
From the 1Sunnaas Rehabilitation Hospital, Nesodden, and 2Department of Psychology, University of Oslo, Oslo, Norway
Objectives: To investigate self and informant ratings of everyday executive functions and their correlation with driving behaviour after acquired brain injury.
Methods: A 1-year follow-up study of 24 adults with stroke and 10 adults with traumatic brain injury deemed fit to drive after a multidisciplinary driving assessment. Baseline measures included neuropsychological tests and self and informant reports of everyday executive function (Behavior Rating of Executive Function; BRIEF-A). Follow-up measurements were the Swedish Driver Behaviour Questionnaire (DBQ) and Sunnaas Driving Pattern Questionnaire (SDPQ).
Results: Patients’ ratings on the BRIEF-A were significantly associated with the DBQ at follow-up, whereas informants’ ratings were not. Neither patients’ nor informants’ reports were associated with accident involvement or the use of compensatory driving strategies. No significant associations were found between level of awareness and driving parameters.
Conclusion: Patients’ reports of everyday executive functioning were more strongly associated with driving behaviour than were informants’ reports. Future studies are warranted to explore how informant and patient reports can contribute to distinguishing safe from unsafe drivers among patient groups with impaired awareness of deficits.
Key words: stroke; traumatic brain injury; driving assessment, executive function, self-awareness; informant report; driver behaviour.
Accepted Apr 19, 2018; Epub ahead of print Jul 2, 2018
J Rehabil Med 2018; 50: 589–597
Correspondence address: Per-Ola Rike, Sunnaas Rehabilitation Hospital, NO-1450 Nesoddtangen, Norway. E-mail: perola.rike@sunnaas.no
Not all survivors of stroke or traumatic brain injury resume driving, due to sensory, motor and cognitive deficits. In general, in other studies of brain-injured drivers, caregivers’ perceptions of patients’ driving-related capacities have been shown to be strong predictors of driving behaviour in daily life. However, this study found that patients, rather than caregivers’, perceptions of driving fitness, were most strongly related to driving behaviour, such as driving mistakes and inattention. We conclude that it is important to consider patients’ own perceptions of their driving-related functions when assessing fitness to drive after a brain injury.
Adequate cognitive functioning and higher-level mental functions, such as self-regulation and awareness of deficits, are prerequisites for safe driving (1, 2). Performance-based cognitive tests adequately assess cognitive functions relevant to driving, but they do not necessarily identify higher-level mental functions, such as executive functions, self-regulation and awareness of deficits (3, 4). Rating measures are suited to assessing higher-level functions, and studies have shown that how drivers perceive their own abilities is related to their daily driving behaviour (5–7). Informant rating of cognitive and executive functions has been less explored as predictors of post-injury driving behaviour, but discrepancy scores between participant and informant ratings may produce a measure of awareness of deficits suitable for driving studies (8, 9).
The main aim of this study was to explore to what extent participant and informant ratings of executive functioning are related to post-injury driving variables (i.e. daily driving behaviour and accident involvement) in a cohort of post-injury drivers who have passed a multidisciplinary driving assessment (MDA).
Higher-level mental functions include adjoining constructs, such as executive functions, self-regulation and self-awareness (10, 11), and may impair driving fitness (12). Executive functions, including abilities such as planning, problem-solving, response inhibition, cognitive flexibility and self-awareness (13), have been found to play a role in adjusting driver behaviour, the ability to make adequate compensatory decisions and the moderation of accident risk (2, 11, 14). Awareness of deficits is found to invoke the use of compensatory strategies to moderate risk, including not engaging in situations that are beyond one’s capabilities (2). Studies have found that drivers with impaired self-awareness are more likely to overestimate their driving ability, drive more, have a more risky driving style with higher incident involvement (15), be significantly more likely to report accident involvement (16) and fail on-road driving tests more often than persons with intact awareness (2, 17). Thus, higher-level mental functions appear to influence driving outcomes directly, as well as being a moderator between neuropsychological functioning and driving performance (2, 9).
A number of studies have found performance-based measures, such as neuropsychological tests, to serve as predictors of driving ability in neurological disorders, such as stroke, traumatic brain injury (TBI), multiple sclerosis and Parkinson’s disease (8, 14, 18–21). Performance-based neuropsychological tests are administered in standardized conditions, where stimulus presentation is carefully controlled. In addition, the measures are typically based on the examinee’s accuracy, response time and responding under a time constraint (3). Shortcomings of neuropsychological tests have been noted, especially with regard to assessing higher-level mental functions, such as self-awareness, self-monitoring, planning and decision-making (9).
An individual may use compensatory strategies in everyday life, but is prevented from using them in the test situation, which is important information when predicting everyday executive skills (22). Rating measures, incorporating self- and informant-reported information about difficulties in daily living, may serve as a window into higher-level mental functions. Some rating measures are widely used in the rehabilitation field, such as the Awareness Questionnaire (AQ) (23) and the Behavior Rating Inventory of Executive Function – Adult Version (BRIEF-A) (24).
One study reported that self-reported executive dysfunctions on the BRIEF-A were associated with increased number of aberrant driver behaviours in a sample of healthy Australian drivers (14), while high symptom ratings on the BRIEF-A self-report form have been associated with attention regulation difficulties and driver errors on the Driver Behaviour Questionnaire (DBQ) in a sample of Canadian undergraduate students (25). Self-ratings of functional abilities after stroke and TBI may therefore provide insight into a person’s beliefs about his or her own confidence and level of awareness, which is suggested to be one of the most important predictors of driving performance and behaviour (26). Only a few studies have explored the use of informant ratings after brain injury. Studying TBI survivors, Coleman and colleagues (8) found that caregiver ratings on the Patient Competency Rating Scale were a better determinant of whether patients resumed driving, including how much they drove, than were the patient’s own ratings. Using discrepancy scores between the participant and the informant on the AQ (23) in order to establish levels of awareness, Griffen and colleagues found that better driving performance on an on-road driving test was strongly associated with better awareness of deficits reported by participants and informants (9).
The BRIEF-A is a widely used descriptive measure of executive function including both a self-report and an informant form. Many studies indicate that the BRIEF-A measures executive functioning in daily living to a stronger extent than standardized neuropsychological evaluations (27, 28). Although some studies support a relationship between self-report on the BRIEF-A and driver behaviour (14, 25), no studies have, to the authors’ knowledge, simultaneously investigated patient and informant ratings on the BRIEF-A in relation to driving behaviour after a brain injury.
Research on fitness to drive after stroke or TBI has mainly used 3 outcome measures: (i) driving tests (such as open and closed on-road driving performance and driving simulator studies); (ii) accident rates; and (iii) self-report of daily driving behaviour.
On-road driving tests are one of the most used outcome measures in driving assessments; however, it has been argued that higher-level driver behaviour (e.g. risk-taking, self-awareness and decision-making) may be difficult to measure in a valid way, as some drivers may suppress risky driving behaviour during the driving test (29). Furthermore, predicting fitness to manage driving in daily living extends the frame of an on-road assessment in which more complex cognitive abilities are challenged (30). Studies have yielded mixed results as to whether driving after a brain injury leads to increased accident risk (12).
Rating measures have traditionally been a less-studied outcome measure than driving assessments and accident rates (12). However, research has pointed to the fact that daily driving behaviour may serve as a mediating factor between neuropsychological functioning and accident rates (31). While driving tests and accident rates include observable and objective data, daily life driver behaviours are accessible
through self-rating measures, such as the Manchester Driver Behaviour Questionnaire (DBQ) (32). Thus, self-reported rating measures are suited to fill the gap between performance-based predictors and accident involvement.
The main aim of this study was to explore the use of patient and informant ratings on the BRIEF-A administered during a multidisciplinary driving assessment in relation to post-injury driving behaviour. In accordance with studies showing that the lack of awareness of deficits may relate to poorer driver performance and aberrant driver behaviour (2, 8, 9), the present study also explored whether awareness of executive deficits was associated with follow-up driver behaviour. The following research questions were addressed:
The data presented in this study were collected as part of a larger consecutive case series follow-up study of stroke and TBI survivors considered suitable for driving according to an MDA at Sunnaas Rehabilitation Hospital, Norway (33).
All participants were patients with stroke or TBI referred to the Sunnaas Rehabilitation Hospital for an MDA 3 months or more post-injury. The participants had at one time not fulfilled the Norwegian health requirements for driving due to sequelae of their brain injuries.
The inclusion criteria were: patients who had: (i) passed the MDA, as described in the main study (33); (ii) had had a stroke or TBI confirmed by computerized tomography (CT) or magnetic resonance imaging (MRI); (iii) had good Norwegian language skills; and (iv) held a driver’s license prior to the injury. Exclusion criteria were: severe psychiatric illness, dementia or severe cognitive deficits contrary to a driving assessment caused by other somatic or neurological illnesses.
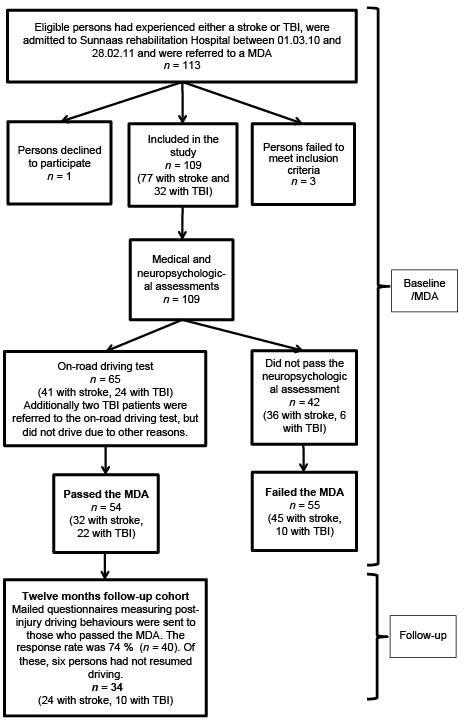
A total of 113 patients were eligible for participation. Of these, 3 were excluded due to severe aphasia and somatic illnesses, and 1 opted to not participate. A total of 109 participants (77 stroke patients and 32 TBI) were included in the main study between the ages of 19 and 80 years. The follow-up cohort consisted of the participants who passed the MDA and returned the questionnaires measuring post-injury driving behaviour that were sent to them after the MDA (n = 34). The sample included 24 stroke survivors and 10 TBI survivors. The flow-chart of participants and assessments is shown in Fig. 1.
Fig. 1. Flow chart of participants.
Written and signed informed consent was obtained from all participants. The study was approved by the Regional Committees for Medical and Health Research Ethics, South-East, Norway, and completed in accordance with the Declaration of Helsinki.
Data for this study were collected during an MDA and approximately 1 year after the MDA. The MDA consisted of a medical evaluation and a neuropsychological assessment, in which the majority of participants were also referred for an on-road driving test. The outcome of the MDA (i.e. pass or fail) was carried out by a physician and a neuropsychologist and based on the Norwegian health requirements for driving fitness. For research purposes only, both participants and informants (defined by the participant as a significant other) were asked to complete the BRIEF-A during the MDA (baseline). To reduce potential under-reporting of symptoms, both participants and informants were informed that their ratings would not have any impact on the outcome of the MDA. Approximately 12 months after baseline, participants who passed the MDA reported follow-up measurements of post-injury driver behaviour (DBQ and the Sunnaas Driving Pattern Questionnaire (SDPQ)).
Neuropsychological test battery. Participants were administered a neuropsychological test battery composed of 19 neuropsychological tests, as follows. Visual field deficits: the Friedmann Visual Field Analyser MK2 (number of misses: maximum 60). Number of misses on the Friedmann may be an indicator of visual deficits and/or visual inattention. Visual attention: the Sunnaas Tachistoscope Test, which is a computerized test of visual attention and neglect, in which symbols are briefly presented bilaterally across 18 trials. A total of 54 hits are achievable in the simple and complex sub-tests. Visuomotor reaction time: React (Gianutsos) is a computerized test in which participants are instructed to respond by pressing the space bar as soon as they detect numbers that appear randomly on the screen. A total score is calculated by summing the mean reaction time (in s) to the left, right and middle visual fields, and dividing this number by 3. Psychomotor speed and mental effectivity: the Grooved Pegboard Test, the Trail Making Test A, the Symbol Digit Modalities test (SDMT), and the D-KEFS Colour Word Interference Test, parts 1 and 2. Visuospatial: copy a 3-dimensional (3D) cross (maximum score 10 points) and Block design (WAIS-III), Verbal abstraction: similarities (WAIS-III). Visual reasoning: picture completion (WAIS-III). Executive cognitive functions: the D-KEFS Colour Word Interference Test, parts 3 and 4, Digit Span and Trail Making Test B tasks. Age adjustments were made for all scores on the WAIS-III and D-KEFS. Age, sex and education adjustments were made for the Halstead-Reitan scores.
Executive functions in daily living (BRIEF-A). All participants were administered an authorized Norwegian translation of the BRIEF-A (24), a 75-item questionnaire that measures different aspects of executive functions as they manifest themselves as real-life situations. In addition, informants were administered the BRIEF-A informant version. All items are answered with options 1 (never a problem), 2 (sometimes a problem) or 3 (always a problem). Three main indexes are derived: the Metacognition Index (MI), consisting of the subscales Initiate, Working Memory, Plan/Organize, Task Monitor and Organization; the Behavioural Regulation index (BRI), consisting of the subscales Inhibit, Shift, Emotional Control and Self-Monitoring; and the Global Executive Composite (GEC), a summary score, consisting of all the clinical scales of the BRIEF-A. To operationalize level of awareness, a discrepancy score was calculated by subtracting informants’ ratings on the BRIEF-A GEC raw scores from patients’ ratings. Positive scores indicated that patients rated themselves as having more executive symptoms than did their informants (i.e. underestimation of competencies), negative scores indicated that participants reported less executive symptoms than did their informants (i.e. impaired awareness), whereas scores approaching zero indicate convergence between participant and informant report (i.e. intact awareness). Three awareness groups were computed using standardized values (z-scores) from the discrepancy scores on the BRIEF-A: (i) intact awareness (discrepancy score ranging from –0.5 standard deviation (SD) to +0.5 SD); (ii) impaired awareness (discrepancy score below –0.5 SD); and (iii) underestimation of competencies (discrepancy scores above +0.5 SD).
Data regarding a variety of pre-injury driving characteristics were collected using the SDPQ (29). The questionnaire is a modified version of that of Schultheis and colleagues (34). Participants were asked to report specific pre-injury driving characteristics, such as the number of years that they held a driver’s license, distance (km) driven per week, use of compensatory driving strategies, and at fault reported and unreported accidents over the last 5 years prior to their injury.
Driver behaviour. An authorized Norwegian translation of the Swedish DBQ (35) was administered. The questionnaire is based on the Manchester DBQ, which aims to measure different types of driving errors and violations through self-report (32). The Swedish DBQ contains 32 items (each scored from 0 (never) to 5 (very often)) and is divided into the following subscales: driving violations, inattention, inexperience and mistakes.
Post-injury driver characteristics. At follow-up, participants completed the SDPQ, reporting their post-injury driving behaviour. The parameters selected for this study were distance driven per week (km), numbers of compensatory driving strategies and accident rates (reported and unreported accidents). Compensatory driving strategies were measured by ticking off the relevant items of the 8 following options: (i) drive more slowly, (ii) drive mostly together with others, (iii) avoid cities, (iv) avoid unknown places, (v) drive only when feeling well, (vi) only drive during the daytime, (vii) avoid highways, and (vii) avoid rush hour. The frequency of accidents (reported and unreported) was calculated per million km driven (29).
Statistical analyses were performed using SPSS PASW (version 25.0). Prior to analysis, data were screened for violations of assumptions for parametric tests. For measures that markedly violated the assumptions for parametric statistics due to non-normal distributions (DBQ, items from the SDPQ and BRIEF-A), data analysis was conducted with non-parametric tests. Raw scores were used in the analysis. To compare patient and informant reports on the BRIEF-A, Mann–Whitney U tests were used. Because patient and informant report may be related, paired testing was also conducted. Independent samples t-tests were applied to explore whether the BRIEF-A ratings differed with regard to diagnosis. To compare baseline reports on the BRIEF-A and follow-up reports on the DBQ, bivariate Spearman rank-order correlations (rho) were calculated. Correlations were considered weak below 0.3, moderate between 0.3 and 0.5, and strong from 0.5 to 1.0 (36). To investigate whether level of awareness was related to 4 specific follow-up driving behaviour parameters, namely: (i) distance (km) driven per week, (ii) numbers of compensatory strategies, (iii) DBQ, and (iv) accident rates, a one-way analysis of variance was conducted (Kruskal–Wallis test by ranks). Level of awareness was operationalized with the use of discrepancy scores from the patient and informant report on the BRIEF-A. The calculations are described in detail in chapter 2.4.2.1.
The follow-up sample included 34 participants. Of these, 24 had had a stroke and 10 had had a TBI. In addition, 31 informants completed the BRIEF-A during the MDA. Demographic and clinical data for all participants are presented in Table I, but demographic data were not available for the informants.
Table I. Demographic and medical characteristics of stroke and traumatic brain injury (TBI) participants
As shown in Table I, 10 participants who had strokes had aphasia and 8 participants had hemiparesis, which mainly accounted for the missing data in the baseline measurements. Further details of the demographic and clinical data are described in the main study (33).
As shown in Table II, the participants performed most neuropsychological tests within the normal range (±1 SD). Adjusted scores were used for tests with available norms. Raw scores are reported for tests where no norms are available, i.e. tests of visual attention and reaction time and Copy a 3D cross. Any missing data on the tests were due to either aphasia or hemiparesis. There were no significant differences between stroke and TBI participants with regards to cognitive performance (for further details, see Table II in Rike et al. (2016), which included the same individuals (37)).
Table II. Neuropsychological data (n = 34)
Descriptive data from the BRIEF-A ratings are shown in Table III, missing informant data (n = 3) was due to non-returned questionnaires. The analyses showed no significant differences between patient and informant ratings on any of the subscales or main indexes on the BRIEF-A. Patients reported somewhat higher scores (increased symptoms) on the BRIEF-A Metacognition Index and the Global Executive Component, but the results did not reach significance. There were no significant differences on the patient or informant ratings on the BRIEF-A with regard to diagnosis. Thus, the data from stroke and TBI are presented together in Table III. Furthermore, in order to investigate whether the responders (n = 40) differed from non-responders (n = 14) at follow-up with regard to baseline patient and informant ratings on the BRIEF-A, independent samples t-tests were carried out. No significant differences were observed between responders and non-responders on any of the 3 main indexes or the 9 subscales.
Table III. Descriptive data from patient and informant ratings of the BRIEF-A
Driver behaviour. A Spearman’s rank-order correlation (rho) was used to investigate associations between patient and informant ratings on the BRIEF-A and follow-up patient ratings of daily life driver behaviour (DBQ violations, mistakes, inattention and inexperience).
As shown in Table IV, multiple significant correlations were seen between the patients’ baseline ratings on the BRIEF-A main indexes and the DBQ at follow-up. Specifically, the relationships between the BRIEF-A MI and GEC and DBQ Mistakes and Inattention Subscales were strong, while the correlation between BRIEF-A BRI and DBQ Mistakes and Inattention were considered moderate. No such significant associations were found between baseline informant ratings on the BRIEF-A and patients’ ratings on the DBQ at follow-up.
Table IV. Spearman intercorrelations between patient and informant ratings of driving behaviour and executive functions
Analyses were conducted in order to investigate whether patient and informant BRIEF-A scores were associated with specific post-injury driving characteristics (i.e. distance (km) driven per week, numbers of compensatory driving strategies and accident rates from the SDPQ). The only significant finding was a positive association between informant ratings on the BRIEF-A Metacognition Index and distance (km) driven per week post-injury, i.e. a higher number of symptoms on the Metacognition Index was related to shorter distances per week (r = 0.381, p = 0.034, n = 31).
To investigate whether the level of awareness of executive functioning was related to the 4 specific follow-up driving behaviour parameters ((i) distance (km) driven per week, (ii) numbers of compensatory strategies, (iii) DBQ, and (iv) accident rates), an analysis of variance was conducted (Kruskal–Wallis). The only significant finding was that km driven per week was significantly higher in the Intact awareness group (F (2,28) = 4.066, p = 0.028). Due to the low numbers of participants in each awareness group, between-group differences comparing pre-injury/baseline vs follow-up distance (km) driven per week were not available in this study. The descriptive data showed that all groups reduced their driving from pre-injury to follow-up (33). Specifically, for those with impaired awareness, median (interquartile range [IQR]) distance (km) driven per week was 95.0 (18.7–152.5) km at follow-up compared with 300.0 (200.0–400.0) km from baseline/pre-injury. In group 2 (Intact awareness), median km driven per week was 250.0 (137.5–425.0) km at follow-up compared with 385.0 (205.0–500.0) km pre-injury. In group 3 (Underestimation of competence), median distance (km) driven per week was 100.0 (31.5–195.0) km at follow-up compared with 225.0 (70.0–575.0) km pre-injury. Furthermore, the results showed that participants with intact awareness reported less use of compensatory driving strategies, mean 0.21 (standard deviation; SD 0.43), compared with those with impaired awareness 0.88 (SD 1.13) and the participants who underestimated their competencies 0.77 (SD 1.4). However, the group differences failed to reach statistical significance (p = 0.069). For those with impaired awareness, median (IQR) number of accidents per million driven km was 0.0 (0.0–0.0) at follow-up. In group 2 (Intact awareness), median (IQR) number of accidents per million km driven was 0.0 (0.0–48.1). In group 3 (Underestimation of competence), median (IQR) number of accidents per million km driven was 0.0 (0.0–56.4). Analysis of variance found that level of awareness was not significantly related to any of the DBQ subscales or accident rates. Further analyses were conducted (data not shown) to investigate associations between neuropsychological functioning and level of awareness and involvement in accidents, respectively, but no significant associations were found.
The main aim of this study was to investigate the relationship between patients’ and informants’ perceptions of executive functioning (BRIEF-A) and post-injury driver behaviour in a cohort of drivers who had passed an MDA. The study found that patient ratings on the BRIEF-A were significantly associated with driver behaviour, as measured by the DBQ, whereas informant ratings were not. However, there was a significant negative association between the Metacognitive Index on the informant BRIEF-A and mileage driven at follow-up. Furthermore, patients with intact awareness had significantly higher mileage driven at follow-up compared with participants with impaired awareness or those who underestimated their competencies.
The first research question was whether patients rated themselves differently from informants on measures of executive functions (BRIEF-A) during an MDA (baseline). The results showed no significant differences between patient and informant ratings, but there was a tendency towards higher ratings on the patient BRIEF-A Metacognition Index and the Global Executive Component.
The second research question was to explore to what extent baseline patient and informant ratings of executive functions (BRIEF-A) were associated with follow-up driving behaviour approximately 12 months after the MDA. Patients’ ratings on the BRIEF-A displayed the strongest associations with driver inattention and mistakes (DBQ), whereas informant ratings did not. This is in contrast to other studies, in which caregivers’ perceptions of patients’ fitness have significantly predicted driving behaviour among patients with TBI and Parkinson’s disease (8, 38). The following methodological differences may explain these inconsistent findings. First, the current study used the 75-item BRIEF-A, a questionnaire of everyday executive functioning with no driving-related items. By contrast, Coleman and colleagues (8) included patient and caregiver responses only from the single driving-related item from the Patient Competency Rating Scale (PCRS) in order to predict driving behaviour outcomes. Secondly, Coleman and colleagues included a larger sample size consisting of TBI drivers and non-drivers; they also used different driving outcome parameters, such as driving status, driving distance per week and accident involvement.
In addition, in the current study, all participants had passed an MDA, thus they most likely represent a cohort with adequate cognitive functions and insight into their potential cognitive deficits compared with other studies that also included non-drivers with presumably more severe cognitive deficits. This may enable them to better identify their executive difficulties in daily living to a larger extent than their informants, symptoms that in this study were strongly associated with the cognitive aspects of driving, i.e. driving inattention and mistakes. Studies of other neurological disorders, such as Parkinson’s disease, have also reported that caregivers’ ratings of the patients’ driving ability predict driving performance. A study by Cordell and colleagues (38) showed that caregivers’ perceptions of driving fitness among drivers with Parkinson’s disease predicted the outcome of an on-road driving test. As noted in Coleman and colleagues’ study, the measurements are not comparable to those in our current study.
Altogether, these methodological differences, i.e. different diseases, sample sizes, and predictors and outcome measures, may explain the divergent findings regarding the predictive value of caregivers’ responses shown in our study. Thus, the findings cannot be directly compared with findings from most previous studies.
Furthermore, neither patient nor informant ratings on the BRIEF-A were associated with accident involvement or the use of compensatory driving strategies. The lack of correlation between the BRIEF-A and accident involvement is most likely because accidents are rare events. The lack of association between the BRIEF-A and reported use of compensatory strategies may be because the patients as a group reported little use of compensatory driving strategies compared with pre-injury levels (as reported by Rike et al. (33)). On the other hand, the low number of compensatory driving strategies may, for some individuals, express impaired insight into the need to adjust one’s driving habits after an ABI, but this conclusion was not reflected in the patient and informant ratings on the BRIEF-A, which did not differ significantly. Furthermore, making use of compensatory strategies is not only a question of awareness of deficit, but also of willingness to adapt to limitations. Studies have found that some brain-injured drivers do not compensate for their impaired driving abilities, even if they acknowledge their limitations (29).
The only significant association between BRIEF-A informant ratings and post-injury driving parameters was that high ratings on the Metacognitive Index were associated with lower mileage driven per week. This finding is in line with Coleman et al. (2002), who reported that informant ratings were better predictors of the number of miles driven post-injury than were the patients’ self-ratings. One explanation for this finding might be that patients rated by their informants as having more executive symptoms in daily functioning may struggle more in resuming vocational and social participation and therefore have less need for transportation.
The final research question was to what extent level of awareness of executive deficits related to follow-up driving behaviour. Consistent with some previous findings (8), participants in the intact awareness group drove significantly further per week. There was a tendency that the group with intact awareness also used fewer compensatory strategies than both the participants with impaired awareness and those underestimating their competence. In contrast, another study by Rapport et al. (15) reported that brain-injured drivers with impaired awareness drove further per week and had more driving accidents than drivers with intact awareness. However, in this study, participants with impaired awareness were defined in terms of having cognitive deficits on neuropsychological tests, but still rated their current abilities as unchanged or high. In the current study, the discrepancy scores on the BRIEF-A were used to operationalize levels of awareness. As patients in the current study performed well on neuropsychological tests, it is possible that they displayed better cognitive functioning than the participants in the study by Rapport et al. (15), which might explain the difference in results.
On the other hand, patients rated as underestimating their competencies might limit their driving due to lower perceived abilities. This is in accordance with previous findings showing a relationship between low driving self-efficacy and lower driving mileage (7). In contrast to previous findings (16), no association was found between level of awareness and involvement in accidents at follow-up. As already mentioned, accidents are rare events, and associations between the BRIEF-A and accidents were expected to be low.
A limitation of the study is that the stroke participants were younger than the general stroke population, and the TBI participants were older than the general TBI population. Furthermore, the sample size was modest (n = 34), and the timeframe for follow-up was relatively short (12 months). These issues call for caution in generalizing the findings.
A methodological concern of using rating measures to assess higher-level mental processes and driver behaviour is the possibility of under-reporting due to social desirability effects. This issue might especially be the case as data were collected during a clinical driving assessment. All the patients/participants in this study had previously been deemed fit to drive in a comprehensive MDA, indicating fairly well-preserved cognitive functions. This fact might have restricted the range and variance of the responses on the self-rating measures, as patients with severe cognitive deficits who did not pass the MDA were not included in this follow-up study. Factors such as reduced awareness of deficits (39) and social desirability bias (40) may have affected the validity of the self-report.
Rating measures may serve as a window into higher-level cognitive functions relevant to driving fitness, which may not be assessable through performance-based measures. The data from this study suggest that patients’ ratings on the BRIEF-A are more strongly associated with aberrant driver behaviour at follow-up than are informant ratings. The level of awareness, operationalized in terms of discrepancy scores between patient and informant ratings, did not show any significant associations with follow-up driver behaviours, although a tendency towards greater distance driven and less use of compensatory strategies was documented for patients with intact awareness. As the participants in this study had all passed an MDA and could be expected to display well-preserved cognitive function, an interesting avenue of future research on higher-level mental functions and driving would be to study patients with more severe cognitive dysfunction in greater depth and with other methods, such as driving simulators.


 Click to show fullsize
Click to show fullsize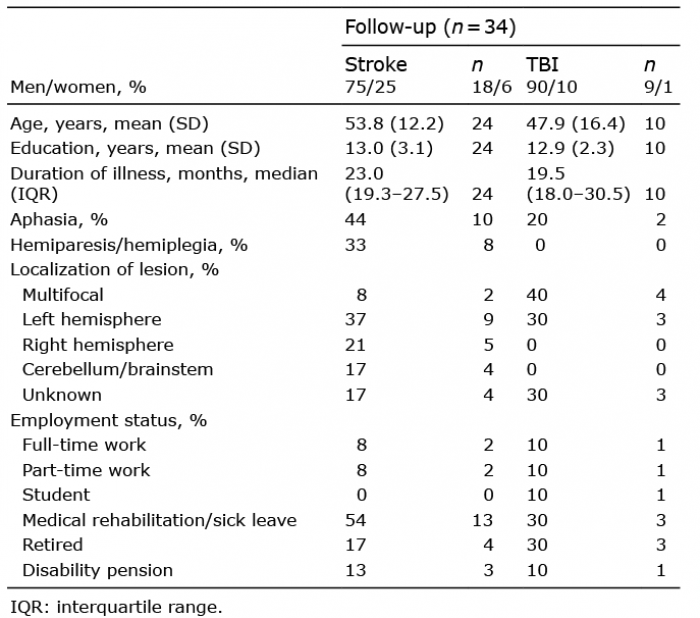 Click to show fullsize
Click to show fullsize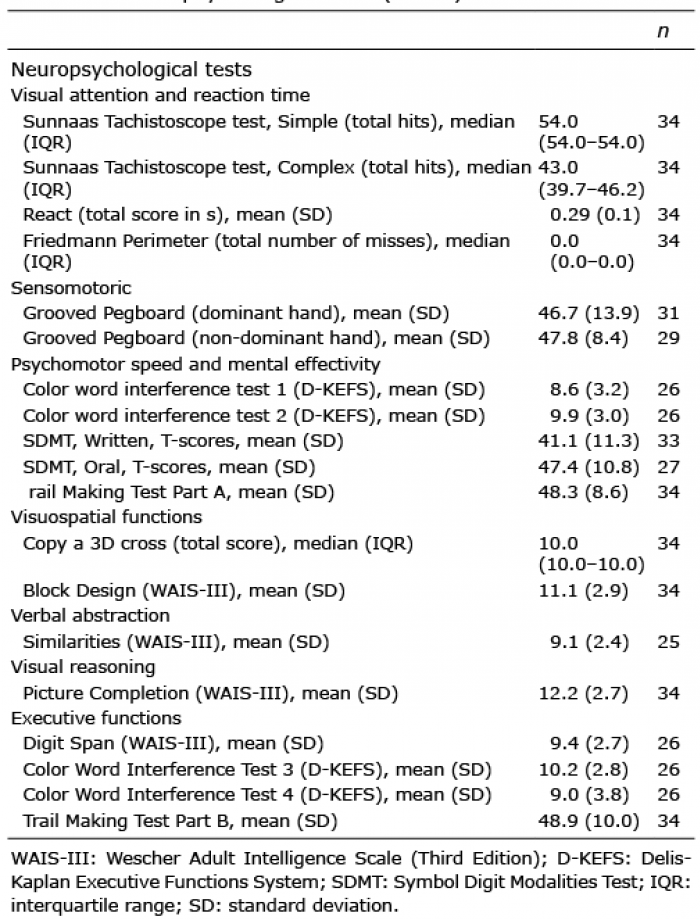 Click to show fullsize
Click to show fullsize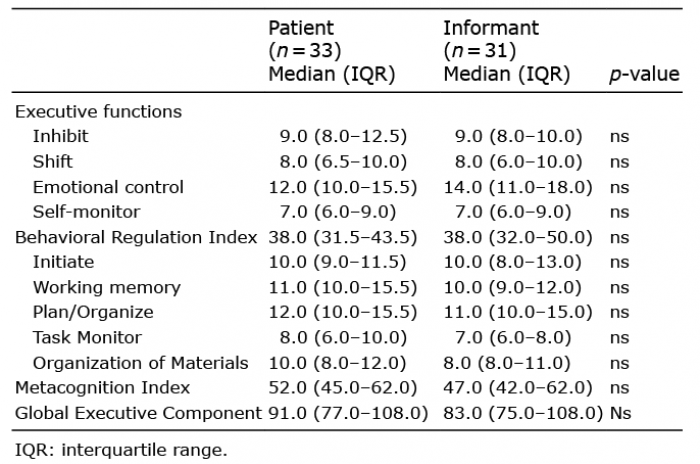 Click to show fullsize
Click to show fullsize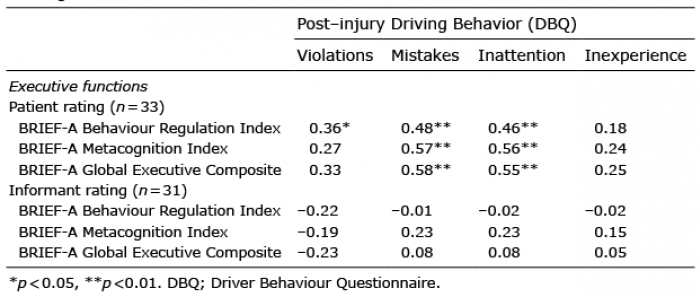 Click to show fullsize
Click to show fullsize