
From the 1Department of Physical Medicine and Rehabilitation, Zekai Tahir Burak Training and Research Hospital, 2Keçiören Training and Research Hospital and 3Gazi University Faculty of Medicine, Ankara, Turkey
Objective: To investigate the efficacy of Nintendo Wii Fit®-based balance rehabilitation as an adjunc-tive therapy to conventional rehabilitation in stroke patients.
Methods: During the study period, 70 stroke patients were evaluated. Of these, 23 who met the study criteria were randomly assigned to either the experimental group (n = 12) or the control group (n = 11) by block randomization. Primary outcome measures were Berg Balance Scale, Functional Reach Test, Postural Assessment Scale for Stroke Patients, Timed Up and Go Test and Static Balance Index. Secondary outcome measures were postural sway, as assessed with Emed-X, Functional Independence Measure Transfer and Ambulation Scores. An evaluator who was blinded to the groups made assessments immediately before (baseline), immediately after (post-treatment), and 4 weeks after completion of the study (follow-up).
Results: Group-time interaction was significant in the Berg Balance Scale, Functional Reach Test, anteroposterior and mediolateral centre of pressure displacement with eyes open, anteroposterior centre of pressure displacement with eyes closed, centre of pressure displacement during weight shifting to affected side, to unaffected side and total centre of pressure displacement during weight shifting. Demonstrating significant group-time interaction in those parameters suggests that, while both groups exhibited significant improvement, the experimental group showed greater improvement than the control group.
Conclusion: Virtual reality exercises with the Nintendo Wii system could represent a useful adjunctive therapy to traditional treatment to improve static and dynamic balance in stroke patients.
Key words: postural balance; virtual reality; stroke; rehabilitation.
Accepted Feb 23, 2018; Epub ahead of print Apr 5, 2018
J Rehabil Med 2018; 50: 00–00
Correspondence address: Elif Balevi Batur, Department of Physical Medicine and Rehabilitation, Keçiören Training and Research Hospital, 29sk, 52/8 Emek, Çankaya, TR-06490 Ankara, Turkey. E-mail: elifbalevi@hotmail.com
1The results of this study have been presented as poster at the 7th World Congress of NeuroRehabilitation Congress (WCNR-2012), Melbourne, Australia.
Stroke is one of the leading causes of disability (1). In stroke patients, balance can be affected by various factors, such as muscular weakness, abnormal muscle tone, deficits in visual and sensory function or disturbances in vestibular mechanisms (2). Since balance dysfunction is associated with increased risk of falling, balance exercises are a critical component of the rehabilitation of stroke patients.
Recent years have seen growing interest in the use of new technologies, such as virtual reality (VR), in stroke rehabilitation. Clinical results indicate that the use of VR technologies improves motor functioning (3–5). VR can be used to improve upper limb function, gait and balance, global motor function and cognitive function in stroke patients (6). However, VR equipment is usually complex and expensive, and may be available only in specialist centres with the help of experienced therapists. As a consequence, there has been an increase in the number of studies on the efficacy of commercial gaming programs in stroke rehabilitation. PlayStation, Wii, and Xbox, along with Kinect, are the game consoles most commonly used in stroke rehabilitation. Wii (Nintendo, Kyoto, Japan) is a game console used to improve balance, strength, flexibility and fitness. It provides a relatively simple and inexpensive opportunity for VR treatment (7).
Several randomized controlled studies have evaluated the effect of Wii-based balance rehabilitation programmes in stroke patients. Cho et al. (8) investigated the effects of VR balance training using Wii in chronic stroke patients. They reported that Wii-based VR exercises resulted in a significant improvement in dynamic balance (8). In another study, chronic stroke patients were randomly assigned to 2 groups. In the first group patients played console games for 5 weeks, and in the control group patients maintained their usual daily activities. A slight improvement was measured in the first group (9).
There are conflicting results in the literature about the efficacy of Wii-based balance exercises compared with other balance rehabilitation programmes, such as progressive balance training and task-specific programmes.
A number of studies have investigated whether the addition of Wii exercises or other exercise options to balance rehabilitation programmes makes a difference in stroke patients. The results are controversial. Lee et al. (10) reported better results in the Wii group. In contrast, Yatar et al. (11) indicated that there were no differences between Wii Fit balance training and progressive balance exercises.
Adequate postural control and good balance performance are prerequisites for independence in daily activities; therefore, these should be important goals of stroke rehabilitation (8). The aim of this study was to investigate the efficacy of Wii Fit-based balance rehabilitation as an adjunctive therapy to conventional rehabilitation in stroke patients.
The study was conducted in accordance with the World Medical Association Declaration of Helsinki and the Guideline for Good Clinical Practice. The study protocol was approved by the local ethics committee and all the participants provided written informed consent.
Stroke patients who were treated in Gazi University Faculty of Medicine, Department of Physical Medicine and Rehabilitation between October 2009 and August 2011 were included in the study. Stroke was diagnosed according to World Health Organization (WHO) criteria and cerebral lesions were verified by computerized tomography (CT) or magnetic resonance imaging (MRI) scans (12).
The inclusion criteria were: having had a first episode of unilateral stroke during the previous 12 months; being able to understand and follow simple verbal commands and participate in a rehabilitation programme for the first time.
Exclusion criteria were: the presence of cognitive disorders, sensory or global aphasia; a history of systemic disease or medication that causes peripheral neuropathy; having a lower extremity motor improvement level of Stage 1 on the Brunnstrom scale; the presence of cerebellar lesions or anomalies in cerebellar tests; deep sensory impairment; visual impairment; vestibular impairment; lack of cooperation in performing the balance exercises and tests; or orthopaedic disorders that prevent execution of the balance tests.
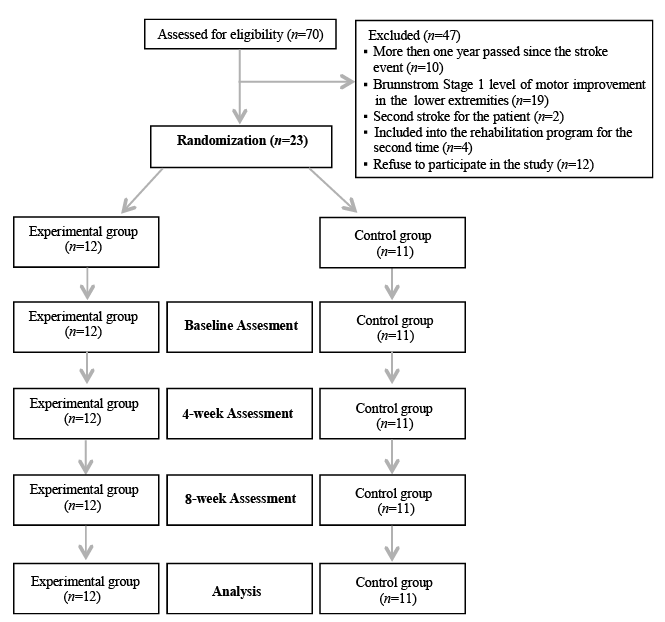
Seventy stroke patients were treated in our clinic during the study period. Of these 47 patients who did not meet the study criteria were excluded (Fig. 1). Twenty-three patients (10 men and 13 women) were randomly assigned to either the experimental group (n = 12) or the control group (n = 11) by block randomization. A randomization table was used to determine randomization numbers. The cards showing to which group each patient would be allocated were placed in a series of numbered, sealed, opaque envelopes. Both the experimental and the control groups participated in conventional balance rehabilitation exercises. These exercises formed part of the conventional neurological rehabilitation programme, and were performed for 2–3 h a day, 5 days a week. Conventional rehabilitation also included a programme of neurodevelopmental facilitation techniques, physiotherapy, occupational therapy, and cognitive therapy, all of which were tailored to the patients’ requirements. The experimental group received 20 min of balance exercise, 5 days a week, for 4 consecutive weeks, with Wii Fit and Wii Balance Board, in addition to conventional rehabilitation. The Wii Balance Board is a small (51.1 cm wide, 31.6 cm long, 5.3 cm high), lightweight (3.5 kg without batteries) system with a total of 4 force sensors, one in each corner, with which it measures the weight and pressure centre of its users. The Wii Balance Board can sense the transfer of weight in different directions. By reflecting this information precisely onto a television screen using an avatar, it allows the individual to observe his or her own movements, and provides positive feedback. The balance games included in the Wii Fit package were used during the exercises. As these games were developed for healthy individuals, 6 of the 9 balance games were selected, which the hemiplegic patients included in the study would be able to play, namely Heading, Ski Slalom, Table Tilt, Tightrope Tension, Balance Bubble and Penguin Slide.
Fig. 1. Study flow diagram.
Patients’ demographic data, time since stroke, date of admission, type of stroke, and radiological findings (MRI and CT) were recorded.
Primary outcome measures were the Berg Balance Scale (BBS), Functional Reach Test (FRT), Postural Assessment Scale for Stroke Patients (PASS), Timed Up and Go Test (TUG), and Static Balance Index (SBI) measured by Kinesthetic Ability Trainer (KAT) 3000 (Med-Fit Systems Inc., Fallbrook, CA, USA) (13–18). Secondary outcome measures were postural sway, as assessed with Emed-X (Novel GmbH, Munich, Germany), and Functional Independence Measure transfer (FIMt) (FIMt; 3 items: Bed, chair, wheelchair; Toilet; Tub/shower) and locomotion (FIMl; 2 items: Walk/wheelchair; Stairs) scores. An evaluator who was blinded to the groups made assessments immediately before (baseline), immediately after (post-treatment), and 4 weeks after completion of the study (follow up) (Fig. 1).
KAT-3000 is a balance platform designed for training and testing of static and dynamic balance. The Static Balance Index (SBI) quantifies the ability to keep the platform near the reference position. For the static balance test, a low SBI value reflects low postural sway during quiet standing and is interpreted as “good” balance (19). The static balance test was performed with the subject standing on the platform on both feet, folding their arms across their chest. Subjects stood with the second toe of both feet on the parallel lines to the y-axis located 10.5 cm away from this axis, and the top of their foot intersecting with the x-axis. Before the test, each person was allowed a 3-min practice period. For the static balance test, they were asked to keep the red “×” sign at the centre of the platform in the centre of the screen for 30 s.
Postural sway was evaluated using the Emed®-x400 pedobarography platform (Novel Gmbh, Munich, Germany). This device has a 6,080 capacitative sensors (4 sensors/cm2) arranged within an area of 475 × 320 mm, recording at a sampling frequency of 100 Hz. Postural sway was assessed by measuring the maximal amplitude of anteroposterior and mediolateral displacements from the centre of pressure (COP). The pattern of COP was recorded while patients stood still for 30 s, first with their eyes open, and then closed. In addition, patients were asked to shift their weight first onto their affected lower extremity, and then onto their unaffected lower extremity, for 10 s. Postural sway during weight shift to the affected side (WSAS), and to the non-affected side (WSNS), was assessed using COP shift from the midpoint. Total mediolateral COP displacement during weight shifting (TWS) was also calculated. To standardize the distance between the patients’ feet for the purposes of measurement, foot positions on the KAT 3000 platform were drawn with an acetate marker pen on the Emed-X platform, and the measurements were performed with patients’ feet placed on these marked positions. To determine the level of independence of, and assistance required by the patients with regards to transfer and locomotion, FIMt and FIMl sub-scores were evaluated. FIM was adapted to our society, and the scale was demonstrated to be valid for stroke patients (20, 21).
All patients who met the inclusion criteria during the study period were included into the study. Since the number of inpatient stroke patients meeting the inclusion criteria was limited, the sample size could not be calculated before the study started. Randomization was undertaken with a block size of 2. The baseline characteristics of the patients are summarized in Table I. To assess the differences between the 2 groups (group effect), within each group over time (time effect), and the interaction between group and time (group–time interaction), the repeated measures analysis of variance (rANOVA) was used. Data are presented as mean (standard deviation; SD). The significance threshold was set at 0.05, with no adjustment for multiple comparisons. Statistical significance was accepted at p < 0.05. The Statistical Package for the Social Sciences (SPSS) for Windows, version 17, was used for statistical analysis.
Table I. Demographic and clinical features of the patients in the experimental and control groups
All patients in the experimental group completed their exercise programme (20 sessions) performed with the Wii Fit and Wii Balance Board. All patients in the experimental group reported enjoying the sessions. The demographic and clinical features of the patients are summarized in Table I. With regard to these characteristics, the 2 groups were similar.
The mean values for the primary and secondary outcome measures at admission, and after 4 and 8 weeks for both groups are shown in Tables II and III. There were no significant differences between the groups in terms of the primary and secondary outcome measures at admission (p > 0.05).
Table II. Mean values of primary outcomes for the experimental and control groups
Table III. Mean values of postural sway parameters, Functional Independence Measure (FIM) transfer and locomotion scores for the experimental and control groups
When the data were evaluated using the repeated measures analysis of variance, no group effect was detected in relation to any of the parameters (p > 0.05). The results showed significant improvement over time (time effect) in all the measures except anteroposterior COP displacement with eyes closed, COP displacement during WSNS, and total COP displacement during weight shift. Group–time interaction was significant in the BBS, FRT and postural sway parameters, except mediolateral COP displacement with eyes closed, and FIMl scores, suggesting that, while both groups exhibited significant improvement, the experimental group showed greater improvement than the control group (Tables IV and V).
Table IV. Group effect, time effect and group-time interaction for primary outcome measures
Table V. Group effect, time effect and group-time interaction for postural sway parameters, Functional Independence Measure (FIM) transfer and ambulation scores (secondary outcome measures)
The use of VR exercises employing Wii has increased since 2010, and has focused mainly on rehabilitation of the upper body (22). Several studies have investigated the use and efficacy of VR applications using Wii Fit on balance in stroke patients. Our study explores the effectiveness of Wii Fit in balance rehabilitation as an adjunctive therapy to traditional treatment.
Our results demonstrated no group effect on any of the parameters. In relation to the time effect, which reflects change over time, all parameters other than anteroposterior eyes closed, WSNS and TWS were found to be statistically significant. This signifies that both groups improved significantly with treatment. The group–time interactions and the changes in BBS, FRT and secondary outcome measures, except mediolateral COP displacement with eyes closed and FIMl scores, were dissimilar, with the change over time favouring the experimental group.
Despite the significant improvements observed in terms of BBS and FRT, the change in TUG test scores was not significant. This might be due to the rising, walking and sitting tasks comprising the TUG test not being addressed by the exercises performed with the Wii Fit. Although the PASS results showed significant improvement in both groups, the degree of improvement did not differ between the groups over time. This might be because the validity of the PASS test is proven in the first 3 months following a stroke, while the patients included into our study experienced a stroke less than one year before the study period. It was also observed that the anteroposterior COP displacement with eyes both open and closed, and eyes open mediolateral COP displacements, which were used to evaluate postural sway, had also shown a greater improvement in the experimental group than the control group. In the experimental group, measurements that evaluated mediolateral weight shifting were identified as having improved in comparison with the control group, which could be due to a number of the exercises performed with the Wii Fit focusing mostly on weight shifting in the mediolateral plane. While WSAS had changed over time, the degree of change over time in WSNS was not statistically significant. This could be attributed to WSNS being in a better state than WSAS before the commencement of treatment. Gil-Gomez et al. investigated the effect of Wii Balance Board-based virtual rehabilitation in chronic stroke patients using both static and dynamic balance scales. They detected significantly greater improvements in the BBS and anterior reach tests in patients receiving virtual rehabilitation compared with traditional treatment (23). The results of the current study are in accordance with these results. Our study also evaluated postural sway and found significant improvements in favour of virtual rehabilitation. In addition, our study demonstrated that the positive effects of virtual rehabilitation continue into the follow-up period (even after termination of the treatment). In contrast to Gil-Gomez et al (23)., we included patients with a stroke history of less than one year, and showed that Wii-based balance exercises were also effective in the earlier stages of stroke. A single-blind randomized-controlled trial designed by Bower et al. (24) investigated the clinical feasibility of the Wii Fit for the treatment of balance difficulties in the early stages of stroke. They detected greater improvements in the step test and FRT in the experimental group. They also suggested that Wii-based treatment is useful in early phase post-stroke rehabilitation.
One of the most significant problems with Wii-based virtual rehabilitation is the fact that the games and exercises included in the package are designed for healthy people. As mentioned by Anderson et al. (25), stroke patients might find the Wii games difficult. The games used in our study were the ones included in the standard Wii Fit package. As a result, only patients who could stand on the Wii Balance Board were included in the study. Even if this held the potential to influence the baseline values, both groups demonstrated significant improvement over time. When we consider the group–time interactions, BBS, FRT, postural sway parameters (except mediolateral eyes closed) and FIMt all improved in the experimental group. The absence of a group effect confirms the comparability of the 2 groups, so it is possible to say that the improvements effected in the 2 groups were dissimilar, and that the results favour virtual rehabilitation.
The balance exercises we used included weight shifting activities. These were aimed at improving postural control by increasing anteroposterior and mediolateral weight transfer. As postural control is a prerequisite for most functional activities, weight shifting exercises aimed at improving postural control may have significant effects on balance during functional activities. The functional balance measurements used in our study (BBS, TUG and FRT) showed that functional performance was improved in both groups.
In the study by Clark et al., the Wii Balance Board was compared with a perturbation platform, which is considered the gold standard in its field. The study demonstrated that the Wii Balance Board is a valid and clinically useful device (26). Furthermore, the Wii Balance Board is cheaper, lighter, and more portable. Other advantages of VR applications mentioned in the literature include being more acceptable to patients given their ease of use, and being more entertaining (27). In our study, patients in the experimental group easily adapted to this exercise method, and all of the patients exhibited eagerness to continue the exercise programme. In addition, there were no accidents that threatened the well-being or safety of the patients during the sessions.
It is not clear from the literature what the optimal duration of a VR exercise programme would be. In our study, patients performed VR exercises for a 4-week period, for 5 days a week and 20 min a day. In Gil-Gomez et al.’s study, participants undertook 20 1-h sessions (23). Despite the brief exercise periods utilized in our study, we obtained favourable results. A more intense and longer application of Wii Fit could increase the effectiveness of the rehabilitation. There is a need for further studies evaluating the effects of rehabilitation duration and intensity.
One of the limitations of our study was the short follow-up period following the completion of the exercise programme. It is difficult to evaluate the long-term balance performance of these patients based solely on evaluations performed 4 weeks after the exercises were completed. Hung et al. (28) compared the relative effectiveness of Wii Fit training and conventional weight shifting training on balance in stroke patients. They also investigated the long-term effects of these 2 approaches. Both groups showed significant improvement in dynamic balance tests, and these effects were preserved in the 3-month follow-up. Wii Fit training was also found to be more effective in improving static standing stability, but, in contrast to our findings, these effects were not preserved in the follow-up. In Hung et al.’s study, the duration of the Wii-based exercises was shorter than ours and a longer period of time had elapsed between stroke episodes and the beginning of rehabilitation (28).
We included subacute and chronic stroke patients in our study. This can be regarded as a limitation since rehabilitation therapy started in the early period provides better results in patients (29). The most important reason for this is the small number of patients meeting the inclusion criteria. In addition, chronic stroke patients in our study had not received prior rehabilitation therapy. Also, in these patients it has not been over 1 year since the stroke. The time since the stroke was not statistically different in the experimental and the control groups (p=0.758).
Morone et al. (30) investigated the efficacy of video game-based balance training on functional balance and disability in subacute stroke patients. This randomized controlled study suggested that Wii Fit training was more effective than standard balance therapy at improving functional balance (BBS). We have achieved similar results to those arrived at by Morone et al. (30) concerning BBS by using not only functional balance measurements but also computer-based balance platforms.
Iruthayarajah et al. conducted a systematic review and meta-analysis of the effectiveness of VR at improving balance in a chronic stroke population in 2017 (31). They selected randomized controlled trials published up to September 2015. They categorized the studies into various groups such as Wii Balance Board, VR combined with treadmill training, and postural VR training. Similar to our study, they concluded that, when compared with conventional treatment, VR improves static and dynamic balance. However, in contrast to our study, they also suggested that the Wii Balance Board may not be effective in improving dynamic balance, although further confirmatory studies are necessary.
In conclusion, this study showed that Wii Fit-based balance rehabilitation could represent a useful adjunctive therapy to traditional treatment to improve static and dynamic balance, functional motor ability, and independence in stroke patients. However, the results of this pilot research (with a small sample size) must be viewed with caution, and as the basis for further research to establish the comparative effectiveness of this therapeutic approach in stroke rehabilitation.
This study was supported by Gazi University scientific research grant number 01/2009-13.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize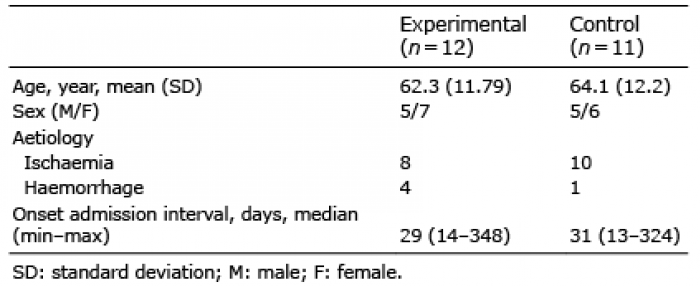 Click to show fullsize
Click to show fullsize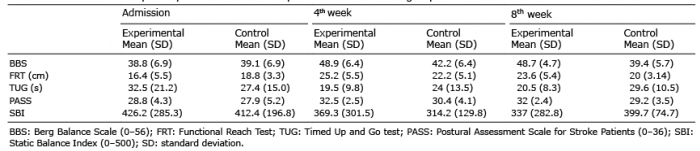 Click to show fullsize
Click to show fullsize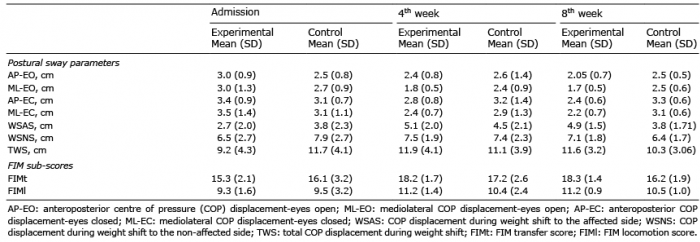 Click to show fullsize
Click to show fullsize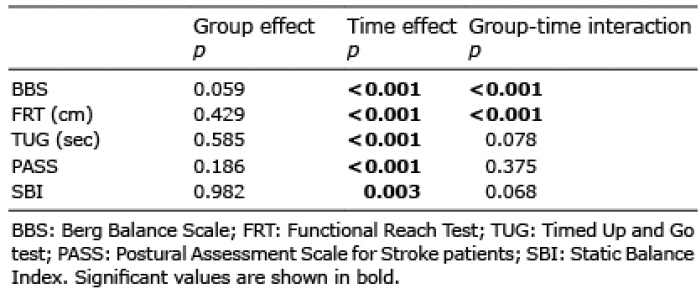 Click to show fullsize
Click to show fullsize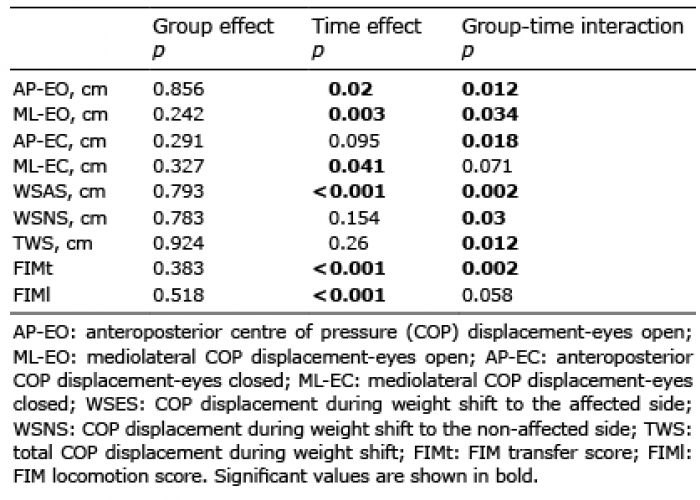 Click to show fullsize
Click to show fullsize