
From the 1Rehabilitation Centre Leijpark, Libra Rehabilitation Medicine & Audiology, Tilburg, 2Rehabilitation Centre Tolbrug, Jeroen Bosch Hospital, ‘s Hertogenbosch, 3Department of Rehabilitation Medicine, and 4Department of Oral and Maxillofacial Surgery, University of Groningen, University Medical Centre of Groningen, Groningen, 5Department of Rehabilitation Medicine, Maastricht University Medical Center, Maastricht, and 6Amsterdam Rehabilitation Research Centre | Reade, Amsterdam, The Netherlands
Objective: To describe the prevalence of comorbidity and its relationship with demographic and clinical characteristics in persons wearing a prosthesis after lower-limb amputation.
Design: Cross-sectional study.
Subjects/patients: Persons wearing a prosthesis after lower-limb amputation (n = 171; mean age 65 years (standard deviation 12); 72% men) at the end of outpatient rehabilitation treatment.
Methods: Comorbidity was assessed with the Func-tional Comorbidity Index: a list of 18 items addressing the presence of specific comorbid conditions impacting on functional status. Comorbidities in medical records were assessed independently by 2 assessors. Associations with demographic and clinical characteristics were analysed using linear or logistic regression.
Results: The median (interquartile range) number of comorbidities was 3 (2; 4). Three or more comorbidities were present in 103 of 171 (60%) participants. Diabetes was present in 71 (41%), cardiac disease in 60 (35%), and lumbago/degenerative disc disease in 39 (23%) participants. The prevalence of comorbidities was higher in women and those with vascular cause of amputation.
Conclusion: There is a high prevalence of comorbidity at the end of outpatient rehabilitation treatment in persons wearing a prosthesis after a lower-limb amputation, especially in women and those with vascular cause of amputation.
Key words: amputation; comorbidity; prosthesis; rehabilitation.
Accepted Jan 12, 2018; Epub ahead of print Jun 8, 2018
J Rehabil Med 2018; 50: 00–00
Correspondence address: Fred A. de Laat, Rehabilitation Centre Leijpark, PO Box 5022, NL-5004 EA Tilburg The Netherlands. E-mail: f.delaat@libranet.nl
Persons who have undergone an amputation of a leg, frequently suffer from other diseases. Because these other diseases can influence prosthetic training, especially exercise therapy, we explored which diseases at which frequencies are prevalent at the start of the prosthetic training. We found that the prevalence of diseases was higher in women and those with an amputation caused by vascular disease. The most prevalent diseases were, besides vascular disease, diabetes, lumbago, and arthritis. Especially women had a higher prevalence of arthritis and anxiety or panic disorders. Therefore we recommend to screen for these diseases actively in women, because it may be necessary to adapt the prosthetic training for these persons.
Comorbidity has been defined as “any distinct additional clinical entity that has existed or that may occur during the clinical course of a patient who has the index disease under study” (1). Comorbidity is becoming more and more relevant, both for daily clinical practice and research, given the ageing of modern societies, the increased survival from diseases and, related to this, the increase in so-called chronic diseases (2). Related to this, there is increasing interest in the impact of comorbidity on study populations (3, 4).
Persons with a lower-limb amputation (LLA) often experience comorbidity (5–7) and the presence of comorbidity may impact on their mobility (8–10). The presence of comorbidity can influence medical care during rehabilitation treatment, as well as the length of rehabilitation treatment. From a review of the literature until 2007 it was concluded that the impact of comorbidity on functional outcome, especially mobility, is inconsistent (11). More recent literature, however, provides evidence that comorbidity does impact on mobility (8–10).
We are aware of 3 studies assessing the prevalence of comorbidity as a primary outcome in persons with a LLA (5–7). One study included 24, mainly young, persons with a traumatic cause of amputation (5), whereas persons seen in daily clinical practice in rehabilitation medicine are predominantly elderly with a vascular cause of amputation (12). Another study used available administrative data only, and did not use data from medical records (6). A third study addressed a sample of nursing home residents older than 67 years undergoing a LLA (7), of whom only a minority will function with a prosthesis. The majority of persons with a LLA seen in daily clinical practice in rehabilitation medicine will function with a prosthesis. The studies did not clarify in detail how the presence of comorbidity was assessed. In addition, the presence of comorbidity was not assessed at the end of outpatient rehabilitation treatment, which is, in our view, the phase that is the most relevant for daily functioning at home.
To our knowledge, the association of demographic and clinical characteristics with prevalence of a wide range of specific comorbidities has not yet been studied in persons wearing a prosthesis after a LLA at the end of their rehabilitation treatment. Elucidating these associations would enable the specification of patients at risk of comorbidities. Moreover, studying these associations enables better predictions with respect to the number and presence of specific comorbidities in patients who differ with respect to age, sex, or type of amputation. Finally, studying these associations enables better comparison of studies that include samples of persons after a LLA who differ with respect to demographic or clinical characteristics.
The first aim of this study was to assess the prevalence of comorbidity in persons wearing a prosthesis after a LLA at the end of rehabilitation treatment. The second aim was to analyse associations of comorbidity with demographic and clinical characteristics.
Participants were persons with a recent LLA who were recruited at the end of their rehabilitation treatment. The first group consisted of patients at the end of their outpatient rehabilitation treatment (in some cases this had been preceded by inpatient rehabilitation) in the ‘s-Hertogenbosch rehabilitation centre (rehabilitation centre group). The second group consisted of patients directly after discharge from inpatient or outpatient rehabilitation treatment in nursing homes in the ‘s-Hertogenbosch region (nursing home group). These 2 groups encompassed all persons wearing a prosthesis after a LLA and undergoing rehabilitation treatment in this region. Participants had to meet the following inclusion criteria: age ≥ 18 years; currently wearing a prosthesis; and able to understand and complete questionnaires. The study protocol was approved by the Research Ethics Committee of the Jeroen Bosch Hospital, ‘s-Hertogenbosch, The Netherlands.
Data on comorbidity, and demographic and clinical characteristics were extracted from medical records. The rehabilitation centre group received a questionnaire about their mobility from the therapists on the second-to-last day of treatment in the rehabilitation centre. They were asked to complete the questionnaire at home and bring it with them on the final day of treatment. The nursing home group received the questionnaire during their first follow-up appointment in the rehabilitation centre. They were asked to complete the questionnaire at home and return it by post.
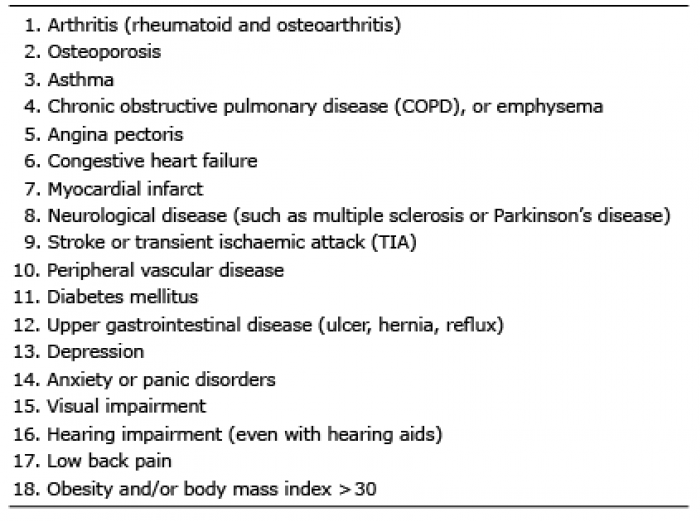
To measure comorbidity, we used the Functional Comorbidity Index (FCI) (13). The FCI consists of a list of 18 items assessing the presence of several comorbidities (yes/no). The total score is calculated by summing items scored “yes”. The FCI has been proven to have a good conceptual framework (13). FCI scores correlated (r = 0.54) with the physical function subscale of the Short Form-36 Health Survey (13). The FCI is easy to administer, as only summation regarding the presence or absence for 18 diagnoses is required, and thus weighting of diseases is not necessary. To obtain the most reliable FCI score, we used a method described previously (14): 2 medical doctors (F.A.d.L. and an independent medical doctor) studied the protocol for scoring instructions of the FCI, studied the medical records and then scored the presence of all 18 diagnoses independently. A comorbidity was defined as being present if it was described in an outgoing medical letter of the medical doctor or if it was coded as such in the (digital) medical records of the rehabilitation centre, nursing home or hospital. In case of disagreement, each score was discussed until consensus was reached. Appendix 1 provides an overview of the comorbidities included in the FCI.
Demographic (age, sex) and clinical characteristics (cause, level and sidedness of amputation, and setting) were recorded. Functional mobility was assessed using 4 self-reported questionnaires: the Walking Questionnaire (WQ35) (15, 16), the Climbing Stairs Questionnaire (CSQ15) (17, 18), the Rising and Sitting Down Questionnaire (R&SDQ39) (19–21) and the Locomotor Capabilities Index (LCI) (22).
The WQ35 assesses activity limitations in walking. It contains 35 items with dichotomous response options (yes/no). The sum score is calculated by adding scores for the 35 items. A standardized sum score ranges from 0 to 100, with higher scores indicating less limitation in walking (15). The Walking Questionnaire had good construct validity and test–retest reliability in persons with a LLA (23).
The CSQ15 assesses activity limitations in climbing stairs. It contains 15 items with dichotomous response options. The sum score is calculated by adding scores for the 15 items. This score is subsequently standardized (range 0–100, with higher scores indicating less limitation in climbing stairs). Patients can mark a 16th item if they do not climb stairs at all because of their health, and these patients are given a score of 0 (17). The questionnaire has been tested in persons with a LLA and exhibited good construct validity and test–retest reliability (24).
The R&SDQ39 assesses activity limitations in rising and sitting down. It contains 39 items with dichotomous response options. The standardized sum score is derived from the 1-parameter logistic model (range 0–100, with higher scores indicating less limitation). The R&SDQ39 is a unidimensional scale. It has good fit with a parametric item response theory model, the 1-parameter logistic model, good intratest reliability and good content validity (19, 20). The R&SDQ39 showed good construct validity and test–retest reliability in persons with a LLA (25).
The LCI assesses a range of locomotor activities, such as rising from a chair or the floor, walking on a variety of surfaces, and climbing stairs and kerbs. It consists of 14 items with 4 response options: unable (score 0), able if someone helps me (score 1), able if someone is near me (score 2), or able alone (score 3). The sum scores range from 0 to 42, with higher scores indicating more locomotor capabilities (or less limitation). The construct validity and the test–retest reliability of the LCI have been reported to be good (22).
Appendix 1. The Functional Comorbidity Index
The total number of comorbidities and the presence of specific comorbidities with counts (percentages) was recorded. With the comorbidity total score or the presence of specific comorbidities as the outcome, the patient characteristics were analysed univariately for their association, using non-parametric statistics. The level of significance was set at p ≤ 0.05. Associated variables (p ≤ 0.10) were subsequently entered into a linear regression model (total score) and logistic regression models (specific comorbidities) as predictors. Through backward stepwise elimination, the non-contributing variables (p > 0.05) were excluded. All statistics were calculated using SPSS 18.0 for Windows (SPSS Inc., Chicago, IL, USA).
A total of 175 persons with a LLA met the criteria, and all participated in the study. Data regarding the comorbidity were not available for 2 participants. Characteristics of the remaining 173 participants are summarized in Table I. The mean age ± standard deviation (SD)) of these participants was 65 years (SD 12) and 72% of the participants were men.
Table I. Patient characteristics
The FCI total score ranged from 0 to 8, with a median (IQR) of 3 (2; 4). Of the participants, only 8 (5%) had no comorbidities, whereas 103 (60%) had 3 or more comorbidities (Table I). In total, 60 persons with a LLA (35%) had at least one of the following 3 cardiac diagnoses: angina pectoris, congestive heart failure, or myocardial infarction.
Univariate and multivariate relationships of the total number of comorbidities with demographic and clinical characteristics are summarized in Table II. Univariate analysis showed a relationship (p ≤ 0.05) with age, sex and amputation aetiology. Multivariate analysis showed that women and persons with vascular cause of LLA had more comorbidities.
Table II. Prevalence of total number of comorbidities and their associations with patient characteristics
The prevalence of The prevalence of the 2 most important comorbidities is presented in Table III . The complete version of Table III with all specific comorbidities and their associations is available in Table SI1. Besides peripheral vascular disease (83%) and diabetes (41%), there was a high prevalence of lumbago (23%) and rheumatoid arthritis or osteoarthritis (22%).
Table III. Prevalence of specific comorbidities and their associations with patient characteristics
Univariate and multivariate relationships between specific comorbidities and demographic and clinical characteristics are summarized in Table SI1. The following univariate and multivariate relationships were found:
A high prevalence of comorbidities was found in persons wearing a prosthesis after a LLA, with most of them having 3 or more comorbidities. The prevalence of comorbidities was higher in women and in those with vascular cause of amputation. The most prevalent comorbidities (> 20%) were peripheral vascular disease, diabetes, lumbago, and rheumatoid arthritis or osteoarthritis. The prevalence of these comorbidities was related to demographic and clinical characteristics.
The study population was the total number of persons from the ‘s-Hertogenbosch region wearing an prosthesis after a LLA. The study population is representative of the whole of the Netherlands with regard to cause and level of amputation (12). In general, in the Netherlands, rehabilitation physicians are consulted when hospitalized persons have undergone a LLA. Persons will be referred to a rehabilitation centre only if the rehabilitation physician predicts that the patient will be able to use a prosthesis. For this reason we focused in our study on persons wearing a prosthesis. This study population may differ from other countries where, for instance, all persons with a LLA are referred to a rehabilitation centre.
There are several instruments for scoring comorbi-dity, but many of them have primarily been developed to predict mortality. The FCI was applied because it was developed to predict physical function (13), which, in our view, is key to rehabilitation medicine. The FCI has been applied, so far, in persons after stroke (median FCI score 2, range 0–12) (26) and in critically ill patients with acute lung injury (median FCI score 2, interquartile range 1–3) (27). For future studies we recommend validating the application of the FCI in patients with a LLA by studying its association with the functioning level of persons with a LLA.
Because the prevalence of comorbidity in persons with a LLA has so far been assessed using other selection criteria, procedures, and instruments, it is difficult to compare the current results with previous studies (5, 6). This concerns the total number of comorbidities as well as the prevalence of a specific comorbidity, such as diabetes, stroke, or a cardiac disease (8, 28) or hemiplegia in persons with a LLA (9). A recent study assessed pre-operative comorbidities in patients revascularized for critical limb ischaemia. Of this population, 19% underwent a LLA within 3 years. That study showed similar results concerning the incidence of stroke, diabetes, COPD and having had a myocardial infarct. The incidence of angina pectoris and heart failure was higher in their study, but they showed a substantial mortality after revascularization (29). A recent study regarding the incidence of anxiety or depression amongst persons after a LLA, due to diabetes, showed even higher incidences of anxiety or depression (30). For future research, we recommend a standardized description of comorbid conditions in studies of persons with a LLA. If the validation studies of the FCI in patients with LLA yield satisfactory results, the FCI might be the measurement instrument of first choice enabling a standardized assessment and description.
In the current study higher age was associated with higher prevalence of rheumatoid or osteoarthritis. The higher prevalence of osteoarthritis in persons with a LLA has been demonstrated previously, but these studies addressed persons with a LLA of traumatic origin and wearing a prosthesis for a longer time (31, 32). In those studies the higher prevalence, compared with the general population, was interpreted as the result of walking with a prosthesis. This interpretation seems an unlikely explanation for our study, where most persons had a prosthesis prescribed for the first time. We are not aware of studies assessing arthritis in persons with a LLA before the prescription of a prosthesis and the start of prosthetic training.
Female sex was associated with a higher total number of comorbidities and with several specific comorbidities, such as lumbago, rheumatoid arthritis or osteoarthritis and anxiety or panic disorders. These comorbidities can influence the functional outcome of prosthetic training. The relationship between female sex and poorer outcome has been described previously (7). This relationship might, in part, be mediated by the higher number of comorbidities.
The relationship between vascular cause of amputation and comorbid peripheral vascular disease was not further analysed in this study because we consider both to be exponents of the same underlying disease. Surprisingly, non-vascular cause of amputation was correlated with a higher prevalence of rheumatoid or osteoarthritis. The reason for this is unclear. We are not aware of studies addressing this relationship.
Comorbidity is one of the factors used to describe the health status of a study population. Given the high prevalence of comorbidities and the impression that medical records are often incomplete (as rehabilitation centres do not always have access to the hospital data) with respect to comorbidities, we recommend registering comorbidities at the start of prosthetic training.
In older persons and females we found a high prevalence of rheumatoid arthritis or osteoarthritis. These comorbidities may interfere with prosthetic training, especially exercise therapy. Therefore we recommend actively screening for these comorbidities, especially in persons reporting arthralgia. It may be necessary to adapt the prosthetic training in order to avoid the side-effects of training. It was also found that females, in comparison with males, had a higher prevalence of anxiety or panic disorders. Therefore we recommend actively screening for this comorbidity, because this is not always noted in the medical record. It may be necessary to adapt the prosthetic training to more task- and context-specific training with the principles of graded exposure (33).
Knowledge of the relationship between comorbidities and mobility in persons wearing a prosthesis is limited. A recent review, addressing the relationship between the presence of hemiplegia and ambulation and independence in persons with a LLA and wearing a prosthesis (9), showed that hemiplegia resulted in a lower rates of successful ambulation and independence. A recent study found a relationship between the total number of comorbidities and perceived limitations in climbing stairs (10). Another recent review addressing the relationship between the presence of cardiovascular diseases and mobility in persons with a LLA (8) showed that cardiovascular diseases were associated with a smaller chance of becoming a prosthetic walker and with poorer mobility outcomes. For future research we recommend studying the relationship between the most prevalent comorbidities (peripheral vascular disease, diabetes, lumbago arthritis) and mobility in persons with a LLA and wearing a prosthesis.
This study has some limitations. First, it assessed only the presence of specific comorbidities; the severity of these comorbidities was not assessed. Secondly, it included only those persons with a LLA who were wearing a prosthesis at the end of their treatment. Therefore, the results cannot be generalized to persons with a LLA not wearing a prosthesis. Finally, the FCI has been validated in 2 large, multi-site, national, general databases (9), but not specifically in persons with a LLA. However, as far as we know, none of existing comorbidity indices is validated for persons with a LLA.
There is a high prevalence of comorbidities at the end of rehabilitation treatment in persons wearing a prosthesis after a LLA, especially in women and those with vascular cause of amputation. We recommend a standardized description of comorbid conditions in patients with LLA.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize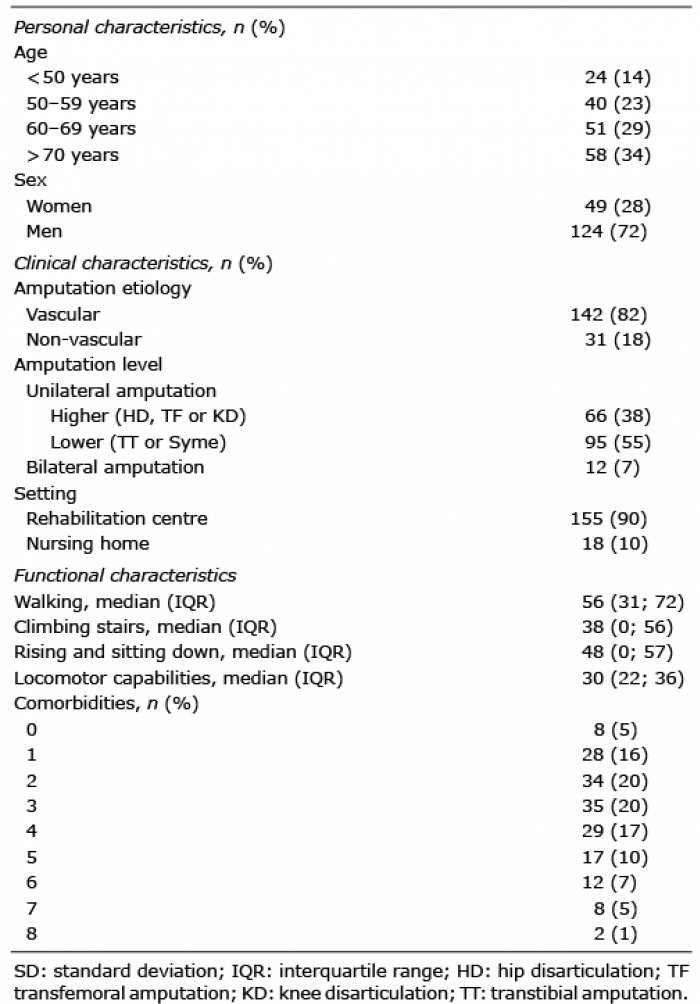 Click to show fullsize
Click to show fullsize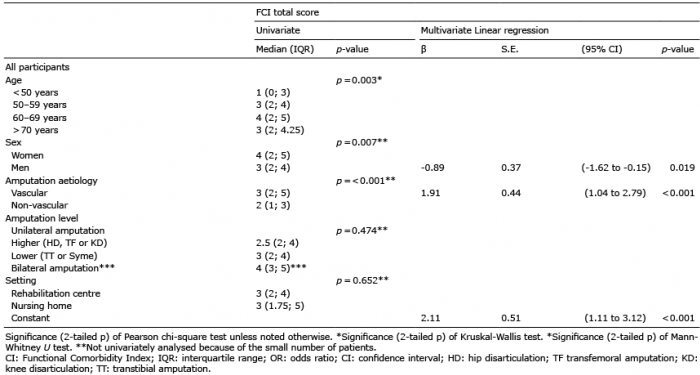 Click to show fullsize
Click to show fullsize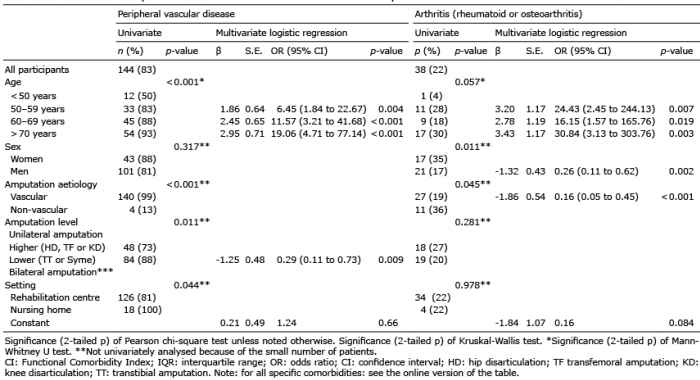 Click to show fullsize
Click to show fullsize