
From the 1Department of Physical Medicine and Rehabilitation, 1APHM, Hôpital de la Timone Hospital, 2Aix Marseille University, CNRS, INT UMR 7289, and 3Aix-Marseille University, Inserm, IRD, UMR912, SESSTIM, Marseille, France
Objective: To assess the efficiency of knee-ankle-foot orthoses for treating painful genu recurvatum, and to determine users’ tolerance and satisfaction.
Patients: Patients included in the study had a genu recurvatum during the stance phase, confirmed by a medical doctor on physical examination. A total of 27 patients with 31 knee-ankle-foot orthoses were included.
Methods: The main outcome was scored on a verbal numerical rating scale (VNRS) before and at least 3 months after a knee-ankle-foot orthosis was fitted, and scored on a verbal numerical pain rating scale (VRS). Secondary outcomes were rated with the Quebec User Evaluation of Satisfaction with assistive Technology (QUEST).
Results: After fitting the knee-ankle-foot orthosis, the median VNRS pain score decreased from 85/100 to 25/100 (p ≤ 0.001) and the description of pain on the VRS decreased from “extreme” to “mild” (p ≤ 0.001). The QUEST total score was 4.0.
Conclusion: Treating a painful genu recurvatum with a knee-ankle-foot orthosis reduced the pain efficiently whatever the patients’ diagnosis, and high scores were obtained for patients’ satisfaction.
Key words: knee-ankle-foot orthosis; KAFO; genu recurvatum; painful recurvatum.
Accepted Feb 21, 2018; Epub ahead of print Mar 27, 2018
J Rehabil Med 2018; 50: 00–00
Correspondence address: Marjorie Kerzoncuf, Département de Médecine Physique et de Réadaptation, 1APHM, Hôpital de la Timone, FR-13385 Marseille, France. E-mail: marjorie.kerzoncuf@ap-hm.fr
Genu recurvatum (GR) is hyperextension of the knee of more than 5°, in which the ground reaction force (GRF) line is anterior to the knee axis (1). GR can occur in various neuromuscular and musculoskeletal diseases, such as myopathy, upper motor neurone diseases, such as stroke, cerebral palsy, multiple sclerosis (2–5), and lower motor neurone diseases, such as poliomyelitis. GR is relatively common in stroke patients, where its rate of occurrence ranges from 40% to 68% (6).
The main physiopathological mechanisms of GR are weakness of the knee extensor, knee extensor spasticity, especially of the quadriceps, weakness of the buttock muscles leading to forward pelvic tilt, lumbar hyper-lordosis and excessive hip flexion compensated by knee hyperextension, weakness of the knee flexors, limited dorsiflexion of the ankle with knee hyperextension due to the patients’ inability to move the tibia forward during the stance phase, avoidance of painful pressure on the ball of the foot or proprioceptive disorders (5, 7).
Depending on the aetiology of GR, treatments include physical therapy, functional methods of electrical stimulation or electrogoniometric feedback (8, 9), botulinum toxin A injections in cases in which GR is due to spasticity (10, 11), orthoses, such as ankle-foot orthoses (AFOs) (12, 13), knee-ankle-foot orthoses (KAFOs) (1), knee orthoses (Swedish knee cages) (14) or hinged soft knee orthoses (15), orthopaedic surgery (16), or selective tibial neurotomy (17). Making clinical decisions in GR is difficult because of the wide range of aetiologies. Step-by-step analysis can be useful to define the main cause of GR and choose the best treatment (18). Studies on orthotic devices for GR have been conducted on AFO and KAFO users (1), the use of knee orthoses (Swedish knee cages) has been assessed (19), and the effectiveness of AFOs vs KAFOs has been compared (20, 21). To assess the effectiveness of KAFO treatment, some authors have analysed the improvement in gait parameters (20–24), while others have studied energy savings (13, 25–28).
In our clinical practice, posterior knee pain resulting from a GR, which is a frequent reason for consultation, consists of pain in the posterior structures of the knee associated with abnormal stretching of the posterior joint capsule and posterior knee ligaments. When repetitive loading occurs, posterior joint laxity can develop as a result of the tensile forces exerted on the posterior capsule, generating posterior articular, muscular and tendon pain (5, 7, 29–31), which can lead to a KAFO being fitted in order to restrict the GR and reduce the pain. Depending on the aetiology and cause of GR, a KAFO with a free knee joint and a posterior offset can be prescribed to reduce the pain. Several studies have described the effects of orthoses on gait parameters (14, 21, 22, 32), but no studies have focused on their effects in terms of pain relief.
The aim of this study was to assess the efficiency of KAFOs for treating painful GR and to determine users’ tolerance and satisfaction.
This retrospective study was conducted on patients who had been fitted with KAFOs in order to alleviate posterior knee pain resulting from GR at our outpatient department of Physical and Rehabilitation Medicine. Data used were collected by an investigator who was not involved in the subjects’ treatment.
Participants provided informed verbal consent after being given information about the study.
Inclusion criteria. Patients with painful GR were included in the study. GR was defined as abnormal hyperextension of more than 5° (measured with a goniometer at physical examination) and by a ground reaction force line anterior to the knee axis during the stance phase (with the hip in the anatomical position). The indication for a KAFO was pain and not instability. Patients included in this study had to be at least 18 years of age and able to understand and answer the questionnaire. Patients with cognitive disorders, particularly memory disorders, were excluded. Additional inclusion criteria were a gait perimeter of more than 10 m without the KAFO, and having worn the orthosis for more than 3 months since the last correction.
Assessment was performed after the KAFO was fitted, and had been worn for at least 3 months, because of the retrospective nature of the study. Data were collected through patient questionnaires.
The patient may also have had other pain localizations, but we only consider pain related to wearing a KAFO. Because of the retrospective nature of the study knee pain without the KAFO was evaluated by patients when they walked without the KAFO, even if they had already been fitted with a KAFO.
The Quebec User Evaluation of Satisfaction with assistive Technology (QUEST) was used to measure patient satisfaction with the orthosis. This questionnaire comprises 12 satisfaction items (8 questions about the orthotic device, its dimensions, its weight, whether it was easy to adjust, its safety and security, its durability, whether it was easy to use, comfort, and effectiveness, and 4 questions about the services involved: its delivery, repairs and maintenance, and the professional services and follow up services), where all the responses to these items give a quantitative score (19, 34), as follows: 1: “not satisfied at all”; 2: “not very satisfied”; 3: “more or less satisfied”; 4: “quite satisfied”; and 5: “very satisfied”.
The following 5 subjective gait parameters were rated without and with the KAFO: “much improved” [+2], “improved” [+1], “no difference” [0], “worse” [–1], “much worse” [–2] (35, 36) and scored only by patients:
Tolerance of the KAFO was assessed as follows:
We asked patients about falls before and after delivery of the orthosis: (“falls: yes/no”).
Paired Wilcoxon tests were used to analyse differences between the pain assessments (in terms of the VNRS and VRS scores) before and after a KAFO was fitted. McNemar’s test was used to compare the proportion of fallers before and after the KAFOs were fitted. To calculate the results of the QUEST, the original methods described in the study by Demers et al. were used (34, 37) with means and standard deviation (SD).
To analyse the quantitative scores, such as the numerical verbal satisfaction scores ranging from 1 to 100, the median, quartiles and range were calculated. In the case of discrete characteristics with available meanings, such as the subjective assessment of walking without and with the KAFO (ranging from +2, “much improved”, to –2, “much worse”), median values, quartiles and range were calculated.
An alpha £0.05 was taken to be statistically significant. All statistical analyses were performed using IBM SPSS Statistics 20.0 software.
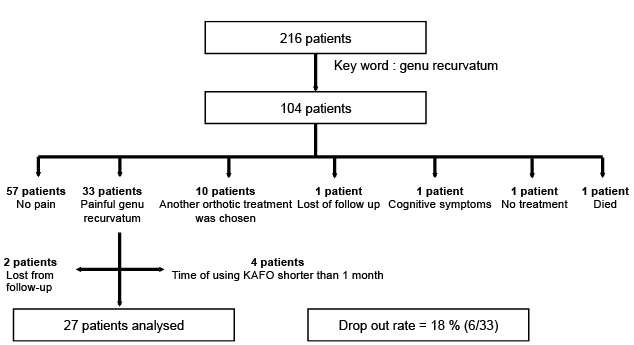
Based on patients’ files recorded between 2007 and 17 October 2014, 216 had a KAFO and 104 had a KAFO to treat GR. In this group of 104 patients, 33 had a KAFO because of a painful GR. Two patients declined to participate in the study, and 4 gave up wearing the KAFO before the end of the first month and declined to participate in the study (Fig. 1).
Fig. 1. Flow chart of the study population selected using the key words “knee-ankle-foot orthosis” and “genu recurvatum” from all the patients attending consultations in our Department of Physical and Rehabilitation Medicine. Only patients who were treated with a knee-ankle-foot orthosis for pain were included, and instability was not taken into account.
Patients’ characteristics. The patients’ characteristics and the types of KAFO are shown in Table I.
Table I. Characteristics of the patients’ in the study population (n = 27)
Diagnoses and clinical examination data. The patients’ diagnoses, range of motion, and muscular strength are shown in Tables II and III.
Table II. Patients’ diagnoses under 3 headings: upper motor neurone pathologies, lower motor neurone pathologies, and traumatic musculoskeletal lesions.
Table III. Patients’ range of motion (ROM) and muscular strength
KAFO characteristics. Twenty-five KAFOs were prescribed with a free offset knee joint, but a posterior stance axis (posterior offset KAFOs). In these orthoses, an anterior restriction was used in order to maintain the GR in the range in which the patient had no pain and to prevent falls that were liable to occur if the knee extensors were not strong enough. Six KAFOs had a locked knee joint.
Concerning knee pain before and after being fitted with the KAFO, all patients reported an improvement, with the VNRS pain score improving from a median of 85/100 (first quartile = 75; third quartile = 90; range 50–100) to 25/100 (first quartile = 10; third quartile = 35; range 0–75) (p ≤ 0.001), and the VRS pain assessment improving from “extreme” (median = 4; range 2–4)) to “mild” pain (median = 1; range 0–3) (p ≤ 0.001). These results are shown in Table IV.
Table IV. Main outcomes: patients’ mean knee pain assessments before and after wearing a knee-ankle-foot orthosis
The QUEST yielded a total score of 4.0 (SD 0.5), corresponding to “quite satisfied”. The results for each item are shown in Fig. 2.
Fig. 2. Results of the Quebec User Evaluation of Satisfaction with assistive Technology (QUEST 2.0). Mean scores obtained on each of the items in the French version of QUEST 2.0 with standard deviations. (QUEST quantitative score: 1: “not satisfied at all”; 2: “not very satisfied”; 3: “more or less satisfied”; 4: “quite satisfied”; 5: “very satisfied”).
The median values of the subjectively assessed gait parameters without and with the KAFO were:
The mean time spent wearing the orthosis per 24 h was 9.8 h (SD 4.4; range: 2–17). Patients reported that they used their orthosis every day from when they got up in the morning until they went to sleep, in their everyday activities. They had to remove the KAFO to wash themselves and sometimes when using the toilet, because of the size of the orthosis or because it damaged their trousers.
Six patients out of 33 did not fit the KAFO: 2 did not answer any phone calls or e-mails and 4 discontinued using the KAFO before 1 month. Three of the patients refused to fit the orthoses due to its weight, discomfort, and difficulty of use, one of them because the KAFO was inducing instability.
The frequency of fallers (yes or no) was 67% before using a KAFO and 37% afterwards (p = 0.021).
Table V. Median values of the subjectively assessed gait parameters* without and with the knee-ankle-foot orthosis (KAFO)
The aim of this retrospective study was to analyse the efficiency of KAFOs for alleviating painful GR, and users’ satisfaction with this particular choice of treatment. The results show that KAFO is an efficient means of treating posterior knee pain, since it reduced the mean VNRS pain score from 85/100 to 25/100 and the VRS pain assessment from “extreme” to “mild”, and the users expressed satisfaction (based on the QUEST), with a mean score of 4.0, corresponding to “quite satisfied”, whatever their diagnosis and the cause of the GR. The subjective gait parameters and the patients’ impression of GR also improved. Based on the QUEST, the KAFOs rated well in terms of safety, durability and effectiveness, whereas their comfort, weight and dimensions were given the lowest ratings, confirming the clinical assessment and users’ criticisms.
The patients reported that they used their KAFOs every day, removing them only for sleeping, bathing, and getting dressed, and that they wore them for up to 9 h per day, which is quite long. In 2 patients with a recurvatum of only 5°, the VNRS knee pain score decreased from 85 and 80/100 to 60 and 20/100, respectively, which shows that the intensity of the pain does not necessarily depend on the severity of the GR. It should be noted that included patients had worn the orthosis for more than 3 months since the last correction. The latter criterion was adopted in order to study the effects of the final orthoses, but it also shows that when orthoses are accepted, it is with efficiency.
The study population (27 patients) was rather small, which was a limitation of this study, but all previous studies on orthotic devices for patients with GR have been conducted on rather small populations (between 11 and 25 patients (1, 14, 20, 22)) because it is difficult to find larger populations of patients with an indication of KAFO for painful GR. Moreover, the strict inclusion criteria used here resulted in the exclusion of all patients with instability, in order to assess the effects of KAFOs on pain and not on instability, although both symptoms often occur concurrently. This is another reason for the small sample of patients in this study. A further limitation of the present study is that, since patients with musculoskeletal and neurological diseases were included, a heterogeneous population was obtained, which is typical of KAFO users. This heterogeneity confirmed the significance of our results. However, for an homogenous group, such as the group of patients with poliomyelitis, it was observed that wearing KAFOs reduced their knee pain scores from 83/100 on the VNRS scale to 29/100, and good ratings of patients’ satisfaction (QUEST = 4.1) were obtained, even on the item “comfort” (3.5/5). Although poliomyelitis patients in general do not have sensory disorders, they were highly sensitive to the pressure exerted by the orthosis (38, 39).
This retrospective study is the first step in the second part of a larger ongoing study with a prospective design. The retrospective approach included assessment after the KAFO was fitted, which may influence the results. Patients included in this study were fitted with a KAFO because of the efficiency of the device. In the second part of the study, using a prospective approach, data will be collected before making the decision to apply orthoses, and kinematic parameters (based on optoelectronic technology with a Helen Hayes marker set up (26)) will be recorded and used to define the cause of the GR and calculate the mechanical energy expenditure (40) and the efficiency of the angular correction before and after orthotic correction. The second question to address in order to improve the medical management of GR, is what range of motion of the knee is required with the KAFO in order to reduce knee pain but not create instability of the knee.
Treating painful posterior GR with KAFOs was found to be an efficient means of alleviating pain, regardless of the patients’ diagnoses. This method met with a good level of patient satisfaction. Further research is needed in order to develop an effective approach to management of GR.
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize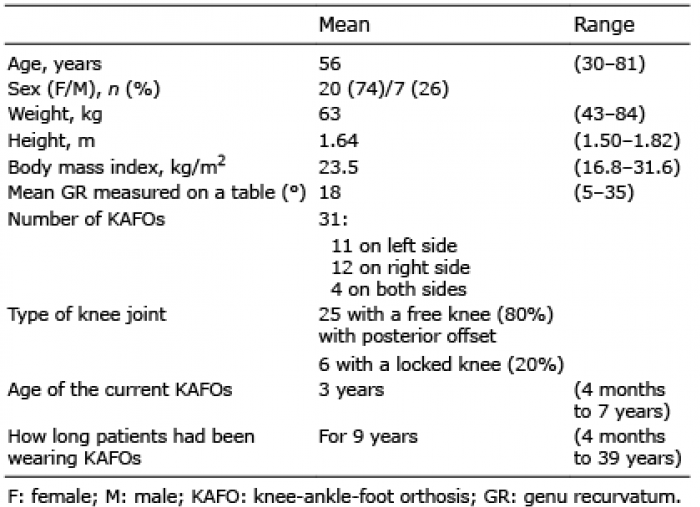 Click to show fullsize
Click to show fullsize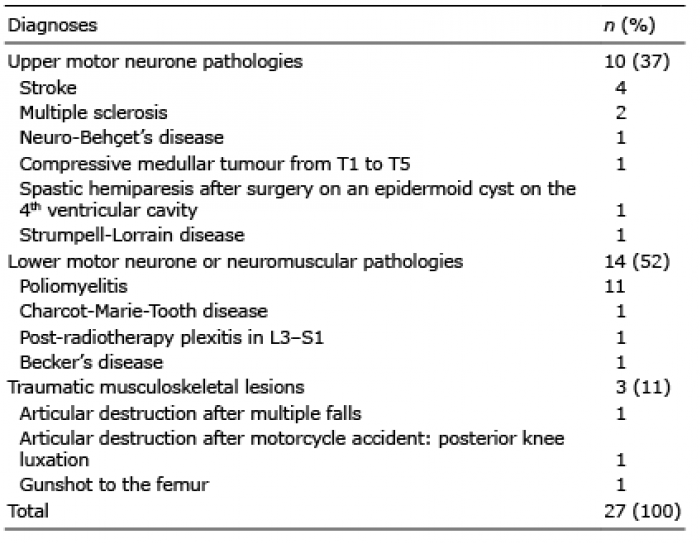 Click to show fullsize
Click to show fullsize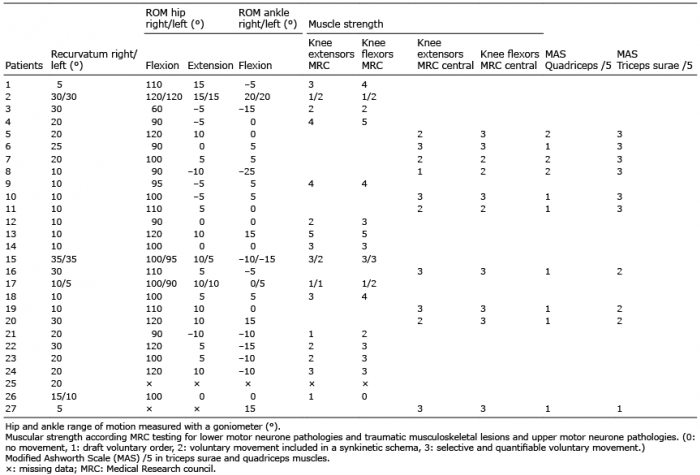 Click to show fullsize
Click to show fullsize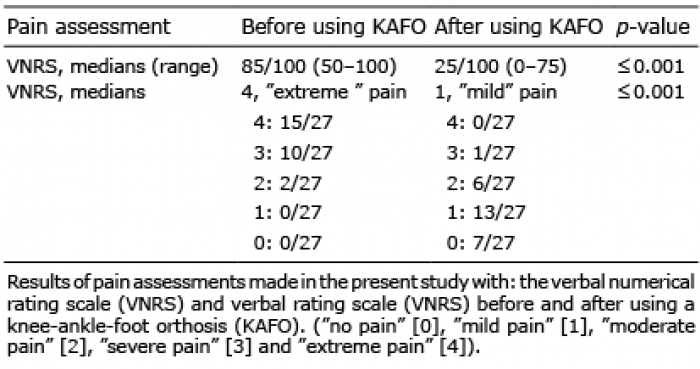 Click to show fullsize
Click to show fullsize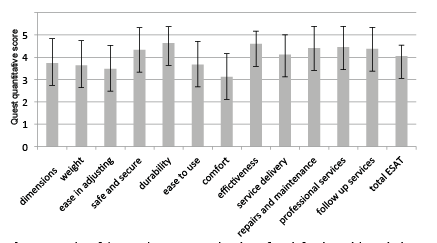 Click to show fullsize
Click to show fullsize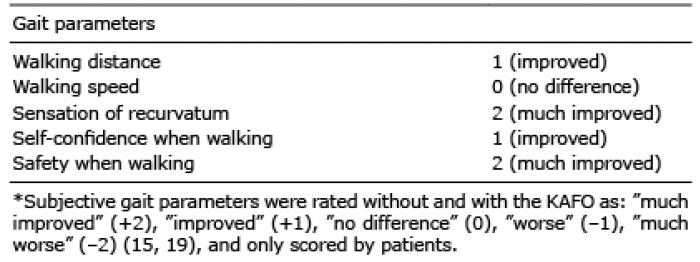 Click to show fullsize
Click to show fullsize