
From the 1Rehabilitation Department, Hôpital Joseph Ravoahangy Andrianavalona, Madagascar, 2Academic Department of Rehabilitation Medicine, School of Medicine, Faculty of Medicine and Health, University of Leeds, 3National Demonstration Centre in Rehabilitation, Leeds Teaching Hospitals NHS Trust, Leeds, and 4Princess Royal Spinal Cord Injury Unit, Northern General Hospital, Sheffield, UK
#These authors contributed equally and should be considered as first authors.
Rehabilitation for people with spinal cord injury in many low- and middle-income countries is not avail-able or is in the early stages of development. However, rehabilitation is recognized as crucial in order to optimize functional recovery and outcomes for patients with spinal cord injury. With an increasing incidence of spinal cord injury, the unmet need for rehabilitation is huge. This report describes the early development of a specialist rehabilitation service for spinal cord injury in Madagascar, one of the poorest countries in the world. The sustained input to an expanding rehabilitation team has led to reductions in avoidable complications. The input of the rehabilitation team has been welcomed by the neurosurgery department, which has recognized fewer delays in patients undergoing surgical treatments. Cost, lack of resources and trained staff, and poor understanding of disability continue to provide challenges. However, the development of the rehabilitation service using low technology, but with a high level of knowledge and systematic management, is a source of considerable pride. This development in Madagascar can be regarded as a model for spinal cord injury rehabilitation in other low-resource settings.
Key words: rehabilitation; spinal cord injuries; persons with disabilities; pressure ulcer.
Accepted Jan 4, 2018; Epub ahead of print Mar 27, 2018
J Rehabil Med 2018, 50: 00–00
Correspondence address: Rory J. O’Connor, Academic Department of Rehabilitation Medicine, D Floor, Martin Wing, Leeds General Infirmary, Leeds LS1 3EX, UK. E-mail: R.J.O’Connor@leeds.ac.uk
Rehabilitation is an integral part of recovery and reintegration to society following spinal cord injury (SCI) (1). In the UK, SCI services have grown from small beginnings during World War II to what is now a fully developed network of services (2). However, on an international scale, the availability of SCI rehabilitation remains uneven. In many developing countries, services are fledgling or absent. With an estimated global incidence rate of SCI of 250,000–500,000 per year, this reflects a huge unmet need for rehabilitation (3).
Madagascar is a large island nation with a population of 24 million, which, since independence in 1960, has experienced political and economic instability. It is ranked 158 out of 188 countries on the 2015 Human Development Index, with many people living in poverty (4). Despite this, the country has made significant strides towards improving access to healthcare and, in 2014, ratified the United Nations Convention on the Rights of Persons with Disabilities (UNCRPD) (5).
Between 2011 and 2013, staff from Leeds Teaching Hospitals, through the charity Opt In (Overseas Partnering and Training Initiative), began working with the Malagasy Ministry of Health and the University of Antananarivo to establish locally appropriate training leading to an examined mid-level Diplôme Universitaire (DU) in rehabilitation medicine (6). This programme resulted in 8 doctors passing the examination, who were then highly motivated to bring about change.
The 8 doctors went on to form a national association (Association de Médecine Physiques et de Réadaptation de Madagascar; AMPR Mada) and were instrumental in the development of the first ever SCI service in Madagascar, supported by rehabilitation staff from the UK. This article describes the development of this service.
Prior to 2011, rehabilitation facilities in Madagascar were poorly developed, with centres staffed only by physiotherapists and, in some cases, general practitioners seconded from primary care (6). There were no specialist services for SCI and there remain only 2 neurosurgical units to serve the whole country.
Early discussions centred on the perceived need for a SCI unit in the country’s capital, Antananarivo. It was decided that the Hôpital Joseph Ravoahangy Andrianavalona (HJRA) would be the focus for developing a centre of excellence, to serve as a hub for a network of regional and community-based services across Madagascar. This initiative had the backing of the neurosurgical team within HJRA, who welcomed the development and offered joint working.
Previously, the management of SCI in Madagascar involved only surgical fixation of fractured vertebrae for those who could afford it, with no rehabilitation or long-term follow up. The introduction of an integrated service, and thereby a patient pathway, now ensures all patients admitted with SCI are routinely reviewed by the rehabilitation team. The patient’s neurological status is assessed on admission according to the International Standards for Neurological Classification of Spinal Cord Injury, with patients then reviewed on a weekly basis (7, 8). Weekly case conferences provide a link with the neurosurgeons and guide inpatient management, whilst the rehabilitation team provide long-term follow up for patients discharged from hospital.
The neurosurgery ward in HJRA has 42 beds staffed by only 2 nurses at any time. Family members rather than nursing staff have to look after the physical needs of patients. The rehabilitation team provides education and support to the families to learn how to manage the patient correctly. Nursing staff are given specialist advice on preventing and treating pressure ulcers, managing bowels and bladder systematically, and practical measures to maintain stability of the spine.
Patients are routinely invited for 3-monthly follow up. The rehabilitation team have also initiated a community outreach programme, whereby members of the multidisciplinary team (MDT) travel into local communities once a week to make home visits to patients who are unable to attend hospital due to logistical or transportation issues.
In 2013, the rehabilitation team consisted of one doctor and one physiotherapist. The team was augmented by the addition of another doctor in 2014 and two nurses in 2015. To date, the country has no qualified occupational therapists to join the team.
Documentation began in June 2014 and continues to be hand-held by the director of the rehabilitation service (for the purposes of this report we have used the full-year data from 2015 and 2016 only). As this is an analysis of anonymized data collected for the purposes of patient care, the institutional review board deemed that ethical approval was not required.
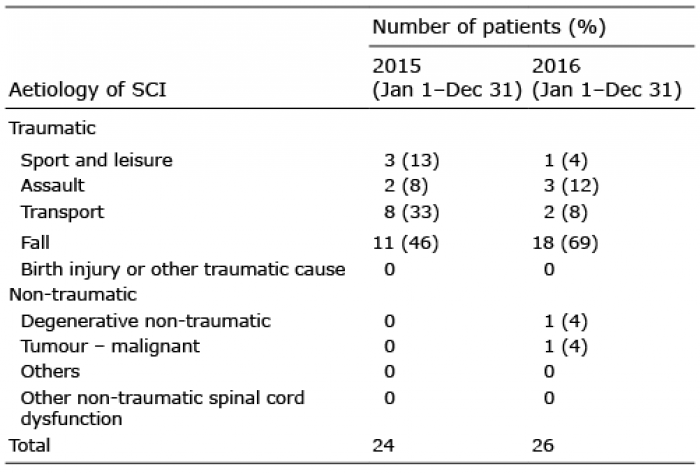
The SCI rehabilitation team at HJRA saw 24 patients in 2015 and 26 in 2016. There were a number of patients with SCI presenting to neurosurgery services who were not seen by the rehabilitation team, but exact figures are not available: patients who presented with a spinal column fracture and no neurological impairment were discharged directly home; those with severe injuries were transferred to intensive care in another unit, some of whom died; and some patients lacked the funds to support on-going medical care.
Most SCIs resulted from trauma; however, a small proportion was attributed to non-traumatic conditions (Table I).
Table I. Causes of spinal cord injury (SCI) per year (7, 8)
Most patients presented with paraplegia: 18 (75%) in 2015 and 23 (88%) in 2016. The rest presented with tetraplegia.
Delays to initial treatment of SCI are a common occurrence in Madagascar for logistic and financial reasons. In the past, these delays would frequently lead to secondary complications such as pressure ulcers, so that operative intervention became no longer possible.
Other secondary complications noted were gastrointestinal bleeding, constipation and neuropathic pain. The introduction of the rehabilitation service has led to improved awareness of preventative techniques, such as appropriate positioning to relieve pressure, and earlier recognition of complications. This is reflected in the reduction in the number of complications between 2015 and 2016, although there are no figures available for comparison prior to 2014. In practice the neurosurgeons have reported better outcomes due to less frequent complications enabling patients to undergo earlier surgical treatment.
Following a period of rehabilitation at HJRA, a small number of patients were referred to other regional rehabilitation centres to continue their treatment. A small proportion died during admission. However, many patients returned home successfully and some were able to return to work in jobs such as cooking or teaching. A number of patients were not contactable by telephone or post and were therefore lost to follow-up (Table II).
Table II. Discharge outcomes and follow-up at 3 months
The development of the first specialist service in Madagascar has been crucial in responding to a known need for SCI rehabilitation. The team has been guided by a UK-based physician with experience in low-income countries and the UK. His expertise has been paramount in facilitating major advances using low technology, but with specialist knowledge and systematic management.
Data from 2 years suggests that the service is beginning to have a positive impact. The rates of secondary complications are comparable with those in other reports from the region. A 2015 study in Ethiopia found 22.5% of patients with SCI developed pressure ulcers, compared with 11.5% in Madagascar in 2016 (9). A Nigerian study found that 45.9% of patients developed pressure ulcers; this higher percentage was attributed to resource constraints and dependence on untrained relatives to provide patient care, as was the case in Madagascar prior to 2014 (10). Rates for urinary tract infections (UTIs) were higher in Madagascar, at 50%, compared with 13.5% in the Ethiopian study (9). How-ever, the decrease in UTIs over the last 2 years suggests an improvement in parallel with on-going training.
There are relatively few patients with tetraplegia seen in the unit in HJRA. Many patients with severe injuries are unable to attend hospital; difficulties with transportation or the inaccessible costs of treatment are major barriers. Where there are multiple co-existing injuries, many patients will not survive to reach hospital, due to the poor availability of pre-hospital care. There is likely to be a higher incidence of SCI overall, particularly given the frequency of road traffic accidents. However, the figures seen here reflect only those admitted under neurosurgery.
Cost. As in many low-income countries, much of the Malagasy health budget is used for World Health Organization (WHO) priority areas, such as maternal health. The development of the SCI service has therefore only been possible through continued external charitable funding. It is hoped that the WHO’s “Rehabilitation 2030: a call for action” and WHO/ International Spinal Cord Society (ISCOS)’s “International perspectives on spinal cord injury”, with their emphasis on the value of multidisciplinary rehabilitation, will result in its accessing more funding (3, 11).
An estimated 78% of Madagascar’s population live on less than US$1.90/day (12). Although there is no formal cost-analysis of SCI management in Madagascar, a study by Kawu et al. estimated the mean cost of the acute phase of SCI care in Nigeria at US$1,598 (13). As there is no universal health coverage in the country, and health insurance is uncommon, few families can afford the acute treatment and subsequent rehabilitation.
Access to healthcare. Poor road and transportation infrastructure in Madagascar has a significant impact on transfer to and from healthcare facilities. In addition, there are few facilities that are accessible to people with disabilities (8). These factors may also account for the large number of patients lost to follow up. However, this is now being addressed through the community outreach programme.
Staffing and resources. Prior to 2011, Madagascar lacked specialist training for rehabilitation physicians. However, between 2011 and 2013 a postgraduate training programme was established, with input from UK-based rehabilitation professionals, resulting in 8 doctors gaining the mid-level Diplôme Universitaire (6).
Further teaching has been ongoing, with regular input from the UK. As part of their continuing professional development, the Malagasy team were supported to present at international conferences, principally the first African Spinal Cord Injury Network (AFSCIN) meeting (Botswana, 2015) and the Southern African Spinal Cord Association conference (South Africa, 2016). Madagascar is now an active member of the newly-formed AFSCIN (14).
The unit in HJRA would benefit from additional trained nursing staff and healthcare assistants. Although there are currently no occupational therapists in the service, the first cohort of trainees will graduate in 2017. Currently, HJRA has no dedicated rehabilitation beds and the neurosurgery ward are unable to keep patients long enough to complete their rehabilitation.
Stigma. In a country where access to education is limited, there remains a stigma attached to disability. Lack of awareness compounds the problem, pointing to the need for education and strong patient organizations prepared to perform advocacy work.
To date, there are limited data on SCI in Madagascar. Although there is a recognized need for computerized data collection, there have nevertheless been handwritten records from 2015 onwards. The limited dataset from the last 2 years may have affected case ascertainment for this quantitative analysis. However, qualitative feedback has been extremely encouraging.
SCI services in Madagascar are continuing to develop, with an emphasis on clinical knowledge and systematic management rather than advanced technology. These developments are a source of considerable pride. However, poor transport infrastructure and the low level of healthcare funding will continue to frustrate development. Other countries now acknowledge the positive advancements in Madagascar, which is leading the way for rehabilitation services across Africa (15). Future evaluations will be beneficial to establish the role and impact of the expanding service.
The authors would like to acknowledge the support of Opt In and SPIRIT, who funded much of the rehabilitation teaching programme. They would also like to thank Dr Sonia Andrianabela at the Malagasy Ministry of Health and Professor Luc Samison, Dean of the Faculty of Medicine at the University of Antananarivo, for their support in the development of the training programme, and the neurosurgeons at HJRA for their encouragement and collaboration.


 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize