
From the 1Department of Kinesiology, University of Illinois at Chicago, Chicago, IL, and 2Department of Rehabilitation Medicine, University of Washington, Seattle, WA, USA
Objective: Challenging clinical balance tests are needed to expose balance deficits in lower-limb prost-hesis users. This study examined whether narrowing beam-walking could overcome conceptual and practical limitations identified in fixed-width beam-walking.
Design: Cross-sectional.
Participants: Unilateral lower-limb prosthesis users.
Methods: Participants walked 10 times along a low, narrowing beam. Performance was quantified using the normalized distance walked. Heuristic rules were applied to determine whether the narrowing beam task was “too easy,” “too hard,” or “appropriately challenging” for each participant. Linear regression and Bland-Altman plots were used to determine whether combinations of the first 5 trials could predict participants’ stable beam-walking performance.
Results: Forty unilateral lower-limb prosthesis users participated. Narrowing beam-walking was appropriately challenging for 98% of participants. Performance stabilized for 93% of participants within 5 trials, while 62% were stable across all trials. The mean of trials 3–5 accurately predicted stable performance.
Conclusion: A clinical narrowing beam-walking test is likely to challenge a range of lower-limb prosthesis users, have minimal administrative burden, and exhibit no floor or ceiling effects. Narrowing beam-walking is therefore a clinically viable method to evaluate lower-limb prosthesis users’ balance ability, but requires psychometric testing before it is used to assess fall risk.
Key words: postural balance; accidental falls; amputee; patient outcomes assessment; rehabilitation; mobility limitation; walking.
Accepted Jan 31, 2018, Epub ahead of print Apr 4, 2018
J Rehabil Med 2018; 50: 00–00
Correspondence address: Andrew B. Sawers, Department of Kinesiology, University of Illinois at Chicago, 1919 W. Taylor Street, 646 AHSB (MC 517), Chicago, IL 60612, USA. E-mail: asawers@uic.edu
Clinical balance tests are often designed for people with significant balance impairments and may be too easy for people with moderate impairments, such as lower-limb amputation (1). As such, balance tests often exhibit ceiling effects (1) or fail to discriminate between lower-limb prosthesis (LLP) users with and without a history of falls (1, 2). Tests that pose greater challenge to balance control are needed to expose important balance deficits and identify users at risk of falls (3, 4).
Beam-walking increases the challenge to balance control (3, 5) by constraining step width and/or reducing the support surface, increasing the control required over the centre-of-mass. Beam-walking has been used previously to discern differences in balance between controls and LLP users (3), older adults (5), children (6) and professional ballet dancers (3). Beam-walking is thus an appealing paradigm for clinical testing because various levels of challenge can be created (i.e. different beam widths create unique walking conditions) and performance can easily be evaluated (i.e. an individual is either on or off the beam). Despite these benefits, the clinical feasibility of beam-walking as a means to assess balance control and/or fall risk within different clinical populations remains largely unexplored.
An initial study of LLP users found that walking on fixed-width beams had limited clinical feasibility. Similar to a study of older adults (5), no single fixed-width beam provided an appropriate challenge to the LLP users studied (7). At least one-third of participants found walking along each of 3 fixed-width beams either too easy (i.e. they regularly finished the task) or too difficult (i.e. they could not consistently start the task). A clinical test derived from a fixed-width beam would therefore probably exhibit ceiling and floor effects. While the use of multiple beams could address this limitation, it would also impose undue administrative burden on clinicians by way of equipment, set-up, and administration time (7). A narrowing beam, consisting of segments from fixed-width beams, was proposed as a way to create a single test condition that could be used with individuals across the spectrum of balance ability. A narrowing beam test would theoretically combine the best attributes of single and multiple fixed-width beam-walking tests (i.e. minimal administrative burden and limited ceiling and floor effects).
The objective of this study was to determine whether narrowing beam-walking could address limitations of fixed-width beam-walking for assessing balance in LLP users (7). We predicted that: (i) a narrowing beam-walking task would challenge a broad range of ambulatory LLP users, such that a subsequent clinical test would be free from ceiling or floor effects; (ii) narrowing beam-walking performance would stabilize for LLP users within fewer trials than fixed-width beam-walking; and (iii) a narrowing beam-walking test procedure that limits administrative burden (i.e. number of trials) would accurately predict and have a high level of agreement with LLP users’ stable performance.
A cross-sectional study was conducted between July 2016 and May 2017 to assess LLP users’ ability to walk on a novel narrowing beam. All study protocols were reviewed and approved by the University of Illinois at Chicago Institutional Review Board. All individuals provided written informed consent prior to enrollment and participation.
Participants were recruited from local prosthetic clinics. Inclusion criteria were: 18 years of age or greater; unilateral, transtibial or transfemoral amputation; at least 1 year of experience using a prosthesis; and able to walk 3.05 m over level terrain without an assistive device other than a prosthesis (e.g. cane). Individuals were excluded if they had amputation of another limb; contralateral leg complications such as a knee replacement, ulcers, or infections; an advanced neurological disorder; or severe heart or pulmonary disease.
Demographic characteristics, including age and sex, were collected by self-report, while the investigators measured height and mass. Health-related information was collected via interview and included amputation level and aetiology, time since amputation, current prosthetic prescription, and time with current prosthesis. Medicare Functional Classification Level (K-Level) (8) was established through clinical inspection and interview. The Prosthetic Limb Users Survey of Mobility (PLUS-M) 12-item short form was used to measure participants’ perceived mobility (9).
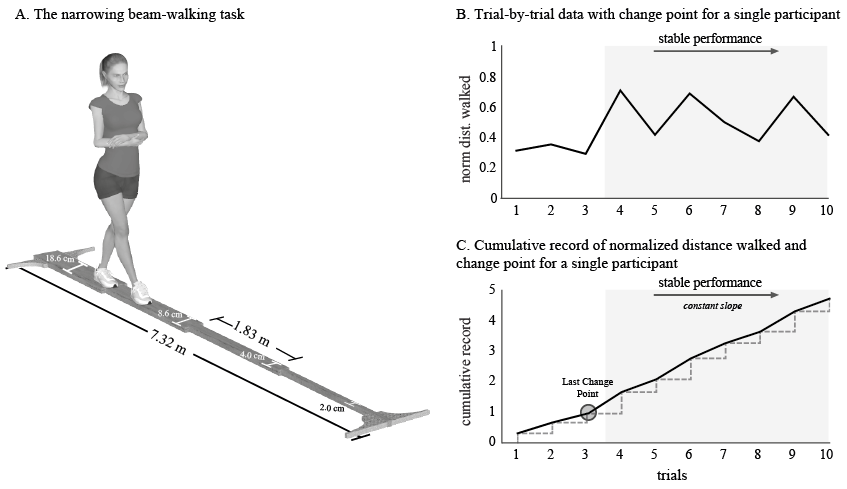
A narrowing beam measuring 7.32 m in length was constructed from 4 fixed-width beam segments each 1.83 m in length (Fig. 1A). A low beam height (3.8 cm) was selected to minimize postural threat (10). Beam segments varied in width (wide = 18.6 cm, intermediate = 8.6 cm, narrow = 4.0 cm, and very narrow = 2.0 cm) to create increasingly challenging walking conditions. Beam dimensions were selected based on earlier research (3, 5, 11, 12), which showed these or similar widths collectively challenged individuals with a range of balance abilities. Marks were placed every 15.24 cm along the length of the beam to measure the distance walked.
Fig. 1. (A) Narrowing beam-walking task. Participants attempted 10 walking trials. Gait pattern was not constrained, but participants kept their arms crossed over their trunk. If participants stepped off the beam or uncrossed their arms, the trial was stopped and the distance walked to that point was recorded. (B) Period of stable performance for a representative participant (grey band). (C) Periods of stable performance were identified based on change points in the slope of the cumulative record of each participant’s normalized distance. For this participant, the last change point occurred during trial 3 (i.e. significant difference in slope before and after that trial).
Each participant attempted to walk the length of the narrowing beam 10 times in order to provide an opportunity to achieve a stable level of performance. Participants were instructed to keep their arms crossed to mitigate potential trial-to-trial or individual differences in arm compensation strategies. No instructions regarding step length were provided, as enforced step length has been shown to have little effect on beam-walking performance (5). Each trial was concluded when the participant uncrossed their arms, stepped off the beam, or walked its full length; whichever came first. The distance of the most anterior position of the last foot on the beam was recorded when the participant uncrossed their arms or stepped off the beam before completing the trial.
Beam-walking performance was quantified by the “normalized distance”, or the mean distance walked across each trial relative to overall beam length (3). To account for participants’ starting position (i.e. with one foot on the beam) relative beam length was the final 6.71 m of the beam (7.32–0.61 m). Therefore, normalized distance was calculated relative to the last 6.71 m of the beam. For example, if the participant did not reach the 0.61 m mark on a trial, normalized distance was 0.0. If the participant successfully walked the length of the beam normalized distance was 1.0. Normalized distance was calculated as 0.36 if the participant stepped off the beam at the 3.05-m mark (i.e. 2.44 m/6.71 m).
To determine if and when each participant’s beam-walking performance stabilized (i.e. reached a consistent level), a recursive algorithm was applied to detect significant changes in the slope of each participant’s cumulative trial-by-trial record (14). These changes in slope are referred to as change points. The last change point in a record indicates when a participant’s cumulative trial-by-trial record reaches a terminal slope, and thus when beam-walking performance stabilizes (Fig. 1B, C). For example, a participant’s beam-walking performance would be considered stable from trials 4 to 10 if the last change point occurred at trial 3. Performance would be considered stable across all trials if no change points were identified in a data record. Conversely, performance would not be considered to have stabilized if a participant’s last change point occurred at trial 9. Change point analysis was performed using previously developed Matlab™ (Mathworks, Natick, MA, USA) routines (14).
Several test administration procedures were proposed and evaluated to determine whether participants’ mean normalized distance during the stable period of narrowing beam-walking could be estimated accurately in 5 or fewer trials. Only the first 5 trials were considered since the objective was to develop a clinical test with minimal administrative burden. Mean normalized distance during the stable period was selected as the reference because it was deemed to reflect an individual’s “usual” or “typical” balance ability.
Combinations of participants’ mean and maximum normalized distances during the first 5 trials (e.g. maximum of first 3 trials, mean of trials 3–5) were systematically assessed to determine which potential test administration procedure best estimated participants’ mean, stable performance on the narrowing beam. Simple linear regressions were performed using mean normalized distance during the stable performance period as the dependent variable and normalized distances from the potential test administration procedures as the independent variables. Bland-Altman plots (15) were also constructed to assess the level of agreement between the independent and dependent variables. To test for proportional bias in each potential test procedure, regression coefficients (β) for each of the Bland-Altman plots were calculated and compared with zero. Shapiro-Wilk’s test was used to assess all data for normality. All statistical tests were conducted using SPSS (V.24; SPSS, Inc., Chicago, IL, USA).
Forty LLP users participated in the study (Table I). Normalized distance on the narrowing beam (mean = 0.41, 95% confidence interval (95% CI) 0.06 across all participants) was normally distributed.
Table I. Participant demographics
Out of the 40 participants 39 were consistently able to start, but rarely finish walking along the narrowing beam. Only one participant demonstrated 3 or more trials with a normalized distance of 0.0 (i.e. too hard), and none registered 3 or more trials with a normalized distance of 1.0 (i.e. too easy) (Fig. 2A). In general, each participant’s performance on the narrowing beam mirrored individual LLP user’s performance on the most suitable of 3 fixed-width beams tested in a previous study (Fig. 2B) (7).
Fig. 2. Narrowing beam-walking provided a suitable level of challenge for assessing balance across a broad sample of ambulatory LLP users. (A) Thirty-nine of 40 participants were regularly able to start, but not complete, the task. (B) Performance on the narrowing beam mirrored performance on the most suitable of 3 fixed-width beams tested previously (7). LLP users in the present study showed similar performance on the narrowing beam as on wide, intermediate, or narrow fixed-width beams deemed to be appropriately challenging for them in a prior study. This implies that a single test condition, the narrowing beam, can replace 3 test conditions (i.e. wide, intermediate and narrow beams) and subsequently reduce administrative burden.
Six trials were required to account for all 40 participants last change points on the narrowing beam (Fig. 3). However, 37 of the 40 participants’ last change points were identified by the fifth trial, and 25 of the 40 participants had no change points in their performance record (i.e. they exhibited stable performance from the first trial onward).
Fig. 3. Narrowing beam-walking performance stabilized for each participant. Overall, 7 trials were required to account for the last change point of each participant. However, 37 of 40 participants’ last change points occurred by the fifth trial, and 25 of 40 had stable performance from the first trial onward.
Assumptions of linearity, independence of observation, normality, and homoscedasticity for simple linear regression were confirmed. Stable beam-walking performance (mean ± 95% CI normalized distance) was 0.41 ± 0.06. Linear regression demonstrated that normalized distances derived from all potential test administration procedures statistically predicted participants’ mean normalized distance during the stable period of performance, F(1,38) = 88.24–242.30, p < 0.005. Normalized distances obtained using the potential test procedures accounted for 70–91% of the variation in mean stable normalized distances with adjusted R2 = 0.69–0.90. The standard error of the estimate varied between 0.067 and 0.106 for each of the potential test procedures (Table II). Normalized distances, based on means of trials 2 through 4, trials 2 through 5, and trials 3 through 5, provided the most accurate estimates of stable performance, and were selected for further analysis.
Table II. Variance in observed score accounted for (R2) and standard error of the estimate (SEE) by potential administration procedures
Among these 3 proposed test administration procedures, there was an equal distribution of data-points above and below the mean difference line on the Bland-Altman plots (Fig. 4). Regression coefficients (β) for each of the Bland-Altman plots were not significantly different from zero (mean of: trials 2 through 4 β = 0.052, p = 0.444; trials 2 through 5 β = –0.020, p = 0.749; trials 3 through 5 β = –0.021, p = 0.760). None of the participants’ estimated normalized distances were outside the 95% limits of agreement (i.e. ± 1.96 standard deviation of mean difference) for the mean of trials 3 through 5. In contrast, 2 (5%) and 4 (10%) of the normalized distances were outside the 95% limits of agreement for the mean of trials 2 through 5 and trials 2 through 4, respectively.
Fig. 4. Bland-Altman plots for the top 3 test procedures. (A) Mean of trials 3 through 5. (B) Mean of trials 2 through 5. (C) Mean of trials 2 through 4. The solid line depicts the mean difference between the observed (i.e. stable) performance and the performance estimated using each of the proposed test procedures. The dashed lines depict the 95% confidence interval (95% CI) or limits of agreement of those mean differences. The equal distribution of points above and below the mean difference line suggests that there is no proportional bias between the full and abbreviated test procedures. 100% of the data points were within the 95% CI limits for the mean of trials 3 through 5, 95% for the mean of trials 2 through 5, and 90% for the mean of trials 2 through 4. Results indicate that the mean of trials 3 through 5 provides the most accurate estimate of participants’ stable performance.
Narrowing beam-walking presents as a clinically feasible approach for evaluating balance ability across a range of ambulatory LLP users. This conclusion is based on results from the present study that showed: (i) participants routinely started, but did not finish, the narrowing beam-walking task; (ii) participants’ performance on the narrowing beam stabilized rapidly; and (iii) a narrowing beam-walking test procedure accurately predicted participants’ stable narrowing beam-walking performance.
Based on previously developed heuristic rules to assess beam-walking performance (7), only one of the 40 participants found the narrowing beam-walking task too hard. None found it too easy. Adopting the conservative 15% threshold noted by Andresen (13), these results imply that a clinical test based on a narrowing beam-walking task would exhibit neither ceiling nor floor effects among ambulatory LLP users. In contrast, fixed-width beam and narrow-path walking tasks would probably require multiple beams or path widths to avoid ceiling and floor effects (4, 5, 7, 16). Eliminating or reducing ceiling effects relative to other types of beam-walking tests may confer additional benefits. Potential benefits include an improved ability to measure balance across a broader range of individuals, identify improvements and deteriorations in balance performance more consistently, and discriminate between fallers and non-fallers with greater sensitivity and specificity. Therefore, the narrowing beam-walking task proposed here appears to achieve a key objective towards improved clinical assessment, to mitigate ceiling effects common to clinical balance tests by increasing the challenge to balance control (1, 17). Although the present study targets LLP users, ceiling effects have been reported in clinical tests used to assess balance in other clinical populations (e.g. incomplete spinal cord injury, concussion, older adults) (2, 18–21). Therefore, the narrowing beam-walking task presented here may also enhance clinicians’ abilities to accurately assess balance in other populations at risk for falls.
Narrowing beam-walking performance stabilized for all participants within 6 trials, 37 of 40 participants within 5 trials, and 25 of 40 participants within a single trial. Overall, narrowing beam-walking performance stabilized in 2 fewer trials than fixed-width beam-walking (7). These results suggest narrowing beam-walking has reduced learning effects relative to fixed-width beam-walking. This is consistent with previous studies that showed participants’ performance on a progressively narrowing path remained stable (22) while participants’ performance on a fixed-width narrow path improved trial-to-trial (16, 23). This implies that tests with offering progressively increasing challenge to balance (e.g. a narrowing beam or path) may be able to measure an individual’s typical performance more efficiently (i.e. with fewer trials) than tests with a consistent level of challenge. It may be that progressively changing task-demands are less susceptible to learning and facilitate the measurement of underlying ability rather than practiced skill. While our finding that 25 of 40 participants demonstrated no learning effect at all supports this hypothesis, but further testing is needed to confirm it. Although the focus of this study was on balance, results may also inform development and administration of more challenging tasks to assess other constructs, such as mobility (24, 25).
Measuring the time course of performance stabilization, as was done in this study, confers 3 benefits that are rarely considered in the development of clinical balance tests. First, identifying the period of stable performance ensures that the construct of interest (i.e. balance) is evaluated during consistent, rather than changing performance levels (e.g. during a period of learning). Efforts to assess the number of trials required to achieve stable performance in clinical balance tests are rare. Studies that have evaluated participants over sequential trials often reveal that the few trials generally recommended in clinical test administration protocols (e.g. 3 or less) are insufficient for performance to stabilize (26, 27). Therefore, most clinical assessments are made when individuals are improving on a test, rather than performing at a consistent level indicative of their inherent ability. Secondly, examining performance stabilization allows developers of performance-based tests to determine whether a proposed administration or scoring procedure measures an individual’s typical or atypical (e.g. best or optimal) performance. This may be particularly important with balance tests, as measuring an individual’s best performance over a small number of trials may overestimate their ability and underestimate the presence of deficits that contribute to fall risk. Notably, developers often recommend scoring a test using the best trial (28, 29) even when consecutive trials in performance-based tests are shown to vary (26, 27, 30). Thus, it remains unclear to what extent an individual’s best performance on a clinical test is representative of his or her true ability. Importantly, none of the test administration procedures examined in this study that used “maximum” normalized distances provided better estimates of participants’ stable performance than the test administration procedures that used “mean” distances. This suggests that LLP users’ best performance may not provide the most accurate estimate of their true ability on this test. Lastly, quantifying the time course of performance stabilization provides a basis for developing an accurate and yet pragmatic administration and scoring procedure. By identifying the point at which performance stabilized, it was possible to develop a shorter, yet still accurate, test procedure for the narrowing beam-walking test.
Several different methods for scoring the narrowing beam-walking test were evaluated in this study. Among the top 3 viable methods, Bland-Altman plots revealed an absence of proportional bias and an acceptable level of agreement between participants’ estimated and observed (i.e. stable) performance. Thus, any of these test procedures could be used in place of the full 10 trials. While each of these test procedures predicted participants’ stable performance, the mean of trials 3 through 5 was the most accurate. Considering its prediction accuracy, level of agreement, and absence of bias, the mean of trials 3 through 5 provides the best estimate of observed stable narrowing beam-walking performance among ambulatory LLP users. Adopting this test procedure reduces the number of trials to be collected, since there is no longer a need to determine each individual’s period of stable performance post-hoc. Thus, administrative burden of the proposed narrowing beam-walking test (Appendix SI1) would be similar to that of existing single-task balance tests, such as the Timed Up and Go (3–6 trials) (26, 31), Four Square Step Test (3 trials) (28), and the Single Leg Stance Test (5 trials) (32) and less than multiple-task tests such as the Berg Balance Scale (33), Dynamic Gait Index (34) or Fullerton Advanced Balance scale (35).
While the results of this study are promising, it is plausible that the current narrowing beam design may be susceptible to floor effects among LLP users with significant mobility restrictions (i.e. unable to walk 3.05 m). This potential limitation could be addressed by adding a wider beam segment at the start of the test (22). In addition, the scoring procedures proposed here (i.e. mean of trials 3 through 5) only provide an estimate of stable observed performance, and may not predict stable performance for every individual. However, our data suggest that this procedure produces an accurate estimation for most ambulatory LLP users and is a practical method to limit overall administrative burden. Since this study was cross-sectional in nature, we assessed only short-term (i.e. within-session) learning effects. Longitudinal studies are required to determine whether beam-walking performance is consistent over sessions conducted on different days (i.e. test-retest reliability). Finally, these results do not imply that a narrowing beam-walking task can be used to evaluate fall risk. Additional validation of the proposed narrowing beam test is needed to evaluate its diagnostic accuracy.
This study is the first step towards the development, psychometric evaluation, and implementation of a standardized narrowing beam-walking test for measuring balance in LLP users. Here we demonstrated that: (i) most participants in this study routinely started, but did not finish, the narrowing beam-walking task, suggesting that a clinical test based on these results is likely to be free of ceiling and floor effects; (ii) walking performance on the narrowing beam stabilized rapidly, facilitating the development of test administration procedures to estimate participants’ stable performance; and (iii) a narrowing beam-walking test, scored as the mean of trials 3 through 5, accurately predicted participants’ stable narrowing beam-walking performance, suggesting a clinical test based on this procedure would have minimal administrative burden. Based on these findings, we propose that the narrowing beam-walking test next be evaluated for validity relative to existing clinical tests, reliability over time, and accuracy for assessing fall risk among LLP users.
The authors wish to acknowledge David Kruse for his assistance with data collection and data entry, as well as David Rotter, CPO, for his assistance with recruitment.
Funding/support: This work was supported through funds from the Orthotics and Prosthetics Education and Research Foundation, Inc. (OPERF) under grant number OPERF-SGA-2016-1, and by the National Institutes of Health (NIH) under Award Number K12HD073945.
Disclaimer: Opinions, interpretations, conclusions and recommendations are those of the authors and are not necessarily endorsed by OPERF or the NIH. The authors declare no financial conflicts of interest.


 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize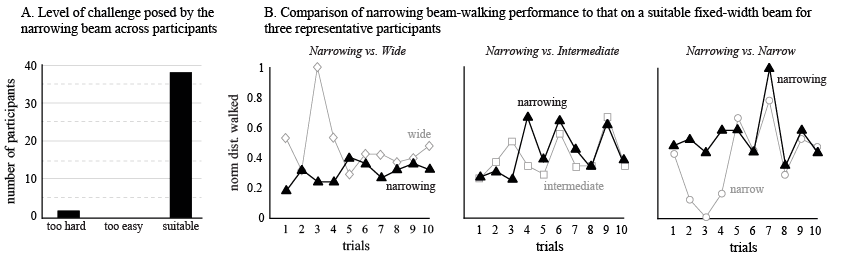 Click to show fullsize
Click to show fullsize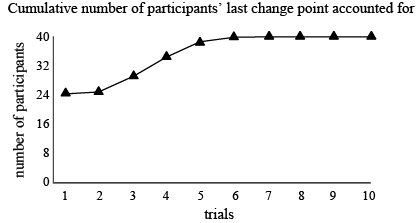 Click to show fullsize
Click to show fullsize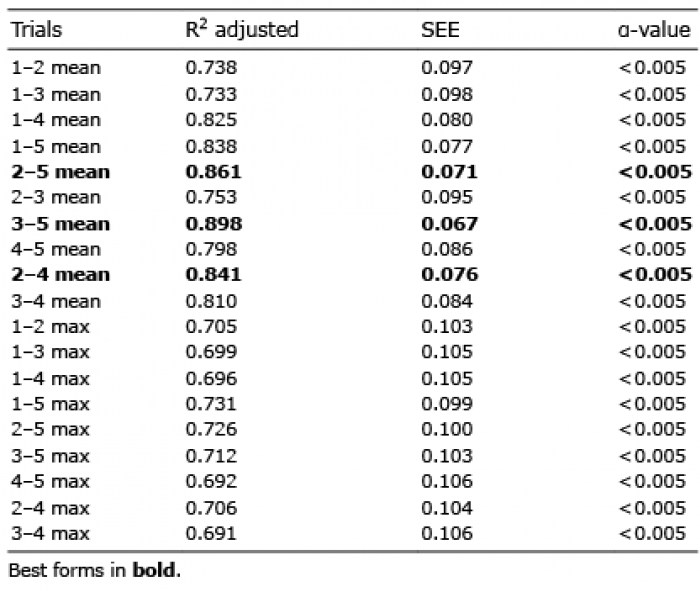 Click to show fullsize
Click to show fullsize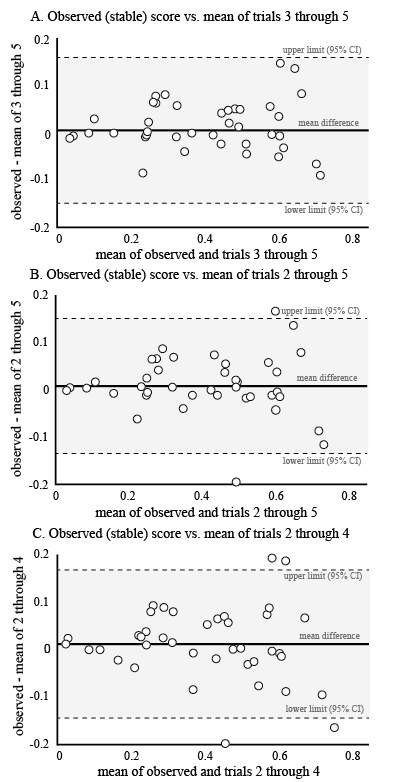 Click to show fullsize
Click to show fullsize