
From 1Rijndam Rehabilitation, and 2Erasmus MC, University Medical Center Rotterdam, Department of Rehabilitation Medicine, Rotterdam, The Netherlands
Objective: To compare 2 configurations of transcranial direct current stimulation (tDCS) for treatment of aphasia.
Design: Randomized cross-over study.
Subjects: Patients with chronic post-stroke aphasia (n = 13).
Methods: tDCS was combined with word-finding therapy in 3 single sessions. In session 1, sham-tDCS/pseudo-stimulation was applied. In sessions 2 and 3, 2 active configurations were provided in random order: anodal tDCS over the left inferior frontal gyrus (l-IFG) and anodal tDCS over the left posterior superior temporal gyrus (l-STG). The optimal configuration was determined per individual based on a pre-set improvement in naming trained (> 20%) and untrained picture items (> 10%).
Results: Overall, participants improved on trained items (median = 50%; interquartile range = 20–85) and post-treatment performance was highest in the active l-IFG condition (p = 0.040). Of the 13 participants, 6 (46%) showed relevant improvement during active tDCS; either in the l-IFG condition (n = 4; 31%) or in both the l-IFG and l-STG conditions (n = 2; 15%). On the untrained items there was no improvement (median = 0%; interquartile range = 0–0).
Conclusion: This randomized cross-over single-session protocol to determine an optimal tDCS configuration for treatment of aphasia suggests that only performance on trained items can be used as guidance for configuration, and that it is relevant for half of the patients. For this subgroup, the l-IFG configuration is the optimal choice.
Key words: aphasia; electric stimulation; stroke; rehabilitation.
Brain-stimulation techniques are currently being studied as a new treatment for people with post-stroke aphasia. The best electrode placement for people with aphasia is a topic of discussion. This study describes a protocol to compare 2 electrode placements within 13 individuals with post-stroke aphasia and discusses how to choose the optimal electrode placement for each individual. We conclude that, for a sub-group of patients, it was possible to choose an optimal electrode placement. In future studies it will be important to study the effectiveness of a chosen electrode placement, which requires multiple treatment sessions with brain-stimulation.
Accepted Mar 7, 2018; Epub ahead of print May 8, 2018
J Rehabil Med 2018; 50: 00–00
Correspondence address: W. Mieke E. van de Sandt-Koenderman, Rijndam Rehabilitation, PO Box 23181, NL-3001 KD, Rotterdam, The Netherlands. E-mail: msandt@rijndam.nl
Approximately one-third of stroke patients have aphasia, a language disorder typically caused by damage to left hemisphere (LH) regions (1). Multiple sessions of speech and language therapy (SLT) combined with transcranial direct current stimulation (tDCS) may enhance language functioning, compared with sham-tDCS (i.e. pseudo-stimulation) (2–8). With tDCS, 2 electrodes are placed on the outside of the head to apply a weak 1–2 mA current to the cortical areas (9–12). Anodal tDCS enhances neuronal excitability, while cathodal tDCS diminishes neuronal excitability. For treatment of aphasia, different electrode configurations have been used across studies (2, 4, 6, 13, 14). As LH activation is thought to be crucial for aphasia recovery (15, 16), most studies aim to promote LH activity by applying anodal tDCS over LH regions.
Studies mostly focus on 2 crucial language areas; the left inferior frontal gyrus (l-IFG) and the left posterior superior temporal gyrus (l-STG) (17, 18). Damage to the l-IFG is associated with non-fluent aphasia, which is characterized by non-fluent, sparse, dysprosodic, and agrammatic speech production (19). Damage to the posterior l-STG is associated with fluent aphasia, which is characterized by fluent speech with phonemic and semantic paraphasias (20). It has been reported that anodal tDCS over the l-IFG or l-STG improves language functioning, both in healthy speakers and in people with aphasia (PWA) (5, 6, 21–25).
Recent studies emphasize that the optimal electrode configuration may vary across PWA, due to factors such as severity/type of aphasia and lesion size (2, 26–28). For example, Baker et al. (2) hypothesized that frontal stimulation may be beneficial for people with frontal damage (non-fluent aphasia), while posterior stimulation may be beneficial for those with posterior damage (fluent aphasia). Interestingly, one within-subject study applied multiple tDCS sessions in patients with non-fluent aphasia and reported an advantage of anodal tDCS over the l-IFG, compared with anodal tDCS over the l-STG and sham (6).
In order to take into account individual variability, some studies determine an optimal electrode configuration per individual before starting with multiple tDCS sessions. Two studies used neuroimaging to guide individualized electrode placement (2, 4) and, although this may be a useful method, it is also relatively expensive, time-consuming, and not applicable to all patients. Another approach is to use behavioural measures (27, 29), which would be more feasible in day-to-day clinical practice. For example, Shah-Basak et al. (27) compared the effect of different electrode configurations within participants in single therapy sessions; improvement on naming untrained items was the outcome measure and the results showed that participants vary in their response to different electrode configurations. It is therefore suggested to develop a single-session protocol to determine an optimal configuration before starting multiple sessions of tDCS.
The aim of the present study is to evaluate such a protocol to compare anodal tDCS over the l-IFG with anodal tDCS over the l-STG in patients with chronic aphasia. The 2 outcome measures are naming performance on both trained and untrained picture items. Interpersonal variability in response to l-IFG vs l-STG stimulation is related to the aphasia type (i.e. non-fluent vs fluent aphasia).
In a double-blind randomized cross-over design, participants were assigned to a sequence of 3 therapy sessions. In each session, a 30-min word-finding therapy was combined with 1 of 3 tDCS conditions. In the first session, all participants received sham-tDCS (i.e. pseudo-stimulation) to get used to the tDCS equipment and treatment protocol, and to study potential placebo effects. In the second and third sessions participants received anodal tDCS over the l-IFG or the l-STG (randomized over sessions 2 and 3). All 3 therapy sessions were completed in 2–4 weeks, with a minimum interval of 3 days between sessions. For this study design with 3 repeated measurements, an alpha of 0.05, power of 0.80, an estimated Cohen’s f medium effect size of 0.35, and an estimated within-patient correlation of 0.70, a total sample size of 12 participants was needed. To account for potential drop-outs during the study we aimed to include a total of 14 participants. This study was approved by the Medical Ethics Committee of Erasmus University Medical Center Rotterdam.
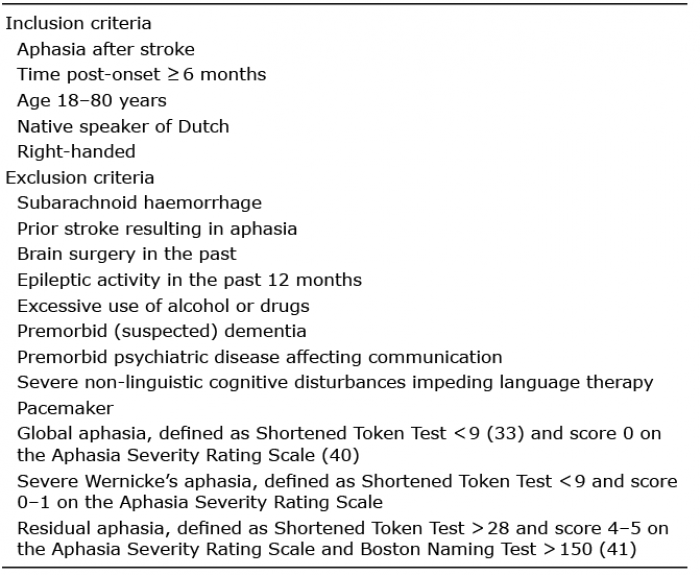
Participants were recruited at Rijndam Rehabilitation between February and December 2016. They were either enrolled in, or had completed, their stroke rehabilitation programme. Additional participants were recruited through a Dutch website for therapists and PWA (www.afasienet.com). The inclusion and exclusion criteria are shown in Table I.
Table I. Inclusion and exclusion criteria
The DC Stimulator PLUS (Eldith, MedCat B.V., Klazienaveen, The Netherlands) was used in the authorized form. This device is certified as a medical device, class IIa, by the European Union Notified Body 0118 (CE 118). Before starting the 30-min word-finding therapy, 2 electrodes (5 × 7 cm) were placed on the subject’s head, using elastic tape. Electrode placement was guided by the international 10-10 electroencephalogram (EEG) system: the F5 EEG position was used for the l-IFG configuration (30) and the CP5 EEG position for the l-STG configuration (31). The device was pre-programmed (with a unique 5-number code per participant and per session) for either sham or active stimulation (1 mA). Thus, both the patient and the speech and language therapist (SLT; in training) were blinded for the stimulation condition.
In the first session, all patients received sham-tDCS, i.e. pseudo-stimulation. The anode was placed over the l-IFG or the l-STG (the order was randomized across participants). In this condition, stimulation was automatically activated with a fade in of 15 s and, after 30 s, the stimulation was deactivated with a fade out of 15 s. In sessions 2 and 3, patients received active tDCS; the sequence of electrode placement was randomized, with the anode either placed over the l-IFG or the l-STG. The stimulation was automatically activated with a fade in of 15 s, and deactivated after 20 min with a fade out of 15 s. In all 3 conditions, the cathode was placed over the contralateral supra-orbital region (EEG position: Fp2).
A baseline assessment was performed before inclusion to assess handedness with the Edinburgh Handedness Inventory (EHI) (32), severity of aphasia with the Short Form of the Token Test (STT) (33), and spontaneous speech with the Aphasia Severity Rating Scale (ASRS) (34). The baseline assessment was followed by the first of 3 therapy sessions (A, B, C). In each treatment session, 2 picture-naming tasks were used, the first to select training items per individual (tasks A1, B1, C1), and a second task to evaluate generalization to untrained items (tasks A2, B2, C2). In total, 6 tasks were used, matched for word length and word frequency. Each task comprised 30 pictures depicting nouns selected from the European Data Bank (35).
All pictures were shown on a computer screen for 5 s, followed by a blank slide for 3 s (using PowerPoint) and responses were audio-recorded. A response was scored as correct when the participant was able to produce the target word (or a synonym) within 5 s, otherwise it was scored as incorrect. The first 10 incorrect responses from A1, B1 and C1 respectively, were selected for treatment, and this “therapy set” was trained during the 30-min aphasia therapy combined with 1 of the 3 tDCS conditions. In case participants named fewer than 10 items incorrectly, items from an extra set were used to complete the therapy set. For the therapy, the SLT was trained to use cueing techniques to help the participant to correctly retrieve and produce the target word (36). The cue of the lowest stimulus power was shown first, followed by increasingly powerful cues until the correct word was retrieved and produced. Details of the therapy are published elsewhere (37). At the end of each session, the therapy set was administered (without help). The 30 pictures of the second naming task (A2, B2, C2) were shown before and after each therapy session, and results were used to study the treatment effect on untrained material. Fig. 1 presents an overview of the sessions and tasks. Finally, to assess discomfort, participants were asked to complete a Wong-Baker Faces Pain Rating scale (WB scale) after each session (38). This is a visual analogue scale ranging from 0–5, developed for individuals with limited verbal skills
Fig. 1. An overview of the 3 sessions and tasks.
All naming tasks were scored offline by a trained test assistant, who was blinded for the tDCS condition. For the untrained items, the test assistant was also blinded for pre-treatment vs post-treatment assessments. For the trained items, this was not possible because performance was only tested post-treatment; per definition, before therapy, the percentage correct was 0%. In general, a response was scored as correct when the participant was able to produce the target word or synonym within 5 s. A pre-set list was made with synonyms, i.e. correct alternatives for the target word. In case the participant produced a synonym that was not listed as a correct alternative, the test assistant and research coordinator discussed whether it should be considered correct. If agreement could not be reached, half a point was given for the produced item. An experienced clinical linguist (WS-K) assessed the ASRS samples and classified participants’ aphasia as fluent or non-fluent.
The main outcome measure was the proportion of correct responses on the therapy set (10 items) after therapy, across the 3 conditions: sham, l-IFG and l-STG. The secondary outcome measure was the improvement on untrained items (30 items), across the 3 conditions. Per condition, the delta score was calculated, defined as the proportion of correct responses post-treatment minus the proportion of correct responses pre-treatment.
To determine an optimal configuration per individual, individual response patterns across conditions were analysed. For the trained items, we considered a proportional improvement of 20% between conditions as relevant, in line with a previous study comparing the same 3 tDCS conditions and using naming performance as an outcome (25). Specifically, we considered the condition in which the performance was 20% higher than in the other 2 conditions as the optimal configuration for an individual. The same method was used for the untrained items, but here we used a smaller proportional difference of 10%, since there is generally less improvement on untrained items.
In addition, we investigated whether, at the group level, the 2 configurations of interest yielded different results of naming performance after a single therapy session. Thus, we compared proportions of improvement across conditions, also taking into account the order in which the montages were applied. Given the nature of our outcome data (proportions of counts), data were analysed with the semiparametric generalized estimation equation (GEE) analysis, which takes into account that multiple measurements within patients are correlated. To study the effect of condition (sham, l-IFG, l-STG), measurement time (session 1–3) and configuration order (starting with l-IFG or l-STG in session 2), these variables were entered as fixed factors into the model, in which either the post-treatment scores of the trained items or the delta scores of the untrained items was the dependent variable. If a factor had a significant effect on the outcome, post-hoc pairwise comparisons were performed to specify the significant differences within each factor. Finally, patient discomfort rating, assessed with the WB scale, was tested using a Mann–Whitney U test. The level of significance (p) was 0.05 in all analyses. IBM SPSS 21 Statistics software was used for all statistical tests.
Fourteen participants were included in the study, but data were collected from only 13 participants.
One participant was excluded after the first session because the therapist considered the therapy to be too intensive for the participant. Thirteen participants completed the 3 therapy sessions. The mean interval between sessions was 6 (standard deviation (SD) 2.9) days (between session 1 and 2, mean 5.3 days, SD 1.8 days; between session 2 and 3, mean 6.7 days, SD 3.7 days).
No side-effects were observed. All participants tolerated the treatment well; however, some participants reported that the treatment sessions were rather intensive. Overall, discomfort ratings were low and ranged from 0 to 1, with median scores of 0 for each session (interquartile range (IQR) session 1: 0–0, session 2: 0–0, session 3: 0–0.75). Discomfort ratings were comparable across sessions; Mann–Whitney U (Friedman: χ2(2) = 1, p = 0.607).
Thirteen participants were recruited (10 men; mean age 53.15 years (SD 10.90)). All participants were right-handed (EHI > 0.50; mean 0.96 (SD 0.12)) and at least 6 months post-stroke (MPO; mean 48.92 months (SD 48.43)). Demographic and clinical characteristics of each participant are shown in Table II.
Table II. Demographic information and clinical data of the participants
Table III presents the post-treatment and delta scores for trained and untrained items respectively, per individual (see Table SI1 with the pre- and post-scores for trained and untrained items).
Table III. Delta scores (%) on trained and untrained items per individual
Trained items. For almost one-third of participants (P1, P2, P6, P12, P13), the therapy set had to be complemented with items from an extra set to ensure that the therapy set included 10 items in each session. For 4 participants (P1, P7, P9, P11) the improvement in the l-IFG condition was larger than in the other conditions. Two participants showed the same improvement in the l-IFG and l-STG condition (P8, P13) and this improvement was larger than in the sham condition. For 7 participants, because no relevant differences were found between the conditions, no optimal configuration could be determined.
Untrained items. Three participants showed lower performance after treatment; specifically, P3 in the l-IFG and l-STG condition, P7 in the l-STG condition, and P10 in the sham condition. For the remaining 10 participants, no relevant differences were found in improvement between conditions.
Trained items. Overall, post-treatment performance on trained items ranged from 0% to 100% correct responses, with a median of 50% (IQR: 20–85). Fig. 2A shows the median and interquartile ranges (IQR) for each condition, with 50% (IQR: 20–80) correct in the sham condition, 70% (IQR: 30–95) correct in the l-IFG condition, and 50% (IQR: 20–82.5) correct in the l-STG condition. GEE analysis revealed an effect of condition, such that the post-treatment score in the l-IFG condition was significantly higher than that in the other 2 conditions (p = 0.040). There was no effect of measurement time (p = 0.943) and configuration order (p = 0.669).
Fig. 2. Results of the proportion correctly named items for the sham condition, the inferior frontal gyrus (IFG) condition and the superior temporal gyrus (STG) condition. (A) Results for the post-treatment results for the trained items. (B) Delta scores for the untrained items.
Untrained items. Overall, the delta scores for the untrained items ranged from –23.3% to 13.3%, with a median of 0% correct responses, reflecting no improvement (IQR: –3.4–3.3). Fig. 2B shows the median and IQR for each condition, with 3.3% (IQR: 0–6.7) correct in the sham condition, 0% correct in the l-IFG condition (IQR: –4.95–1.65), and 0% correct in the l-STG condition (IQR: –6.7–0). GEE analysis revealed no significant effect of condition (p = 0.820), measurement time (p = 0.404) and configuration order (p = 0.382). Pairwise comparisons revealed that the delta scores in sessions 1 and 3 were significantly different (p = 0.044), with a larger delta score in the first session.
The aim of this study was to evaluate a tDCS protocol, comparing different configurations within individuals and using behavioural language measures to guide optimal electrode placement. This is the first study to include both trained and untrained picture items as outcome measures in a protocol aimed to determine an optimal configuration in a single session.
At the group level, there was a better post-treatment performance on trained items in the l-IFG condition compared with the other conditions. In line with our expectations, there was considerable variability in the individual response patterns. Almost half of the group responded more to the l-IFG condition or both active conditions; the other half showed equal performance across conditions, therefore it was not possible to determine an optimal configuration for these participants. In contrast to the trained items, there was no improvement on untrained items, indicating that one word-finding therapy session did not generalize to naming untrained items. Individual response patterns showed variable results and there were no conditions in which the improvement was relevantly larger than in the other conditions. Instead, 3 participants showed a lower performance after treatment. Therefore, interestingly, our protocol to determine an optimal configuration had a differential effect for trained and untrained items. However, performance on trained items may have been more suitable to detect improvements in the present study, as the trained items constituted an individualized set of material, tailored to the individual’s performance level.
The group results of the trained items revealing enhanced performance in the l-IFG condition are in line with other studies showing an effect of anodal tDCS over the l-IFG (5, 6, 21). Moreover, Marangolo et al. (5) reported an advantage of anodal tDCS over the l-IFG, compared with anodal tDCS over the l-STG and sham. However, their design differed from that of the present study in both type and duration of treatment: i.e. Marangolo et al. (5) combined tDCS with a 10-day conversational therapy treatment aiming to improve spontaneous speech in multiple sessions, whereas the present study aimed to determine an optimal electrode configuration in single sessions before starting with multiple tDCS sessions.
The lack of generalization to untrained material is in contrast with the results of Shah-basak et al. (27). These authors compared the effect of different electrode configurations within participants in single therapy sessions. Improvement in untrained naming performance on an 80-item picture naming task was used as an outcome measure. The authors found significant improvement on untrained items and concluded that these results could be used to determine an optimal electrode configuration for each patient. In the present study, we did not replicate such generalization to untrained items. In general, it can be assumed that there is less improvement on untrained items compared with trained items (2, 14) and generalization to untrained items may be difficult to achieve after a single therapy session. For example, although Meinzer et al. (14) found no significant differences in performance on untrained items immediately after 1 treatment session, significant effects emerged during the follow-up assessments, after multiple sessions.
The differences in results between the study of Shah-Basak et al. (27) and the present study may be related to the differences in aphasia severity between the study samples. For example, the study sample of Shah-Basak et al. (27) may have had less severe aphasia and would therefore respond better to treatment. Another possible explanation is that our naming task contained 30 items, whereas that of Shah-Basak et al. (27) contained 80 items; a larger set of items will be more sensitive to improvement. It was interesting to note in our study that both the pre- and post-scores improved over time and the delta scores decreased across sessions, suggesting that, over time, there was less room for improvement. Some participants had high baseline scores in the first session, for both trained and untrained items, implying less room for improvement.
Individual analysis of the trained items revealed that 6 participants showed a relevantly larger improvement in the active conditions compared with the sham condition. Two of these participants, both with fluent aphasia, showed the same improvement in the l-IFG and l-STG condition; therefore, based on our protocol, it would not matter what configuration is used. For 4 participants, the electrode configuration did play a role, such that these participants had a relevantly larger score in the l-IFG condition; interestingly, 3 of these latter patients were diagnosed with non-fluent aphasia. In the study of Baker et al. (2) 4 of 12 patients responded to anodal tDCS over the frontal cortex. These patients had apraxia of speech and/or non-fluent aphasia, both of which are associated with left frontal damage. Therefore, the authors hypothesized that frontal stimulation may be beneficial for people with frontal damage (non-fluent aphasia) (2). Our findings support this idea, since we observed that 3 patients with non-fluent aphasia performed better on the trained items during the l-IFG configuration. However, our study does not support the idea that people with fluent aphasia respond more to posterior stimulation, at least not in a single session. For 7 participants, there were no relevant differences across conditions; for these individuals, our protocol did not provide a basis for choosing an optimal electrode configuration. The same applies to the study group of Shah-Basak et al. (27), in which 5 of 12 patients did not respond better to any specific configuration.
The present study has some limitations. First, no information on lesions was available for our participants, whereas lesion size/site are considered important factors in aphasia recovery and (probably) also important in determining an optimal configuration. Another limitation is the small sample size. Furthermore, some participants reported that they found the sessions rather intensive. As the naming task to measure improvement on the untrained items was always assessed at the end of each session, we cannot exclude the possibility that participants became tired/less attentive at the end of the sessions and across sessions. Therefore, we recommend that studies using within-subject designs to study the effect of tDCS take into account the factor of time and other possible effects, such as fatigue and/or attention. Finally, we have compared 2 configurations, anodal tDCS over the left-IFG with anodal tDCS over the left-STG, while several other electrode configurations have been described in the literature, such as inhibition of right hemisphere areas (13), simultaneous facilitation of left hemisphere areas and inhibition of right hemisphere areas (bihemispheric tDCS) (39) and facilitating language areas through motor area stimulation (14). For future studies it will be important to compare different electrode configurations and to evaluate how we can choose an optimal electrode configuration in aphasia treatment.
In conclusion, our protocol to determine an optimal configuration showed a differential effect for trained and untrained items, such that we could only use performance on trained items as guidance for configuration. For some participants, it was possible to determine an optimal configuration after comparing single therapy sessions. It would be interesting to verify our protocol in future samples to elucidate which patient profiles allow us to determine an optimal configuration after a single session. It is important to note that our single session protocol is limited, such that we cannot test the effectiveness of a selected optimal configuration as we have only used single tDCS sessions. Therefore, future studies may also study the effectiveness of the selected configuration, which requires multiple therapy sessions.
The authors thank Dunja Allal El Bakhti and Linda Boekee-Hordijk for their help in the test assessments.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize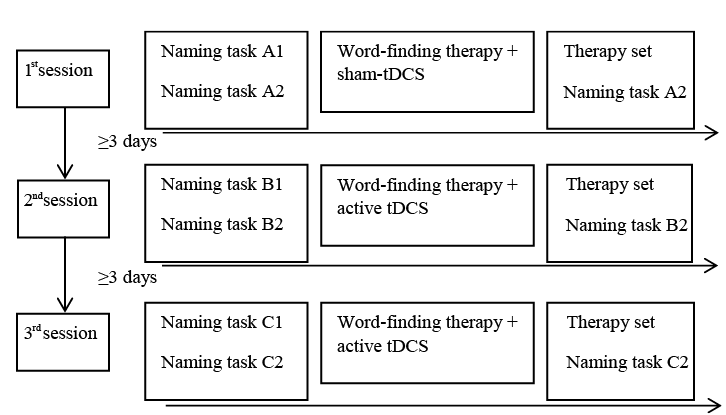 Click to show fullsize
Click to show fullsize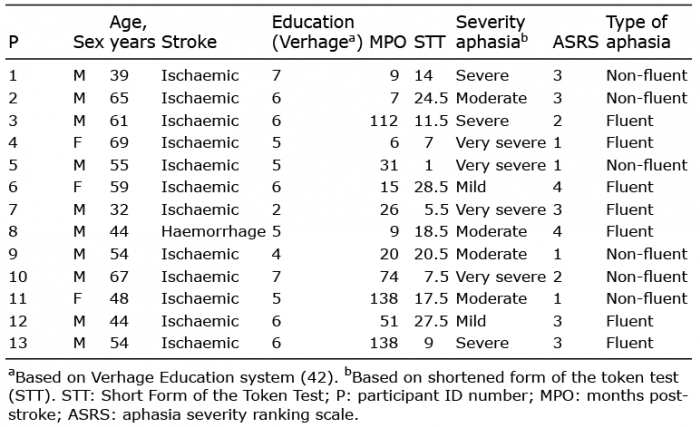 Click to show fullsize
Click to show fullsize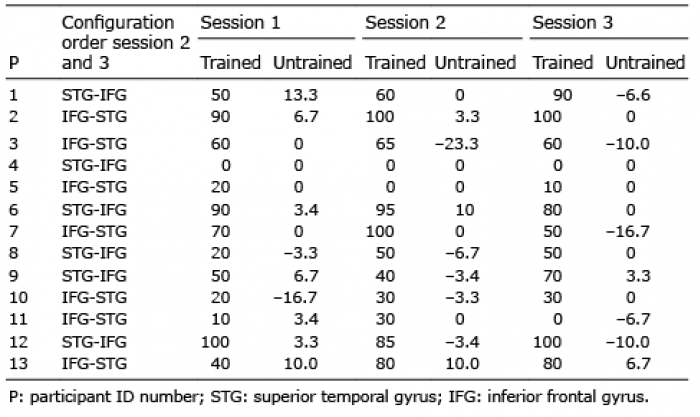 Click to show fullsize
Click to show fullsize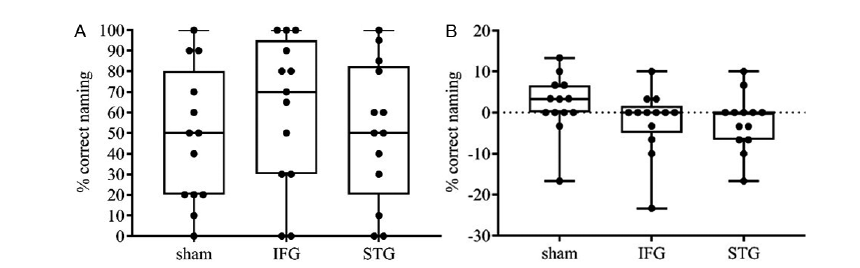 Click to show fullsize
Click to show fullsize