmes in Hong Kong. Randomization was not feasible in this study because: (i) assignment of patients to the acute hospitals depends on the location of the fracture accidents; and (ii) follow-ups were allocated to first admitted hospitals. CFFMP was established in only one hospital (Prince of Wales Hospital) and another hospital with conventional care programme (Queen Elizabeth Hospital) was the control, both implementing the same acute management protocol under the regulations of the Hong Kong Hospital Authority (www.ha.org.hk). The hospitals have standardized clinical service (e.g. type of surgery, allied health service) and facilities for hip fracture. All patients who were ≥ 65 years of age, diagnosed with recent fragility hip fracture, who attended the orthopaedic specialist out-patient department (SOPD) or emergency room during 2010–13 were invited to participate in the study. Exclusion criteria were subtrochanteric fracture, pathological fractures, living in old age homes (unable to comply with the rehabilitation programmes) or those already treated for osteoporosis, e.g. bisphosphonate, or intensive exercise training. Fall/fracture incidences were collected at every follow-up, while physical performance and quality of life were assessed at 6 and 18 months post-operatively. The study was approved by the Clinical Research Ethics Committee of the Chinese University of Hong Kong (CRE-2009.226) in accordance with the Declaration of Helsinki and was registered in ClinicalTrials.gov:NCT01382875.
The Prince of Wales Hospital (interventional group) and the Queen Elizabeth Hospital (control group) are both in well-developed urban regions in Hong Kong (Shatin and Central Kowloon, respectively). According to the 2011 census (www.census2011.gov.hk), the socio-economic status of the 2 districts were similar. Elderly people ≥ 65 years in Shatin constituted 11.4% (67,853) of the district population and, in Central Kowloon, 14.3% (41,061). The median salary in Shatin was HK$26,000 and Central Kowloon HK$24,000, while the proportion of families with low-income in Shatin was 17.5% and Central Kowloon 19.2%.
Control group care. Patients admitted to the hospital with conventional care served as controls. They received standardized management during acute stay, including anaesthetic procedures, surgical intervention, medical treatment and nursing care. Patients were then transferred to a convalescence hospital for standardized rehabilitation with daily physiotherapy and occupational therapy care (usually a mean of 10 days post-fracture). Post-acute rehabilitation at a convalescence hospital was provided depending on the patients’ condition, including daily 3 physiotherapy sessions with daily monitored walking exercise and 1 occupational consultation session to assess mental score and home safety. After discharge from the convalescence hospital, they were referred back to the SOPD of the same hospital for follow-up.
Intervention group care. The key characteristics of the intervention group included geriatrician care in an acute hospital and a multidisciplinary rehabilitation programme after discharge from the convalescence hospital.
In brief, the patients received standardized management, as in the control group, during the acute stay; in addition to orthopaedic surgeons, they had additional management by a geriatrician once pre-operative and post-operative (4). After transfer to a convalescence hospital for standardized rehabilitation, patients were discharged and referred back to the Fragility Fracture Clinic in SOPD for follow-up, and to their nearest district elderly community centres (DECC) for a 1-year comprehensive rehabilitation programme once their condition had stabilized (~6 months after operation and subject to doctors’ decision). (Note: DECCs are present in almost every housing estate and are regulated by the Social Welfare Department of Hong Kong Government (http://www.swd.gov.hk/). They provide a standardized setting, including the same scope of service, operating hours, staffing and target groups). An annual charge of US$65 was made to patients in order to enhance programme compliance (Note: US$65 is an arbitrary amount, which is affordable for most elderly people in Hong Kong), while other costs were covered by the project fund. Referring to previous reports (2–5), CFFMP provided a 1-h/week group-exercise class led by professional physiotherapists, including general mobilization exercise, strength training with cuff weights, and functional mobility training (e.g. single-leg standing, tandem walk). Patients were encouraged to practice the exercises regularly at home. It also included consultation with a physician every 3 months to provide bone health medication (anti-resorptive drugs, calcium and vitamin D), fall risk and polypharmacy counselling, and referral to osteoporosis screening. Educational talks were organized every 3 months to enhance fall prevention, and environmental safety. Whole-body vibration (35 Hz, 0.3 g peak-to-peak magnitude) was provided at 3-sessions/week, 20-min/session for one year in the DECC according to our protocol (14). The DECC rehabilitation service was restricted to referred patients and the 2 districts are geographically distinct. Patients from the control group were not able to join the DECC service.
All physical performance assessments were performed at the 18-month follow-up by an independent research technician who was blinded to group allocation.
Fall and fracture incidence. Fall incidences were monitored prospectively during the study period. A fall/fracture calendar was provided to patients for recording fall or fracture incidences and was returned at every follow-up. The definition of fall refers to resting unintentionally on the ground, floor, or lower level (14). Fragility fractures and other injuries were confirmed via the central electronic patient record of the Hong Kong Hospital Authority.
Physical performance assessment. Mobility and balancing ability of patients were assessed because these were known risk factors for recurrent fall and fractures and are related to daily living activities, including: (i) timed-up-and-go test (TUG) (15); (ii) Elderly Mobility Scale (EMS) (16); (iii) Berg Balance Scale (BBS) (12, 17), (iv) fall risk screening (FS) (18–20); and (v) ambulatory status, which recorded use of walking aids, with 5 classifications: walk unaided, walk with canes, with quadripods, with frame, and wheelchair-bound.
Quality of life assessment. Quality of life (QoL) was assessed with the Short Form-36 (SF-36) version 1 questionnaire, which measures physical component score (PCS) and mental component score (MCS) (14, 21).
Cost analysis. Cost analysis (18-month follow-up) was performed by comparing the costs of 2 rehabilitation programmes based on the 2010 Hong Kong Hospital Authority price, as our subject recruitment started in 2010. All costs were calculated based on healthcare system’s perspective and presented in 2010 US dollars ($, according to purchasing power parity (PPP) conversion rate, i.e. $1 = HKD5.638). Management costs for both groups were calculated from the total expenditure on hospitalization, all medical and allied health follow-ups, attendance at the emergency department, and management of secondary fracture (if any). Costs in the intervention group also included the costs of CFFMP, such as the joint geri-orthopaedic consultation fee, general practitioners’ consultation fee, physiotherapists’ salary, and administration cost.
All data were analysed using SPSS20.0 (IBM, NY, USA) and expressed in mean (standard deviation; SD), while cost was also expressed in median and interquartile range (IQR). Comparison of demographic and baseline data of 2 groups were performed with independent t-test and χ2 test. Independent t-test was used to compare the effectiveness outcomes between groups for continuous data; and χ2 test, Fisher’s exact test and continuity correction for other categorical data. The secondary fracture rate and fall rate were compared between groups by calculating the relative risk with 95% confidence intervals (95% CI). Paired t-test was used to compare the baseline and endpoint functional outcomes within groups. Cost analysis was performed with a Mann–Whitney U test. Two-tailed p < 0.05 was considered as statistical significance.
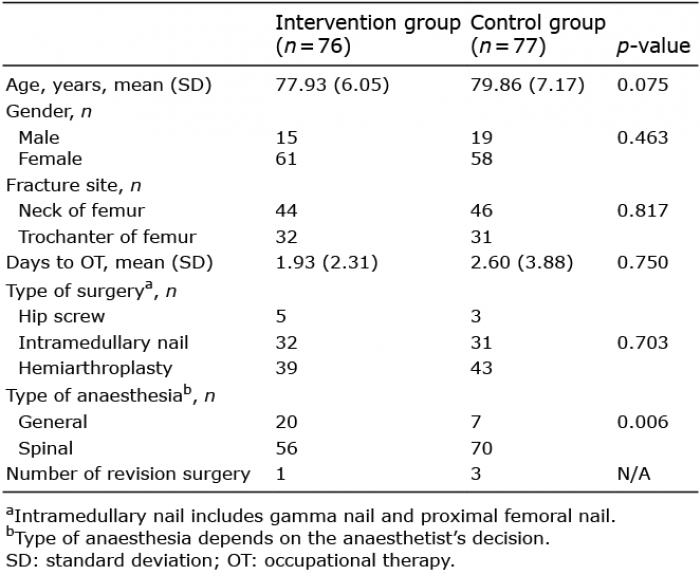
A total of 209 patients were invited to join the study and screened for inclusion and exclusion criteria. Thirty patients were excluded from the intervention group and 26 from the control group due to drop-out and defaulted assessments. A final total of 76 patients in the intervention group and 77 patients in the control group completed the study. The mean (SD) ages in the intervention and control groups were: 77.93 (6.05) and 79.86 (7.17) years, respectively with no significant difference (p = 0.075). There were no significant differences in the baseline characteristics between groups except for the type of anaesthesia (p = 0.006), which mainly depended on the anaesthetists’ decision (Table I). The compliance rate with the rehabilitation programme in the intervention group, defined as the percentage of scheduled sessions attended, was 66.1% in exercise classes and 74.9% in vibration-therapy. No cognitive impairment or mental problems were reported in any of the elderly people throughout the follow-ups.
Table I. Demographic data
At the 18-month follow-up, one patient in the intervention group had experienced secondary fracture of the humerus (1.32%), and 8 patients in the control group reported secondary fractures at the hip, spine, distal radius (10.4%) (Table II). All subjects visited the accident and emergency department and their fractures were confirmed by radiography. Six of the control group patients were re-admitted to hospital, and 4 of them had an operation due to secondary fracture. The secondary fracture rate in the intervention group was significantly lower than in the control group, with a relative risk of 0.127 (95% CI = 0.016–0.988, p = 0.034). 8 out of 76 (10.53%) patients in the intervention group fell, while 12 out of 77 (15.58%) patients in the control group fell, without statistical significance (relative risk = 0.675, 95% CI = 0.293–1.559, p = 0.353).
Table II. Total number of falls and fragility fractures reported at the 18-month follow-up
In the intervention group, significant improvements in TUG, EMS, BBS and FS (p < 0.01 for all) (Table III) were observed against baseline. The improvement was significantly better than those in control group in the EMS, FS (both p = 0.011) and TUG (p = 0.052). For BBS, the intervention group was not different from controls (p = 0.087). Also, the intervention group showed no difference in terms of utilization of walking aids (Table IV) compared with the control group (p = 0.072). For quality of life, the mean (SD) scores at the 18th month were 65.59 (19.49) and 60.70 (19.77) (Table III) in intervention and control groups, respectively, without significant difference (p = 0.425).
Table III. Comparison of functional outcomes and quality of life at the 18-month follow-up
Table IV. Comparison of mobility status in terms of utilization of walking aids between 2 groups at the 18-month follow-up
In the intervention group, the number of SOPD consultations and general out-patient department (GOPD) consultations were significantly lower than the controls (p = 0.010 and 0.024, respectively) (Table V). The expenses on acute hospital stay, orthopaedic SOPD consultations and GOPD consultations were significantly lower in the intervention group (p = 0.008, 0.010 and 0.024, respectively). Overall, the total cost in the study period was US$1,706,208 in the intervention group (76 patients) and US$1,949,121 in the control group (77 patients). The mean cost per patient was lower in the intervention group than in the control group (US$22,450 vs US$25,313). There was a mean of US$2,863 saved per patient under the CFFMP. There were a total of 9 secondary fractures reported and the mean management cost was US$16,260 per patient.
Table V. Total healthcare expenditure of the 18-month follow-up (all costs are expressed in 2010 US$ based on to purchasing power parity (PPP) conversion rate, $1 = HKD 5.638)
This study aimed to compare the effectiveness and cost of the multi-disciplinary management programme with a conventional care programme for hip fracture in elderly patients. A significantly lower secondary fracture rate was found in the intervention group. The fall rate in the intervention group (10.5%) was lower than in the control group (15.6%), despite statistical insignificance. This may have helped to reduce the risk of secondary fracture. The intervention group participated in 1-year community rehabilitation programme with group-exercise class, physicians’ consultations, and vibration-therapy. Physical training has been reported to reduce fall risks, especially muscle strength training, flexibility and endurance training (22). Also, some evidence showed that group-based exercise classes were effective in reducing fall rate and risks (23, 24). This was further substantiated by improved EMS and TUG, and decreased FS score in the intervention group. Enhanced balancing ability and functional outcomes were also associated with better functional performance, and decreased number of falls, which are keys to prevent secondary fractures and fall-related injuries (25, 26). This is important because loss of muscle and bone density is significantly accelerated within the first year of hip fracture (27). Regular physicians’ consultation can optimize patients’ medical conditions and lower fall risk related to polypharmacy. Prescribing bone health medication plays an important role to reduce future fracture risk. In Hong Kong, less than 18% of patients were prescribed with anti-resorptives after hip fracture based on the local Fragility Fracture Registry (http://www.ffr.hk).
The current study also demonstrated specific strategies in each phase of fracture management, providing continuous holistic care from hospital to the community, with standardized protocols for acute hospitalization, and multidisciplinary management of orthopaedic surgeons, geriatricians, anaesthetists and nurses (28). It was evident that early optimization and stabilization of concurrent medical problems under ortho-geriatric intervention would significantly shorten hospital stay, surgical waiting time, mortality rate and improve ambulatory status (29, 30). The intervention group in this study has shown significantly shorter acute hospital stay. These findings echo with previous findings on the impact of ortho-geriatric collaborative intervention in Hong Kong (4) as well as in the USA (28, 30), Sweden, Germany and the UK (31), which showed that geriatric co-management significantly resulted in lower-than-predicted length of stay (4.6 vs 5.2 days), readmission rates within 30 days (9.7% vs 19.4%) (28, 30), and 1-year mortality rate (28, 30). A multidisciplinary approach is crucial for complexity and multiple co-morbidities among elderly patients. Furthermore, hip fracture patients in Hong Kong are usually followed up 4–6 times within the first year of fracture regarding surgical aspect. Other medical problems associated with subsequent falls and fractures might not be well-monitored. With CFFMP, the patients were referred to physicians in the community for further management, such as osteoporosis care. The importance of physicians in post-fracture treatment, i.e. osteoporosis screening and treatment, was also addressed in some literature (32).
With better in-patient care and long-term rehabilitation follow-up, the intervention group had a significantly shorter acute hospital stay, and lower number of SOPD and GOPD visits. The shorter stay in acute hospital may associate with early stabilization of patients with ortho-geriatric co-management and no re-admission to acute hospital for secondary fracture management. The better support from community centres and physicians may lead to earlier discharge of patients from SOPD and fewer visits to GOPD. To implement the CFFMP, a mean cost of US$958 per patient was required in the intervention group. However, the reduced healthcare costs, as stated above, have covered the extra expenditure of running the CFFMP; the overall cost within 18 months was US$2,863 (per patient) lower than conventional management. There are 6,000 hip fracture cases/year in Hong Kong and this figure is expected to increase to 15,000 in 20 years due to an increasingly elderly population; annual saving is conservatively projected up to US$17,178,000 with the implementation of CFFMP. CFFMP is cost-effective to improve functional recovery, prevent secondary fracture, and reduce the overall costs of fragility fracture management.
In the current study, elderly patients attended a sustained rehabilitation programme at their nearest DECC, which are situated almost in every housing estate, due to the highly compact area of Hong Kong. Most of the patients realized that the rehabilitation programme was readily accessible and the DECC was an important factor for their adherence to the programme. Elderly patients with peer support and a sense of belonging favour long-term sustainable rehabilitation, as suggested by Wong’s study (13). Compliance with exercise classes and vibration-therapy were 66.1% and 74.9%, respectively, in the present study, which was comparable to previous studies with an adherence rate of 42.3–79% in 12-month community-based programmes (33, 34).
The limitation of this study is its non-randomized study design due to the automatic hospital assignment mechanism in Hong Kong, which might increase the risk of selection bias. Also, the confidence interval of relative risk for fracture was quite wide, which should be interpreted with caution and warrants a larger sample to confirm. In addition, this study was not conducted based on a cost-effectiveness approach, as it aims to provide an estimate of the sample size calculation for a stochastic cost-effectiveness study in the future. Instead, the sample size estimation of this study was based on our previous study (12), evaluating a multidisciplinary fall clinic for community elderly people, which showed n = 59 was needed in each arm to detect a significant difference with power of 0.8 and alpha of 0.05.
In conclusion, the CFFMP, with hospitalization and rehabilitation in the community, enhanced functional recovery, prevented secondary fracture and reduced healthcare expenditure on hip fracture care for elderly patients. CFFMP not only enhanced patients’ functional performance, but also relieved the financial burden on society. With an escalating aged population, policymakers should review the current fragility fracture management protocol and consider implementing a multidisciplinary management programme.
This study was supported by Public Policy Research Grant Council, Hong Kong SAR Government (Ref: 4013-PPR-09).
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize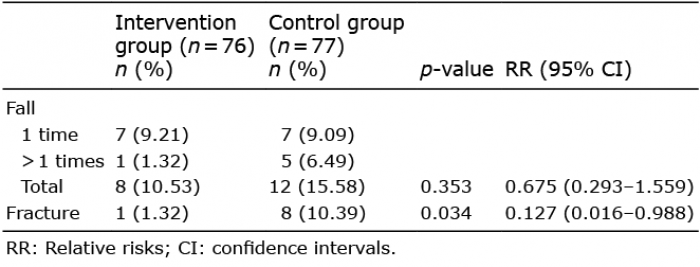 Click to show fullsize
Click to show fullsize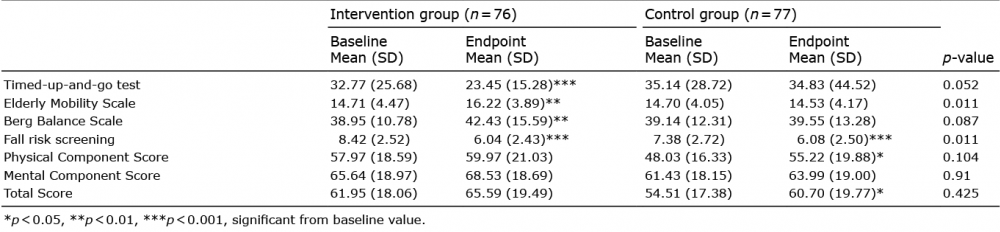 Click to show fullsize
Click to show fullsize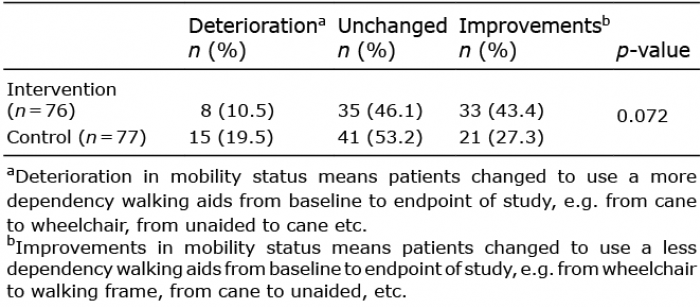 Click to show fullsize
Click to show fullsize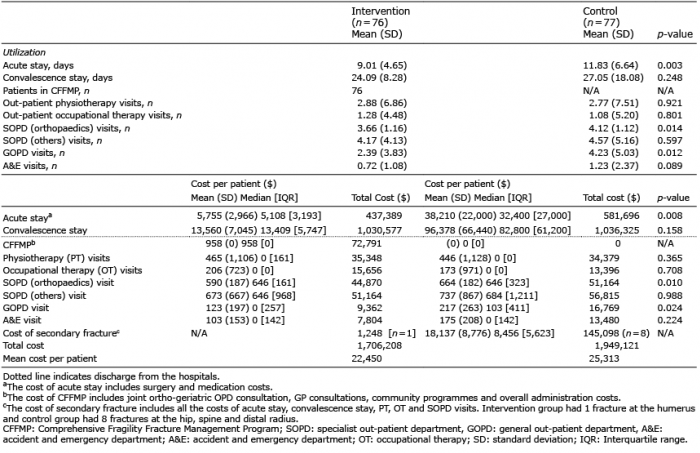 Click to show fullsize
Click to show fullsize