
From the 1Department of Rehabilitation Medicine, Erasmus MC, University Medical Centre Rotterdam, 2Rijndam Rehabilitation, 3Department of Paediatric Neurology, Erasmus MC, University Medical Centre/Sophia Children’s Hospital, Rotterdam, and 4Department of Rehabilitation Medicine, VU, University Medical Centre Amsterdam, Amsterdam, The Netherlands
Objective: Botulinum toxin (BoNT-A) is widely used in combined treatment for spastic cerebral palsy, but its added value preceding comprehensive rehabilitation for motor impairments, gait, and goal attainment
has not been studied.
Design: A comparative multi-centre trial, in which two groups underwent comprehensive rehabilitation (i.e. high-intensive functional physiotherapy, and indicated casting/orthoses). One group received intramuscular BoNT-A prior to rehabilitation, and the other group did not receive BoNT-A.
Subjects/patients: Children with spastic cerebral palsy, Gross Motor Function Classification System (GMFCS) levels I–III, age range 4–12 years, indicated for BoNT-A treatment regarding mobility problems.
Methods: Sixty-five children participated (37 boys), mean age 7.3 years (standard deviation (SD) 2.3, range 4–12 years), equally distributed across GMFCS levels. Forty-one children received BoNT-A+ comprehensive rehabilitation and 24 received comprehensive rehabilitation only. Functional leg muscle strength, passive range of motion, angle of catch, cerebral palsy-related pain, walking speed, kinematic gait parameters, goal attainment, and proxy-reported general functioning were assessed at baseline,
primary end-point (12 weeks) and 24-week follow-up.
Statistical analyses were performed with linear mixed
models.
Results: At the primary end-point there were no statistically significant differences in treatment effects between the groups, except for the angle-of-catch of the rectus femoris, which was in favour of comprehensive rehabilitation without BoNT-A (12° difference, 95% confidence interval (95% CI) 2:23, p = 0.025). Results at follow-up were similar.
Conclusion: At the group level, treating with BoNT-A prior to comprehensive rehabilitation did not add to the clinical effectiveness of rehabilitation. Thus, BoNT-A prescription and use should be critically reconsidered in this cerebral palsy age- and GMFCS-subgroup.
Key words: spastic cerebral palsy; botulinum toxin; functional physiotherapy; casting; orthoses; impairments; goal attainment; paediatric rehabilitation
Accepted May 17, 2018; Epub ahead of print Aug 6, 2018
J Rehabil Med 2018; 50: 732–742
Correspondence address: Fabienne Schasfoort, Department of Rehabilitation Medicine, Erasmus MC, University Medical Centre Rotterdam, PO Box 2040, NL-3000 CA Rotterdam, The Netherlands. E-mail: f.schasfoort@erasmusmc.nl
*This article has been handled and decided upon by Chief-Editor Kristian Borg
For children with spastic cerebral palsy who are able to walk independently, botulinum toxin injections are often part of a combined treatment to improve their functioning. Although it is known from the scientific literature that such combinations are more effective than low-intensity standard care, the relative contribution of the costly botulinum toxin injections to the total treatment effect is unknown. The aim of this study was to determine the added value of providing botulinum toxin treatment prior to a period of comprehensive rehabilitation compared with comprehensive rehabilitation alone in a group of 65 children aged 4–12 years. The effect outcomes measured were: leg muscle strength, muscle length and spasticity of several leg muscles, CP-related pain, walking speed, several gait pattern parameters, the degree to which individual therapy goals were attained, and parent-reported general functioning. At the group level, no differences were found in effect between the group that received botulinum toxin injections and comprehensive rehabilitation, and the group that received comprehensive rehabilitation alone. This suggests that the widespread prescription and use of botulinum toxin for spastic cerebral palsy in this age- and severity-subgroup needs critical reconsideration.
Botulinum toxin (BoNT-A) has been widely used in the treatment of ambulatory children with spastic cerebral palsy (CP) since the 1990s (1, 2). BoNT-A injections in the leg muscles temporarily block the neuromuscular junctions and thereby provide (better) conditions to optimize and reinforce the effects of post-BoNT-A adjunctive interventions. However, there is a consensus that BoNT-A should never be a stand-alone intervention (3–8). Therefore, BoNT-A injections are generally given as part of a combined, multimodal treatment package.
Although the body of evidence for such combined treatment packages including BoNT-A has increased since the first systematic review (3), the evidence is ambiguous (9) and even conflicting (10). Since it is difficult to perform controlled intervention studies in CP (5, 11), discussion about the content and contribution of both BoNT-A treatment and the adjunctive post-BoNT-A treatment modalities is ongoing (7, 11–24). However, previous controlled trials have shown that a more comprehensive treatment package including non-pharmacological interventions (such as functional and goal-directed physiotherapy, serial casting and/or ankle-foot orthoses (AFO)) following BoNT-A injections generally leads to better results than regular low-intensity “maintenance care” (e.g. 4, 11, 25–33).
An important characteristic of previous BoNT-A research is that the (adjunctive) non-pharmacological interventions are, in general, poorly described, with unknown content and of unknown quality (13, 16, 34–36). In 2006, Scholtes and colleagues noted that it was unclear to what degree positive effects of combined BoNT-A and comprehensive rehabilitation (CR) (compared with standard low-intensive care) could be attributed to BoNT-A injections or to characteristics of the other modalities applied in the ambulatory subgroup of children with CP (33). This “black box” issue has been reported frequently (11, 16, 34, 35, 37, 38). In recent years, there has also been increasing support for intensive individually tailored, functional and goal-directed physiotherapy-based interventions for spastic CP (in comparison with effectiveness of standard low-intensity care) (13, 39–51).
The added value of BoNT-A prior to CR (consisting of non-pharmacological modalities; physiotherapy, casting and orthosis) has not previously been explicitly studied, although there are a number of disadvantages to BoNT-A treatment (e.g. burden of treatment, toxin, use of anaesthetics, repeated treatments, expense). Therefore, we performed a clinical trial including economic evaluation named SPACE BOP (SPAstic cerebral palsy; Cost-Effectiveness of BOtulinum toxin and Physiotherapy). In this trial, the effectiveness and costs of BoNT-A plus CR were compared with the effectiveness and costs of CR alone in a group of ambulatory children with spastic CP in the age range 4–12 years. Both intervention groups received an equally high-intensity, best-available-evidence-based package of non-pharmacological interventions; physiotherapy, casting and orthosis. Improvement was found at the group level in both groups with regard to gross motor function, everyday physical activity levels and HRQoL, but there were no differences in effect between groups (52). Because it is unclear whether (absent) improvements in a single category from the International Classification of Functioning Disability and Health/ International Classification of Functioning Disability and Health-Children and Youth (ICF/ICF-CY) framework (53, 54) are related to (absent) improvements in other ICF categories (9, 55), the aim of this study was to determine the added value of BoNT-A preceding a period of CR for ambulatory children with spastic CP for a broad range of effect outcomes across ICF categories. This study evaluated CP-related pain, functional leg muscle strength, passive range of motion, angle of catch, walking speed and kinematic gait parameters, as well as proxy-reported general functioning and attainment of individual activity-related therapy goals.
The study design, inclusion criteria and procedures have been described previously (52). This methods section provides only summary data.
A single-blind, partly-randomized, comparative multi-centre trial was performed, in which the effectiveness of BoNT-A plus a 12-week period of comprehensive rehabilitation CR (BoNT-A+CR) was compared with the effectiveness of a 12-week period of CR alone (only-CR). Two groups received CR, consisting of individually tailored, high-intensity, goal-directed physiotherapy (iPT), and, if necessary, serial casting and/or AFOs. One of the groups received BoNT-A injections prior to CR, and the other group did not receive any BoNT-A. Participants were randomized to 1 of 2 groups, except when objections to randomization were so strong that families refused to participate. These families were offered participation in the treatment group they preferred. Power calculations were performed for the primary outcome measure gross motor function. The total sample size of 65 children was considered sufficient for the effect outcomes presented here, especially since both legs were taken into account in the analysis of bilaterally measured outcomes (if spastic).
During regular spasticity-management team consultations in 2 Dutch university hospitals and 5 rehabilitation centres, experienced multidisciplinary teams of professionals assessed children for eligibility. The main inclusion criteria were: unilateral or bilateral spastic CP in the leg(s), classified at levels I–III of the Gross Motor Function Classification System (GMFCS), age range 4–12 years, with an indication for multi-level BoNT-A treatment for mobility problems.
Written informed consent was obtained for all participating children. The ethics committee of Erasmus MC approved the SPACE BOP study, and the trial was registered in the Dutch Trial Register (NTR TC1655).
In case of randomized participation, children were centrally assigned to 1 of the 2 intervention groups and allocation was concealed until after baseline measurements. We attempted to mask the outcome assessors, the children’s physiotherapists, and those administering casting and AFO to whether or not BoNT-A was injected. After anonymization and coding, data analyses were performed by individuals not involved in the interventions or outcome assessments.
To enable a fair comparison of both costs (see (52)) and effects between the 2 intervention groups, BoNT-A treatment plans were made for each child. The need for serial casting and prescription or (re)alignment of AFOs was also determined. In the group that received BoNT-A injections, these were administered under general anaesthesia by experienced clinicians in a paediatric hospital day-care setting. Clinicians adhered to recommendations about preparations, cautions, dose modifiers, localization techniques, and safety aspects, as described in the European Consensus 2009 (5). In all cases, preparations of botulinum toxin serotype A – Botox® (Allergan Inc., Eindhoven, The Netherlands) were used, and age- and weight-related maximum allowed doses were injected. Post-injection side-effects and/or adverse events were monitored. The CR period, during which all children had iPT, started one week after BoNT-A injections.
An iPT guideline was developed. based on best-available evidence in 2010 (46, 56). During a 12-week period, the children ideally had 3 45–60 min physiotherapy sessions each week, with at least 1 rest day between sessions. Sessions were individually scheduled at the children’s special schools and/or in private practices. Because of large heterogeneity that is inherent to CP, the content of each session was individually tailored within the framework of the guideline, and strongly relied on physiotherapists’ clinical reasoning abilities. After a dynamic and playful warm-up, the main therapy components consisted of functional strength exercises and functional goal-directed activity-focused exercises. Progressive resistance exercises (PRE) were done to improve strength, based on current guidelines for typically developing children (46), and children with CP (i.e. intensity of 8–15 repetition maximum (RM)) (56). Functional goal-directed exercises were focused at the ICF activity/mobility categories, and were based on the families’ request for help. Range of motion exercises were not included in therapy sessions except for some time to explain the ”homework” (50). All involved therapists were specialized in paediatric physiotherapy. Information about therapy compliance and content of each session was obtained from the therapists’ administrations and custom-made iPT diaries. After primary end-point measurements, the physiotherapy returned to the children’s individual pre-study intensity.
In both intervention groups, 2–4 weeks of serial casting (i.e. weekly changed below-knee walking casts), starting about 1 week after the iPT period commenced, could be prescribed in cases in which passive ankle dorsiflexion with extended knee was less than 0°. The iPT sessions continued when children wore casts. If necessary, alignment of current or new AFOs was also arranged. Primary end-point measurements were performed when the 12-week iPT period had ended, and follow-up measurements were performed 12 weeks thereafter.
Intensity of current CP-related pain was reported by the children using a paediatric visual analogue scale (VAS) with emoticon faces (5-point scale).
Functional leg muscle strength was measured with a Sit-to-Stand (STS) test (57), in which the child had to attain a standing position, without using the arms and with no assistance. The starting position is on a small bench, seated with feet flat on the floor and knees flexed at 90°. The maximum number of repetitions in which the legs and hips were within 15° of the extended position within 30 s was counted. This STS test is valid and has been used before in effectiveness research (43, 49).
The guideline ”standard physical examination of children with central motor paresis” (58) was used to determine the passive range of motion (passive ROM) and angle of catch (AoC). A Lafayette goniometer was used to measure the passive ROM (in absolute degrees) during slow passive stretch as an indicator of muscle length. This was done for 8 outcome measures: hip adduction, hip abduction in flexion, hip extension while prone, knee extension, the popliteal angle of the knee, knee flexion while prone, ankle dorsiflexion with knee flexed 90°, and ankle dorsiflexion with an extended knee, for both legs in case of bilateral CP.
As an indicator of spasticity, it was assessed whether there was a catch (i.e. a sudden increase in muscle tone, considerably blocking further movement) during fast passive stretch, for both legs separately in case of bilateral CP. The AoC was noted for fast passive stretches: hip abduction in flexion (AoC adductor muscles), the popliteal angle (AoC hamstring muscles), knee flexion while prone (AoC rectus femoris muscle), ankle dorsiflexion with knee in 90° flexion (AoC soleus muscle), and ankle dorsiflexion with extended knee (AoC gastrocnemii muscles). These 5 AoC outcome measures were expressed as the number of degrees short of a physiologically normal end of range for their corresponding passive ROM (i.e. the greater the deficit, the worse the spasticity). The number of degrees short was 0° if there was no catch present.
Walking speed and kinematic gait parameters were determined from 2-dimensional instrumented gait analysis, for both legs in case of bilateral spastic CP. This was done while walking barefoot and with footwear/AFO on a 10-m walkway, while children were instructed to walk at a comfortable walking speed. Two digital cameras were used to capture sagittal and dorsal views. Passive markers were attached to relevant bony markers, and the locations of the markers were digitalized and transformed. Walking speed and 2D kinematics were determined from the 2D space calibrated middle 3 m of the walk-way. Walking speed was calculated from the sagittal spatiotemporal information of the lateral malleolus.
From the sagittal position of the markers, 4 effect outcomes were determined: the inter-segmental joint angle of the ankle during mid-stance and during mid-swing, the knee angle during mid-stance and the maximum knee angle during the swing phase (i.e. absolute joint angle).
For each kinematic gait parameter, the deviation (in °) from a physiologically normal joint-angle-range (59) was also calculated. If the absolute angle was within a certain pre-defined bandwidth, it was considered as non-deviant. In our opinion, this better reflects improvements at the group level because a shift within a physiologically normal bandwidth range should not be considered as improvement. Moreover, it better adjusts for the different pathological walking types (60).
The satisfaction of primary caregivers regarding functioning of their child in general was assessed with a VAS with scores ranging from 0 (very dissatisfied) to 10 (very satisfied). Using a second VAS with the same scoring range from 0 to 10, the child’s satisfaction with its own functioning was proxy-assessed.
Finally, goal attainment scaling (GAS) was used as an effect outcome. GAS is increasingly used in studies of BoNT-A treatment for CP (61–64), because its responsiveness is assumed to be better than that of more generic measures (7, 65–67). GAS measures the extent to which individual therapy goals are attained on a 6-point scale (–3 = deterioration; –2 = baseline score; –1 = improved but less than goal; 0=goal attained; +1 = more than goal attained; +2 = far more than goal attained). For each child, an individual ”SMART” goal (i.e. specific, measurable, acceptable, relevant and time-related goals) in the ICF activity category was set before treatment started for the treatment period up to the primary end-point at 12 weeks. The GAS scales were set in dialogue between families and physiotherapist, based on the request for help as discussed in the spasticity management consultation, and were scored by the child’s therapist at 12 and 24 weeks (with additional video check by an independent assessor not involved in any treatment modality).
First, baseline characteristics of participating children and the different treatment modalities they received in the 2 intervention groups were described and compared using conservative non-parametric tests. Subsequently, baseline comparability regarding the effect outcomes was checked in the same way.
The comparative effectiveness analyses compared treatment outcomes of BoNT-A+CR with the outcomes of only-CR to estimate differences in effect. For the randomized participants this was done according to the intention-to-treat (ITT) principle. Two separate analyses were performed to compare baseline scores with the scores at 12 weeks (primary end-point) and with scores at 24 weeks (follow-up), using linear mixed model analyses. We adjusted for the dependency of repeated observations in each subject with a random intercept, and also adjusted for the number of previous BoNT-A treatments, age and GMFCS level.
For the bilaterally measured outcome measures, in principle, both legs were included in the analyses for children with bilateral spastic CP (with an additional left/right adjustment). For muscle length, spasticity and gait, however, a leg was included in the mixed models analyses only when the child’s BoNT-A treatment plan targeted muscles or muscle groups that were expected to have an effect on that particular effect outcome. For example, if a child’s BoNT-A treatment plan targeted the gastrocnemius muscles, the leg was included only in the mixed models for the passive ROM effect outcomes knee extension, popliteal angle of the knee, knee flexion while prone, ankle dorsiflexion with knee flexed 90°, and ankle dorsiflexion with an extended knee, the effect outcome AoC for ankle dorsiflexion with extended knee, and all kinematic gait parameters. This grouping of ”targeted muscle/effect outcome – combinations” was based on expert opinion injection schemes.
Finally, because our study was not fully randomized and we also allowed participation in the treatment group that was strongly preferred by families, we adjusted for the strength of the preference. All statistical analyses were carried out using IBM-SPSS statistics 21, and p ≤ 0.05 was considered statistically significant, with no adjustment for multiple comparisons.
A total of 757 children were assessed for study eligibility between October 2009 and September 2013. Of these, 634 did not meet the inclusion criteria regarding their GMFCS level or age (see figure in Schasfoort et al. 2017 (52)). Of 123 families who were asked to participate, 65 had their child enrolled in our partly randomized study. For various reasons, 60% of the participants had such a strong preference for one of the two interventions that they had serious objections towards randomization. Only 10 families (15%) were completely neutral towards receiving one or the other intervention.
There were 37 boys and 28 girls, with a mean age of 7 years and 4 months (standard deviation (SD) 2 years, 4 months, age range 4–12 years). Fourteen participants had unilateral spastic CP subtype and 51 had the bilateral subtype; and 19, 23 and 23 children were classified as GMFCS levels I, II and III, respectively. There were no drop-outs and few missing data (see right-hand columns in Tables III and IV).
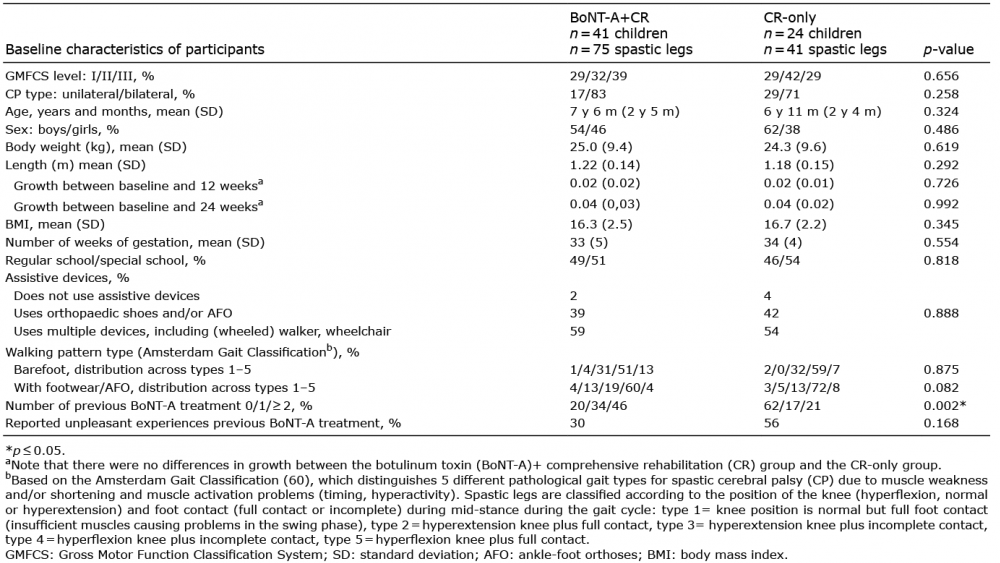
After the baseline measurements, 41 children received BoNT-A+CR and 24 children started a 12-week period of CR alone. Except for a significantly higher number of previous BoNT-A treatments in the BoNT-A+CR group (p = 0.002), there were no significant differences between the 2 intervention groups regarding patient characteristics (Table I).
Table I. Characteristics of the participants in the 2 intervention groups
Children were evenly distributed over GMFCS levels between groups. For the children who received BoNT-A, the mean dose of intramuscular BoNT-A was 9 (SD 5), 17 (SD 5) and 17 (SD 4) units per kg bodyweight for GMFCS levels I, II and III, respectively. Except for the rectus femoris muscle (p = 0.003), there were no significant differences between the intervention groups regarding the particular muscles that were targeted in the children’s prescribed BoNT-A treatment plans or the characteristics of the other treatment modalities (Table II).
Table II. Characteristics of different treatment components in the 2 intervention groups
Comparison of baseline scores for effect outcomes in the 2 intervention groups showed that the intervention groups were comparable, except for passive ROM for ankle dorsiflexion with an extended knee and the AoCs of the adductor and hamstring muscles (Tables III and IV).
Within both intervention groups, in general, changes over time for the different effect outcomes were in the same direction and of equal size between baseline and primary end-point (i.e. 12 weeks after the start of CR) (Table III). This was also the case for changes between baseline and follow-up (i.e. after 24 weeks; Table IV).
The comparative effectiveness analyses showed that there were no statistically significant differences in treatment
effect between the 2 groups at primary end-point (Table III), except for the AoC of the m rectus femoris, which was a clinically relevant difference in effect in favour of the only-CR group (12° difference between groups, p = 0.025). At follow-up, the kinematic gait parameter maximum knee angle during the swing phase while walking barefoot was the only effect outcome that showed a statistically significant and clinically relevant difference in effect in favour of the BoNT-A+CR group (6° difference between groups in favour of BoNT-A+CR, p = 0.034). However, this difference in effect was not significant with gait parameters expressed as the deviation in degrees from a physiologically normal gait range (1° difference between groups in favour of BoNT-A+CR, p = 0.510) (Table IV).
Goal attainment scaling showed similar patterns for both intervention groups (Fig. 1). There were no differences in effect between interventions at primary end-point (0.1estimated difference in favour of only-CR, 95% CI –0.71–0.93, p = 0.791) or at follow-up (0.2 difference in favour of BoNT-A+CR, 95% CI –1.13–0.75, p = 0.688).
Fig. 1. Goal attainment scaling (GAS) for individual ”SMART” goals at the ICF activity level, unadjusted mean scores at baseline, 12 and 24 weeks (SD). GAS scoring: –3 = deterioration; –2 = baseline score; –1 = improved but less than goal; 0 = goal attained; +1 = more than goal attained; +2 = far more than goal attained. SMART: specific, measurable, acceptable, relevant and time-related goals; BoNT-A: botulinum toxin; CR: comprehensive rehabilitation; SD: standard deviation.
There were no serious side-effects and/or adverse events related to BoNT-A and/or CR, but the casting periods and/or alignment of AFOs was complicated in a number of cases in both groups, mainly due to pain or pressure complaints (Table I).
In the SPACE BOP study, the added value of BoNT-A treatment preceding a period of comprehensive rehabilitation (CR) was determined in an ambulatory group of 65 children with spastic CP in the age range 4–12 years, who were equally distributed across GMFCS levels I–III. Differences in treatment effects (and costs, as described previously (52)) were studied between a group of 41 children receiving BoNT-A+CR and a group of 24 children receiving only-CR. One full treatment cycle per child was followed, with a large number of outcome measures across ICF categories: pain, muscle strength and length, spasticity, walking speed, gait characteristics, proxy-reported overall functioning, individual goal attainment, gross motor function, everyday physical activity levels, and health-related quality of life.
For the effect outcomes, gross motor function, everyday physical activity levels and health-related quality of life, it was found previously that treatment regimes with and without BoNT-A were approximately equally effective (52). For the presently described effect outcomes pain, muscle strength and length, spasticity, walking speed, gait characteristics, proxy-reported overall functioning and individual goal attainment, the findings at primary end-point in the BoNT-A+CR group were largely in accordance with previously reported findings (11, 32, 33, 68–71). However, similar results were found in the smaller intervention group that received only CR. Treatment regimes with and without BoNT-A appeared to be equally effective at the group level. Findings at 24-week follow-up also showed no difference in effectiveness between groups. Thus, at the group level, no evidence was found for the added value of BoNT-A injections when preceding CR for ambulatory children with spastic CP in the age range 4–12 years.
These results may appear to contradict previous findings, but this is not the case. When the literature is critically appraised, there are some indications that the relative contribution of factors other than BoNT-A to overall effectiveness of combined treatment packages may have been underestimated. For example, in the uncontrolled observational study by Molenaers et al. (14) in a very large group of children with CP (n = 577), all children received BoNT-A injections plus physiotherapy, plus additional casting and/or AFOs. Results showed that increased intensity of physiotherapy, post-injection casting and increased use of orthoses significantly contributed to better outcome (all p ≤ 0.005), whereas the correlation between total BoNT-A dosage and goal attainment was not significant (14). In a randomized cross-over trial by Reddihough and colleagues, the physiotherapy period intensity during the more effective BoNT-A phase and the less-effective control phase differed (mean 28 vs 21 h) (69), indicating that intensity of PT may also be an important determinant of effectiveness. It has also been reported that larger parental satisfaction in the BoNT-A intervention group was not related to improvements (thereby suggesting a possible placebo effect), and that improvement lasted longer than the pharmacological effect (4). In the 2010 international consensus statement it was acknowledged that the effects of serial casting seemed to be at least as strong, and in some studies even stronger, than the effects of BoNT-A (6). In another uncontrolled small study by Yap et al., it was found that child, family, and treatment characteristics influence the degree of responsiveness to BoNT-A treatment (plus post-BoNT interventions), and that the contribution of contextual factors may be underappreciated (72).
In short, a stronger relative contribution of factors other than BoNT-A may equally well explain improvements, especially in view of the longer-term effectiveness. Assuming a positive effect of intensity of physiotherapy, this factor cannot counterbalance a possible positive effect of BoNT-A in our study: the mean intensity of physiotherapy was similar in the period until primary end-point, and remained/was higher between primary end-point and follow-up in the group that received BoNT-A (700 min in this group vs 558 min in the only-CR group, Table II).
Since children have never been specifically excluded from regular standard care in the intervention groups in most, if not all, previous (randomized) controlled trials, conclusions regarding (especially long-term) BoNT-A effects have in fact been conclusions regarding the effects of BoNT-A plus (an)other co-intervention(s). This is especially the case in trials that focus on efficacy, safety and dosage of BoNT-A. However, efficacy and effectiveness research usually have different aims (73). The size of the contrast between intervention and comparator also differs, with generally larger contrasts in efficacy studies. Low-intensity “standard care” as comparative control intervention is, from a clinical effectiveness perspective, not the most logical choice, and may even be considered a priori inferior because they do not do justice to the current body of evidence for the non-pharmacological post-BoNT-A treatment packages for spastic CP. The comparative alternative intervention should be a full representative of best-available evidence for the non-pharmacological modalities that are applied in clinical practice to date.
As we pointed out earlier (52), up to now, research questions and designs have been based on the implicit assumption that BoNT-A is the most active component in combined treatment packages. However, given the consensus that BoNT-A should never be a stand-alone treatment and an interdisciplinary multi-modal team approach is required (5), it may, in our opinion, be likely that physiotherapy was intensified after BoNT-A treatment in the intervention groups. This cannot be checked, however, because the post-BoNT-A interventions and the interventions in the comparative intervention largely remained ”black boxes” (35). It is difficult to weigh the current body of evidence, but based on our results, the assumption that BoNT-A creates better conditions to enhance the (long-term) effectiveness of adjunctive interventions may be questioned. It should be noted that, as long ago as 2000, Ade-Hall & Moore warned about premature acceptance of BoNT-A because of inconclusive evidence (3).
The current study does not question the working mechanism or efficacy of BoNT-A. This is related to the possibility of false indications for BoNT-A treatment, even though the medical specialists involved in the current study had ample experience with BoNT-A. Clinical assessment of responses to passive muscle stretch is complicated, as it is difficult to distinguish reliably between non-neural (tissue-related) and neural (central nervous system related) contributions to hyper-resistance (74). This clearly hampers the interpretation of findings because BoNT-A can only impact non-neural contributors to hyper-resistance, whereas pathophysiological responses to stretch can have multiple causes.
Further investigations are therefore clearly warranted, and the p-values presented in this paper should be interpreted with caution because of the disturbed randomization. In future research, instrumented/quantitative assessment of different components of hyper-resistance should be applied (74). At the same time, it is important to focus on opening the black box, by defining the content of treatment in both intervention and control groups, to enable us to better determine the best intervention for each patient (13, 75).
The main limitations of the current study were its pragmatically chosen partly-randomized design, the relatively small sample size, failed masking of outcome assessor (37%) or physiotherapist (69%), and the lack of a control group without intervention. These have been discussed extensively previously (52). The potential bias related to differences in BoNT-A treatment history between groups was not evident from the data. A strength of the current study is that, in contrast to most other studies, we included both legs in the comparative effectiveness analyses for children with bilateral spastic CP (instead of only the most involved leg). This better reflects the true effectiveness of interventions for the bilaterally measured outcome measures. We agree with Ade-Hall that it is important to reflect clinical practice as closely as possible (3), and therefore only included legs in the analyses for an effect outcome when a BoNT-A-targeted muscle was expected to have an effect on that particular effect outcome according to a scheme based on expert opinion. This is debatable, of course, but in our opinion is the most valid way to evaluate the effectiveness of multi-level BoNT-A treatment. Underdosing was highly unlikely because the medical specialists applied the maximum recommended BoNT-A doses per large muscle group in relation to the age of the child.
In conclusion, at the group level, giving BoNT-A injections prior to rehabilitation did not increase the effectiveness of multimodal comprehensive rehabilitation treatment for ambulatory 4–12-year-old children with spastic CP. Since this applies to a wide range of effect outcomes across different ICF categories, it is now relevant to critically reconsider the indications for and use of BoNT-A treatment in this specific CP subgroup.
The authors greatly appreciate the Netherlands Organisation for Health Research and Development (ZonMW grant number: 170995003) and Rijndam Rehabilitation for their financial support. The authors thank SPACE BOP study group members Dr Suzanne Polinder, Dr Ewout Steyerberg, Eline Bolster, Irma Viola, Karlijn van Beek, Suzanne Lambregts and Johannes Verheijden, for their substantial contributions to this study. The authors also thank Gerard Borsboom (statistical advice); Dr Wim Hop (randomization scheme); Kim van Hutten and Mariette Koster (measurements/analyses); Dr Eugene Rameckers (iPT guideline); medical specialists in rehabilitation of VU Amsterdam, Erasmus MC Rotterdam, Rijndam Rehabilitation Rotterdam; and the secondary centres in the Amsterdam region, Revant Breda, Libra Rehabilitation & Audiology Eindhoven, De Hoogstraat Utrecht and De Trappenberg Huizen (patient enrolment), all physical therapists, casting room workers, CPOs and, finally, the participating children and their families.
Financial support: The SPACE BOP study is financially supported by the Netherlands Organisation for Health Research and Development (ZonMW grant number: 170995003) and Rijndam Rehabilitation Rotterdam, the Netherlands.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize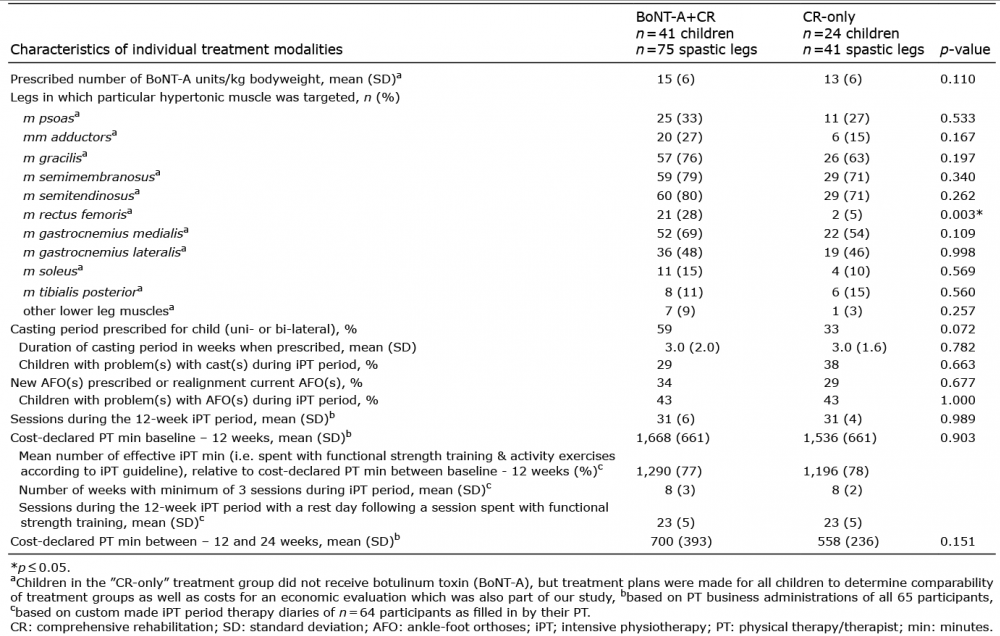 Click to show fullsize
Click to show fullsize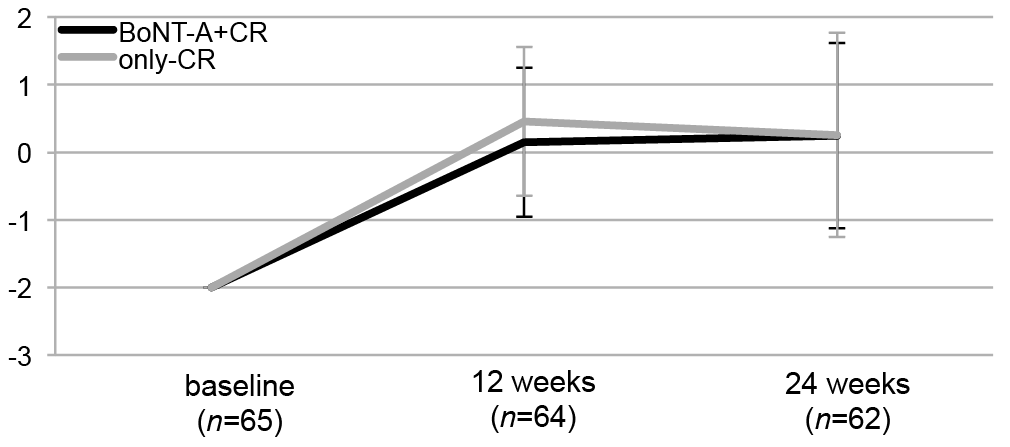 Click to show fullsize
Click to show fullsize