
From the 1Roessingh Research and Development, 2Department of Biomechanical Engineering, 3Department of Biosystems and Signals, University of Twente, Enschede, the Netherlands, 4Cereneo AG, Vitznau, Switzerland, and 5Departement of Physical Medicine and Rehabilitation, Northwestern University, Chicago, IL, USA
Objective: To investigate the feasibility of a wear-able, soft-robotic glove system developed to combine assistive support in daily life with performing therapeutic exercises on a computer at home (the HandinMind system).
Design: Feasibility study.
Patients: Five chronic stroke patients with limitations in activities of daily living due to impaired hand function.
Methods: Participants performed a usability test and several functional tasks with the HandinMind system across 2 sessions. Feasibility was measured using the System Usability Scale (SUS), Intrinsic Motivation Inventory (IMI) and performance times of the functional tasks.
Results: User acceptance measured by the SUS and IMI was scored high. The median SUS scores of sessions 1 and 2 were 80.0 (interquartile range (IQR) 70.0–88.8) and 77.5 (IQR 75.0–87.5), respectively, and the median IMI score was 6.3 points out of 7 points (IQR 6.2–6.3). Functional task performance was initially slower with the HandinMind glove compared with performance without the glove, but improved up to the level of performance without the glove across no more than 3 repetitions.
Conclusion: Chronic stroke patients with impaired hand function were positive about the feasibility of the first prototype of the HandinMind system. How-ever, performance and ease of use of the system should be improved further in future development phases.
Key words: soft-robotic glove; assistive technology; robot-assisted rehabilitation; wearable devices; activities of daily living; upper limb; stroke.
Accepted Apr 19, 2018; Epub ahead of print Jul 2, 2018
J Rehabil Med 2018; 50: 598–606
Correspondence address: Bob Radder, Roessingh Research and Development, Roessinghsbleekweg 33b, PO Box 310, 7500 AH Enschede, The Netherlands. E-mail: b.radder@rrd.nl
This study investigated the feasibility of a first prototype of a wearable, soft-robotic glove system (HandinMind) developed to combine assistive support in daily life with performing therapeutic exercises on a computer at home. This system was tested by 5 chronic stroke patients with limitations in activities of daily living due to impaired hand function. Although the subjects identified several usability issues, they showed high scores on usability for this first prototype of the HandinMind system. Furthermore, they initially performed functional tasks slower with the HandinMind glove compared with without the glove, but performance improved up to the level of performance without the glove across no more than 3 repetitions. With further improvements, this system may enable intensive functional hand training for stroke patients without the need for supervision by a therapist.
Worldwide, stroke, or cerebrovascular accident (CVA), remains a leading cause of permanent disability (1). For optimal restoration of upper limb motor function after stroke, therapy should consist of several key elements: repetitive, high-intensive, task-specific and functional exercises with active contribution from the patient (2–4). Providing such highly intensive therapy in a conventional rehabilitation setting predominantly involves close supervision of a therapist for each patient, which makes it labour-intensive and expensive (5, 6). This will be an even greater problem when the incidence of stroke patients rises further in the coming decades, as is expected due to the ageing population (1). Therefore, the number of new technological innovations that can be used to facilitate exercise programmes fulfilling the key elements of therapy is increasing rapidly, of which robotic devices and therapeutic exercises in the form of games are well-known examples (7–9).
Although more conclusive evidence is needed,
robotic devices aimed at training have shown effects on upper limb motor function, but limited improvements in performance of daily activities (5, 10–12). These devices have initially focused predominantly on the proximal upper limb, while the hand also plays an important role in performing daily activities. Therefore, hand training should also be part of the rehabilitation programme to improve functional performance (3). Moreover, the review of Balasubramanian et al. (7) showed that distal robotic training has a generalization effect on motor improvements of the entire arm.
Although robotic training devices can improve motor function and performance to a certain extent, a larger effect is expected when therapy could be applied with a higher frequency and/or duration than is currently possible in many conventional rehabilitation settings (13, 14). This would require (partly) self-administered training by stroke patients, ideally at a person’s home when the device is suitable for home deployment (15). More pronounced effects on activity level are expected when functional, task-specific exercises are implemented in robotic therapy, by including functional exercises for the hand (16).
The latest technological innovations concerning soft-robotics allow robotic devices to become wearable and less obtrusive to use in daily life (17–19). This enables an entirely new paradigm for stroke rehabilitation, in which intensive use of the arms and hands in functional exercises become entwined, via assistive support of the impaired hand during daily activities at home. In addition, the assistive support of the impaired hand during daily activities could be combined with performing therapeutic game-like exercises on a computer.
In the HandinMind (HiM) project, such a wearable dual-function system (the soft-robotic HiM glove), is being developed. Since this system is part of an iterative development process, a user-centred approach is used to increase the chances for uptake of such devices in daily life (20, 21). Therefore, the aim of this initial stage of user tests is to obtain a first insight in feasibility of the first prototype of the HiM system. Thus, this study investigated user acceptance (e.g. perceived ease of use, motivation, system usability) and impact of the HiM system during the performance of activities of daily living (ADL).
For this feasibility study, 5 chronic stroke patients with self-perceived hand function impairments resulting in problems executing ADL were recruited through the rehabilitation physician of Roessingh Centre for Rehabilitation (Enschede, the Netherlands). Additional inclusion criteria included age between 18–80 years, > 6 months post-stroke, at least 10° of active flexion and extension of the fingers to produce the interaction force that is needed to control the assisted support of the glove, don/doff the glove by themselves (closing the zip of the glove was not necessary for completion of don/doff), living at home, sufficient cognitive status to understand 2-step instructions and (corrected to) normal vision. Exclusion criteria included severe sensory problems, acute pain, spasticity and contractures of the affected hand or co-morbidities that may limited hand function and functional use in ADL, wounds on the affected hand that could lead to problems with wearing the glove, participation in other studies that could affect functional performance of the affected upper limb and having insufficient knowledge of the Dutch language to understand the purpose or methods of the study. The rehabilitation physician, who was familiar with the HiM system, judged whether the potential participant was suitable for participation on the basis of the criteria.
All participants were informed verbally and in writing about the purpose and procedures of the study and signed a written informed consent before inclusion. This study was approved by the Medical Ethics Committee Twente, Enschede, the Netherlands (registration number: NL51270.44.14).
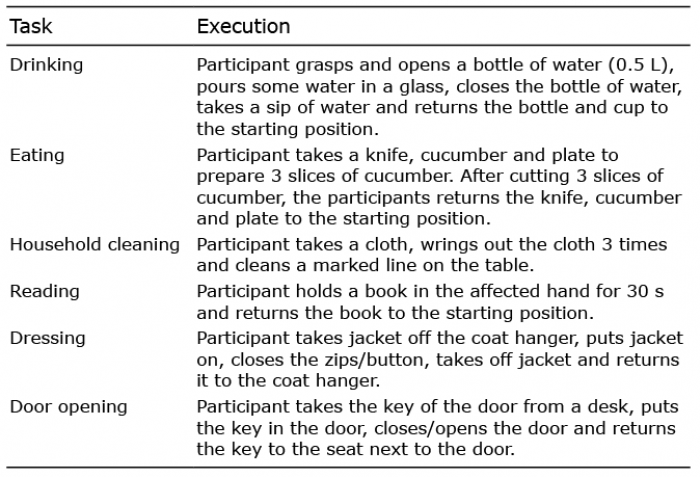
In this cross-sectional feasibility study, participants performed various ADL-like tasks (Table I), 3 times with, and once with-out, the HiM system prototype during 2 sessions on 2 separate days (with a minimum of 4 days between sessions). During the performance of these different tasks, participants were encouraged to think aloud (22). The experiment took place in a controlled laboratory environment at Roessingh Research and Development (RRD), Enschede, the Netherlands. The order of the conditions (with or without HiM system) applied during each session was randomized by a trained clinical researcher using sealed envelopes. Using the HiM system for the first time (naïve use) was tested in evaluation session 1 and exposed use was tested in evaluation session 2. All sessions were supervised by the same clinical researcher (human movement scientist), who had experience with performing these tests.
Table I. Explanation of task execution
The first HiM system prototype consists of a wearable soft-robotic glove that was developed to support grip and hand opening of all fingers of stroke patients in a wide range of ADL (HiM assistive system). The same glove can be connected to a computer with specific software to provide a specific training context to train hand function (HiM therapeutic system) (Fig. 1).
Fig. 1. The HandinMind system. Left: the HandinMind assistive system. Right: the HandinMind therapeutic system.
The HiM assistive system consists of 2 parts: (i) the control unit; and (ii) the glove. The control unit houses the actuators, control software and batteries, which allows a use period of multiple hours.
The extra grip strength is regulated by a tendon-driven
mechanism that is controlled by sensor input from force sensors (technology from Tekscan Inc., South-Boston, Massachusetts, USA) at the fingertips and extension/flex sensors (Flexpoint, Draper, USA) along the dorsal side of the fingers. This prototype uses an intention detection logic that activates the grip support after the participant initiates contact with an object, detected through the force sensors, and is intended to provide support in a fast, natural and intuitive way. The tendon actuators provide support in proportion to the grip force applied by the participant, with more support supplied when a stronger grip is applied on the object. Grip force is released when the participants release the object and the force sensors detect a reduction of force. In addition, hand opening is supported by passive leaf springs attached to the dorsal side of each finger.
The HiM therapeutic system comprises of: (i) a therapeutic platform (e.g. computer) to which the HiM assistive system is connected; and (ii) therapeutic software including exercises, assessments, patient databases, connectivity features, additional safety mechanisms and a user interface for the patient and therapist (see Fig. 1).
The HiM therapeutic system supports the following therapy goals:
A usability test was performed at the start of session 1 only, to obtain insight into the perceived ease of use of the HiM system prototype upon first, naïve use. The test involved donning/
doffing the HiM assistive system, performing a drinking task with the assistive glove and performing a few assignments using the HiM therapeutic system (e.g. start training software, perform calibration, select 3 game exercises, play exercises for 2 min, etc.). Participants received no instructions about how to use the HiM system prototype before or during the usability test. This was done to test the intuitiveness of the glove and training software, in order to gather feedback about how to design the next versions of the HiM system. The researcher closely observed the actions and registered the comments of the participant during the test to identify areas that need improvements.
A functional task performance test was part of both sessions and performed after the usability test in session 1. Prior to this test, participants received instructions about how to use the HiM system prototype properly. Subsequently, the level of hand opening support and the amount of grip support (in terms of sensitivity and maximal gain) was tuned for each individual participant based on the participants’ needs and experienced comfort (until support from the glove was experienced). Participants then used the wearable soft-robotic glove during 6 different functional tasks: drinking, eating, household cleaning, reading, dressing and door opening (for more details about task execution, see Table I). The most-affected hand was used as the primary hand to perform all functional tasks, irrespective of hand dominance. All functional tasks were demonstrated by the researcher before the test started. Furthermore, participants received verbal instructions about how to execute the functional tasks during the test, if needed.
Fugl-Meyer assessment. Motor function of the arm and hand was measured with the upper extremity part of the Fugl-Meyer assessment (FM). The maximal score on the FM was 66 points (23).
Usability test. The usability test was video-recorded after consent from all participants and the main findings were noted by the researcher. The findings of the full observational analysis have been grouped by the clinical researcher, first to a grouping structure, defined by the overall categories elicited by the
patient responses concerning use issues, and sub-divided among specific topics of information, where needed. Subsequently, the common denominators have been extracted across all usability tests by analysing the number of participants that have indicated a particular issue.
Functional task performance test. The performance time of
all functional tasks was measured from the start position (lifting hand from table) until completion of the task by using a stopwatch. In addition, the researcher observed and noted striking qualitative aspects of task execution (e.g. remarkable (differences in) speed of movement or fluidity of movement) as a potential sign of issues.
Of the 3 repetitions with the glove, the first 2 were dedicated to getting used to the glove, and only the last repetition was used to compare the performance times between both conditions. Change in performance times over the 3 consecutive repetitions with the glove were used to explore a potential learning effect.
User acceptance. User acceptance of the HiM system in terms of usability and motivation when using the system was measured by the System Usability Scale (SUS) and the Intrinsic Motivation Inventory (IMI), respectively. The English versions of the SUS and IMI were already translated into Dutch, and although the translated versions were not validated, they were also used in other studies, e.g. Nijenhuis et al. (24).
The SUS is a 10-item questionnaire assessing the subjective experiences of usability of a technological system. Each item was scored on a scale ranging from ”(1) strongly disagree” to ”(5) strongly agree”. The total score of the SUS was translated to a score ranging from 0–100, where higher scores indicate better usability. A score < 50 indicates a low probability of acceptance in the field, 50–70 is a promising score, but does not guarantee high acceptance in the field, and a score > 70 indicates a high probability of acceptance in the field (25, 26). The SUS was administered in both sessions, after the functional performance tests.
The IMI is a 34-item questionnaire consisting of 6 different domains (interest/enjoyment‚ perceived competence‚ effort‚ perceived choice while performing a given activity, experienced pressure/tension and value/usefulness), assessing an individual’s intrinsic motivation during a physical activity, in this case performing functional tasks with support from the HiM system. Each item was scored on a scale ranging from “(1) not at all true” to “(7) very true” (27–29). A higher score on the IMI indicates a higher motivation during the use of the HiM system. The IMI was administered at the end of session 2 only.
Statistical analyses were performed using IBM’s SPSS Statistics software package, version 23.0. Descriptive statistics were used to describe patient characteristics and all outcome measures. In addition, the Friedman test was used to test the differences in performance times between consecutive repetitions of the functional tasks with the glove within both sessions. The overall level of significance was set at α ≤ 0.05.
The characteristics of the 5 chronic stroke patients at baseline are shown in Table II. No adverse events were observed during any of the tests with the HiM system.
Table II. Characteristics of the participants
All participants were able to don and doff the first version of the HiM assistive system by themselves. However, closing the zips of the glove was not possible for all participants. Performance of the drinking task with the HiM assistive system was completed successfully without instructions by 3 participants, the other 2 participants needed help due to their impaired hand function. Nevertheless, some aspects of using the HiM assistive system prototype in this functional task were
observed to be difficult for most participants (Fig. 2). This was related predominantly to less sensation, which was experienced and reported by all participants, while performing the task with the glove due to the thickness of the fabric of the glove.
Fig. 2. Difficulties with the drinking task.
Participants also experienced some usability issues while using the first version of the HiM therapeutic system when no instructions were given, especially regarding selecting and playing the various therapeutic exercises (Fig. 3).
Fig. 3. Difficulties with the therapeutic exercises.
Three attempts with the glove (second attempt door opening task of participant 2 during session 1, second attempt reading task of participant 3 during session 1, and third attempt household cleaning task of participant 5 during session 2) were not included in the analysis, because these tasks were not performed according to the given instructions. Furthermore, participant 5 was not able to perform the reading task, because of insufficient arm strength to lift the book. All individual performance times for each task are shown in Fig. 4.
Fig. 4. Individual performance times of all tasks. (A) First repetition with glove, (B) second repetition with glove, (C) third repetition with glove, and (D) without glove.
The individual performance times of the participants (Fig. 4) showed improved performance during the 3 consecutive repetitions with glove (a learning curve in performance), during both sessions. However, the learning curve in sessions 1 seemed larger compared with the learning curve in session 2. There are a few trials in particular in the eating and door opening tasks that interrupt the learning curve in performance for some participants. Additional statistical analysis showed that for the drinking and household cleaning tasks in both sessions (p ≤ 0.039), and the eating task (p = 0.019) and door opening task (p = 0.005) in session 1, performance times differed between the 3 consecutive repetitions with the glove. For these tasks, individual participants showed an overall reduction in performance time between the first and third repetitions of 9.4–42.4 s in the drinking task, 5.0–23.5 s in the eating task, 0.3–8.9 s in the household cleaning task, 4.1–15.6 s in the door opening task of session 1. In session 2, they improved performance in the drinking task with 1.4–22.6 s and in the household cleaning task with 0.7–4.7 s.
When we are looking at the performance times of the final repetition with glove and without glove (Fig. 4), we do not see a clear difference in performance times between with and without glove for all tasks in favour of performance with glove or without glove, in either session. Overall, median changes showed a small difference between performance with and without glove ranging from –1.1 to 2.5 s, except for the drinking task in session 1 (median difference of 5.8 (IQR 0.6–16.0) s), door opening task in session 1 (median difference of 5.4 (IQR 3.6–18.9) s) and the drinking task in session 2 (median difference of 4.1 (IQR –7.9 to 12.0) s), in favour of performance without glove.
Qualitative observations during the functional performance test highlighted that all participants experienced difficulties with performing fine motoric subtasks (e.g. grasp cap of the bottle from table, grasp cap of bottle during opening/closing the bottle) when wearing the glove. Participants mentioned that they experienced these difficulties with fine motoric tasks due to perceived decreased sensation with the glove. On the other hand, all participants mentioned that they mainly noticed and appreciated the grip support of the glove during gross motor activities, such as holding the bottle, turning the cap of the bottle during opening/closing the bottle, cutting food, wringing the cloth and gripping the key during turning. They also perceived an improved performance with the glove across consecutive repetitions in terms of improved performance time and ease of use. In addition, the dressing task was too difficult to perform for all participants with glove, because the first prototype of the HiM assistive system was too bulky to wear underneath a jacket. Another usability issue observed by 3 participants was an unpleasantly warm and sweaty hand while using the glove.
All 5 participants completed the SUS after both sessions (see Fig. 5 for individual scores). The lowest SUS score was 65. The median of the SUS of session 1 was 80.0 (IQR 70.0–88.8) and the median of the SUS of session 2 was 77.5 (IQR 75.0–87.5), which was comparable (Fig. 5).
Fig. 5. Individual System Usability Scale scores.
Each part of the IMI was rated very positively by all participants, with a sub-score of at least 4.8 points per domain (Fig. 6). The IMI total score varied between 6.1 and 6.3 points, with a median IMI score of 6.3 (IQR 6.2–6.3).
Fig. 6. Individual Intrinsic Motivation Inventory (IMI) scores for each subscale.
The results of this study showed that the usability of this first HiM system prototype upon first and second use was acceptable and promising, as reflected in SUS scores of 80 and 77.5 (25). In addition, all participants were able to don/doff the glove by themselves, except for closing the zips of the glove. Furthermore, 3 participants were able to complete a functional drinking task with support from the HiM system without any assistance or instructions. Nevertheless, several usability issues were identified, especially concerning difficulties with performing the therapeutic exercises with the HiM system, performing the dressing task due to the bulkiness of the system, opening/closing the bottle with the glove and grasping the cap from the table with the glove without any assistance or
instructions. These issues need improvements in future iterations of glove development. Regarding functional performance, performance with the glove was initially slower than without the glove, but performance times with the glove improved across no more than 3 repetitions to levels close to or even up to the level of performance without the glove. This was even more pronounced during session 2. Overall, participants were motivated to use the HiM system and reported improved performance with the glove, although this was not always reflected in the outcomes as quantified via performance times.
Concerning feasibility of the HiM system, participants were positive about its usability and very motivated to use it, as reflected in the high individual SUS and IMI scores. The individual SUS scores of both sessions, ranging from 65 to 95, showed high probability of
acceptance of the HiM system for using the device for upper limb rehabilitation and assistance in daily life (25). Other studies (24, 30, 31) that investigated usability of other types of technology for the upper limb, such as (robotic) assistance or training programmes, showed lower scores (< 70) on usability indicating promise, but not guaranteeing high acceptance in the field. In addition, the median IMI score of 6.3, with at least a 4.8 on each subscale (Fig. 6), indicates that participants also regarded the HiM system as an interesting, useful and motivational system to use, aimed at improving their hand function during daily life. The studies from Nijenhuis et al. (32) and Radder et al. (31) showed lower overall IMI scores for stroke patients and elderly people using robotic hand devices for training purposes or assistance in daily life. Interestingly, the studies of Nijenhuis et al. (24, 32) showed that stroke patients were able to use a robotic training device, that received lower SUS and IMI scores, for the upper limb independently at home for at least 105 min a week. This may suggest that stroke patients might be able and motivated to integrate the HiM system into use in daily life. Moreover, the first HiM system prototype will be refined further based on the present usability findings, before it will be applied in a field test. This further enhances the probability of the HiM system to be applicable and usable in daily life.
The usability test of this feasibility study revealed some examples of experienced usability issues upon first use that need improvements for independent use of the HiM system at home. Our findings are in line with Demain et al. (33), who have suggested that barriers to assistive technology use are related to the simplicity of the design of assistive technology, such as difficulties with donning/doffing and initializing the device. Similar findings were observed when elderly subjects with age-related decline in hand function were asked about use of assistive technology to assist with ADL (34). When these issues are addressed in a proper way, potential users of assistive technology did consider
assistive devices as a home-based solution for intensive and functional upper limb rehabilitation, as well as for support during ADL. However, a prerequisite for using such a system is that it complies with user requirements (e.g. easy to operate, compact, simple to apply, portable etc.) for assistive technology (33–35). In addition, the system would be adopted only if the user perceives that the device enhances their functional performance and/or independence (35).
Regarding performance enhancement, there was no difference in functional task performance duration found between with and without glove performance in the majority of tasks. In our previous study (31), we observed that older adults with reduced hand function performed faster without the glove compared with with the glove during the same functional tasks as performed by stroke patients in the current study. The difference in influence of the glove on performance duration between both populations may be related to the severity of hand function problems. It is likely that participants with larger limitations in hand function can experience a larger gain when using the glove than participants with substantially less hand function limitations. This could be the case for people with limited hand function only, because the glove could not support insufficient arm strength (for example, holding a book). Stroke patients often experience a restricted range of motion, loss of sensory function or strength and increased muscle tone in their affected arm/hand causing severe motor loss and function (36), whereas elderly (possibly with rheumatoid arthritis or osteoarthritis) can experience decreased ability to perform daily activities due to reduced grip strength, sensory changes or pain (37). This results in that the glove would be less suitable for stroke patients with these severe impairments.
Concerning the amount of glove use, the HiM system was only used actively for approximately 20 min in both sessions to assess the feasibility of the HiM system. During these 20 min, participants showed large improvements in performance duration (median changes up to 38.8%) with the glove across only 3 consecutive repetitions, indicating a steep learning curve in both sessions. These learning curves showed that participants learned rather quickly how to make use of the glove after only 3 consecutive repetitions (see Fig. 4) (38). It is important to consider that more progression in performance with the glove is possible, because participants probably have not yet reached a learning curve plateau. Therefore, performance with the glove might become even faster compared with performance without the glove after a longer learning period with the glove.
Several limitations may have affected the interpretation of the results of this feasibility study. Firstly, the statistical analysis needs to be interpreted with extreme care, since these analyses involved a small sample of stroke patients (n = 5). Therefore, descriptive interpretations of the individual results of the stroke patients are also shown in this feasibility study. Secondly, stroke patients performed the functional tasks in this study with their most-affected hand, which could have been their dominant or non-dominant hand. This might have caused difficulties in performing functional tasks with and without the glove, because the most-affected hand of stroke patients is often used to support the non-affected hand instead of using it as primary hand to perform functional tasks (39). Therefore, subsequent studies should take the role of the gloved hand into
account. Thirdly, participants performed the functional tasks with and without the activated glove only. The fact that participants did not perform functional tasks with an inactivated glove makes it difficult to establish the influence on task performance of wearing a glove itself, for instance via loss of sensation, in particular during the performance of fine motoric activities (e.g. grasping the cap from the table). Fourthly, it is difficult to perform fine motoric tasks with the glove and to support fine motoric tasks with a soft-robotic glove. Therefore, usability of the current glove needs to be improved for fine motoric tasks, which should not be ignored during next design iterations. On the other hand, participants liked the extra support during gross motor activities. Therefore, gross motor activities should not be ignored in subsequent studies. Finally, no detailed evaluation of movement execution and quality of task performance were performed in extension of the single aspect of timed performance. Therefore, additional research is needed to investigate the effect of the HiM system in ADL in more detail, in terms of functional task performance, movement execution and handgrip/pinch strength, as well as the effect of the HiM system after prolonged use.
This feasibility study showed that chronic stroke
patients with limitations in ADL due to impaired hand function were positive about the usability of the first HiM system prototype and were motivated to use it. The system is aimed at intensive and functional upper limb rehabilitation as well as assistance during ADL. Nevertheless, design adaptations are needed to improve ease of use, usability and system performance. Functional performance duration with the glove improved across 3 repetitions up to the level of their performance time without the glove.
This work was partly funded by EUROSTARS (Project E!8227) via the State Secretariat for Education Research and Innovation (Switzerland) and Vinnova (Sweden). The authors of this study would like to thank our project partners Bioservo Technologies AB and Hocoma AG for the provided systems and their technical support during the study.
Potential conflict of interests: Our project partners Bioservo Technologies AB and Hocoma AG were involved in the EUROSTARS project (Project E!8227), and interested in commercializing the HandinMind system. Alejandro Melendez-Calderon was with Hocoma AG at the time of the study, but is now with Cereneo AG, Switzerland. He does not receive any financial or personal benefits from Hocoma AG or any other source for the publication of this study.


 Click to show fullsize
Click to show fullsize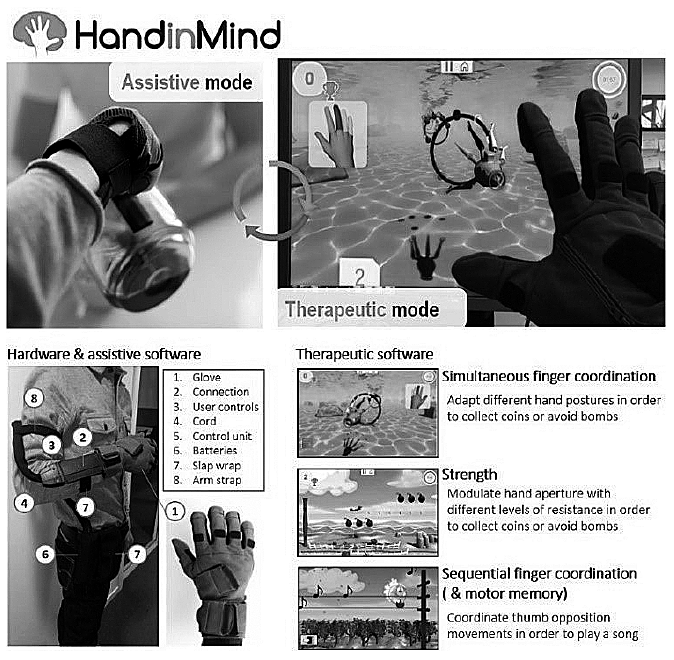 Click to show fullsize
Click to show fullsize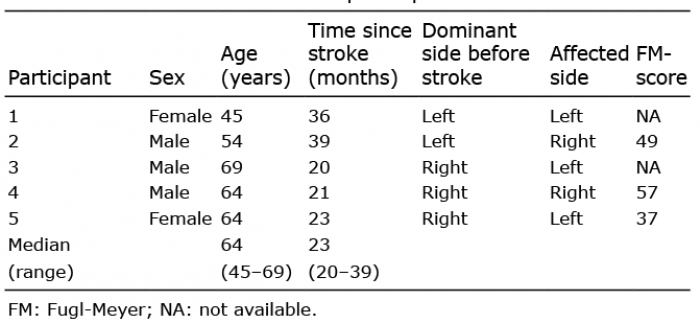 Click to show fullsize
Click to show fullsize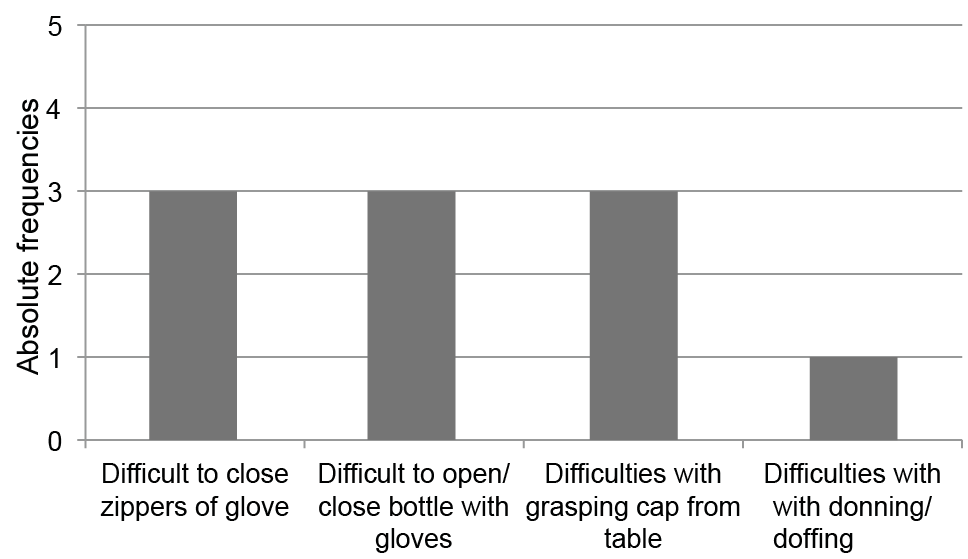 Click to show fullsize
Click to show fullsize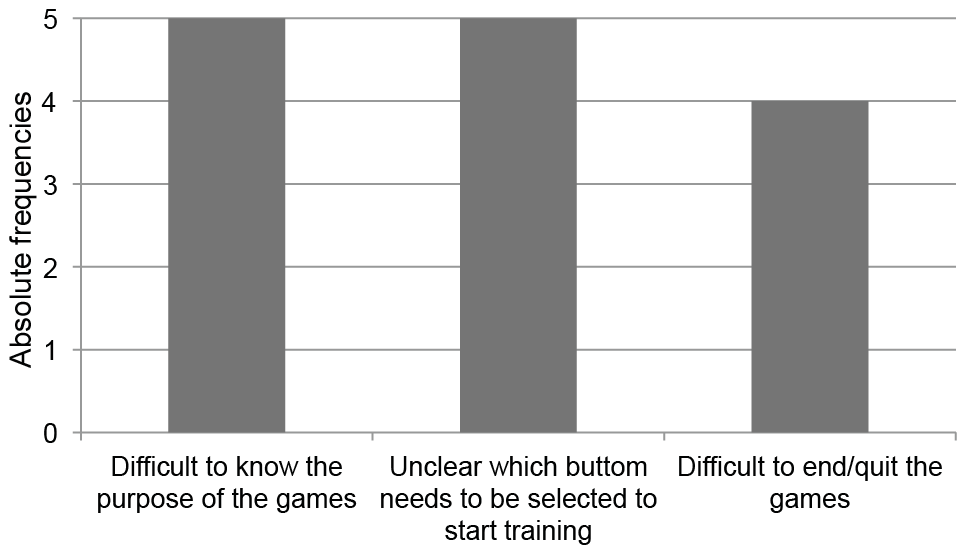 Click to show fullsize
Click to show fullsize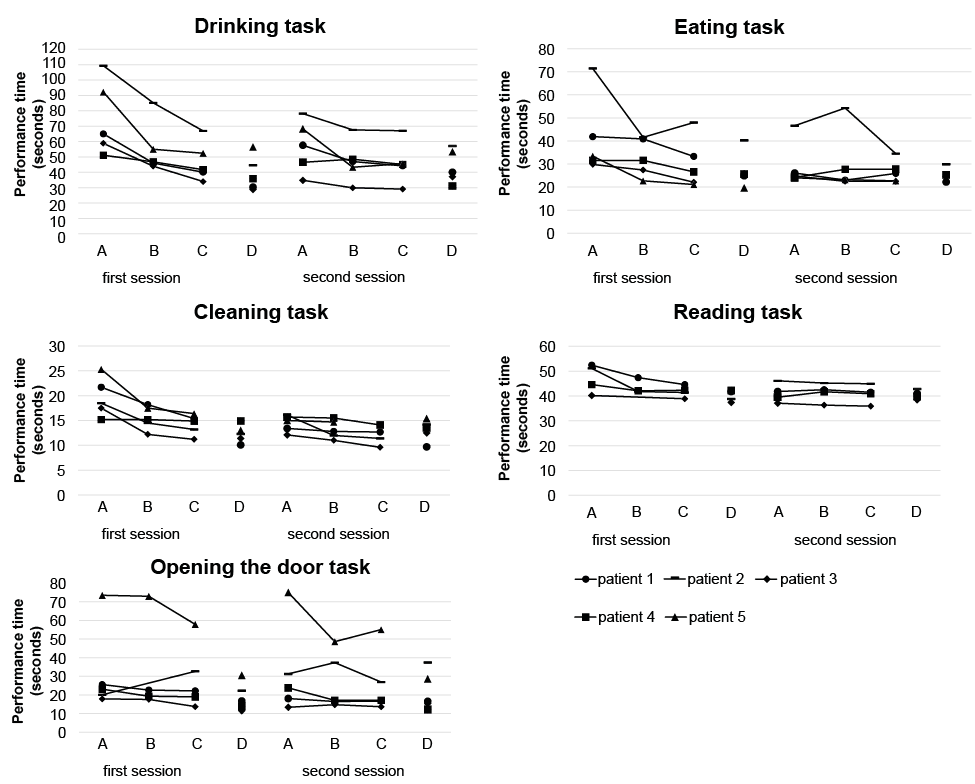 Click to show fullsize
Click to show fullsize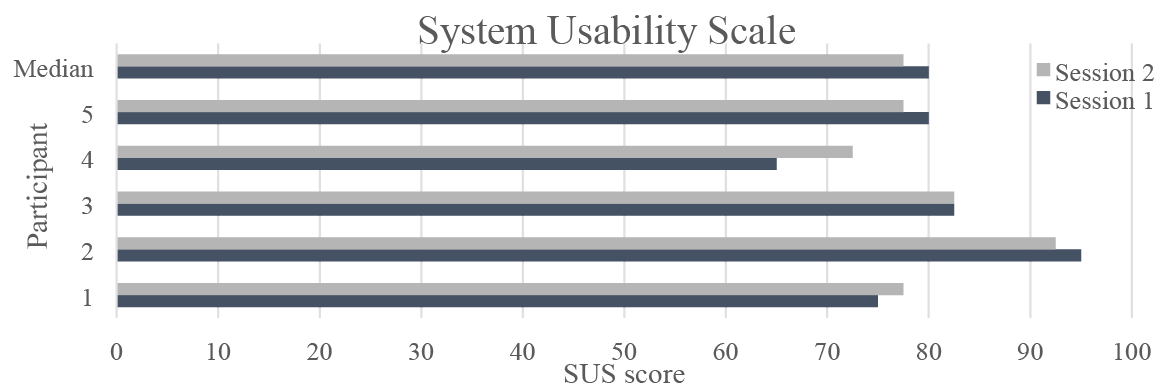 Click to show fullsize
Click to show fullsize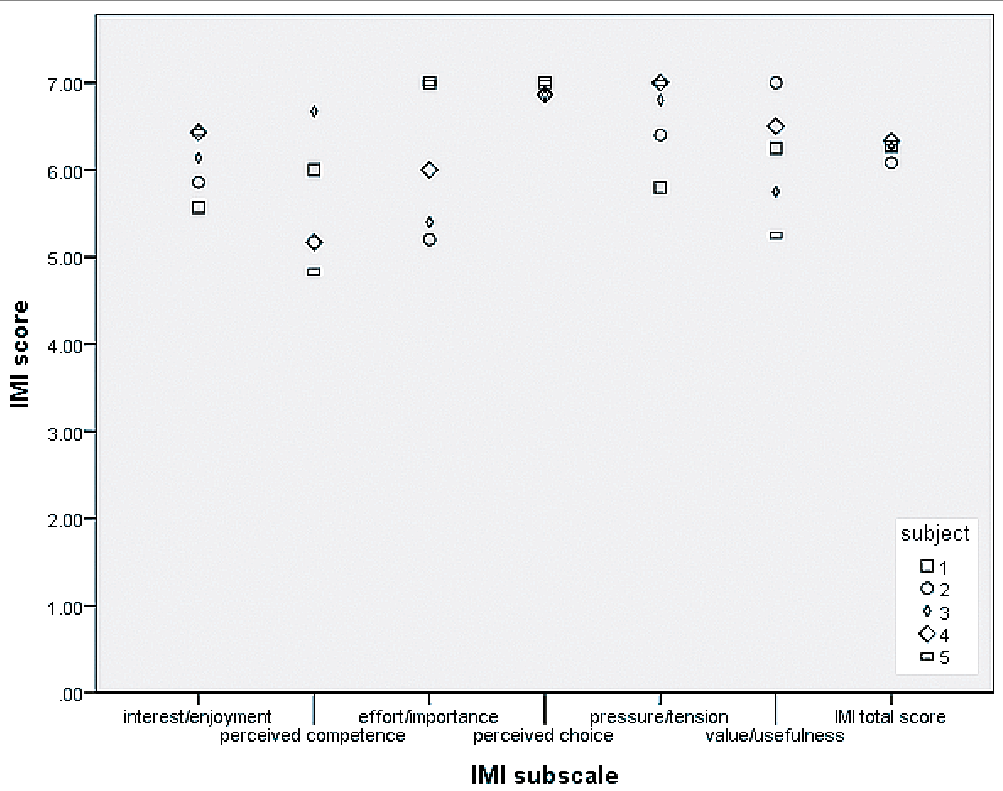 Click to show fullsize
Click to show fullsize