PHYSICAL BEHAVIOR IS WEAKLY ASSOCIATED WITH PHYSICAL FATIGUE IN PERSONS WITH MULTIPLE SCLEROSIS-RELATED FATIGUE

From the 1Department of Rehabilitation Medicine, 2Department of Biostatistics, Erasmus MC University Medical Center, Rotterdam and 3Department of Rehabilitation Medicine, EMGO Institute for Health and Care Research, VU University Medical Center, Amsterdam, The Netherlands
Background: Fatigue affects 80% of persons with multiple sclerosis and is associated with daily physical functioning. Both fatigue and physical behaviour are multidimensional concepts.
Objective: To study the association between the dimensions of physical behaviour and multiple sclerosis-related fatigue.
Methods: Cross-sectional analysis of 212 persons with multiple sclerosis. Participants were severely fatigued, with a Fatigue Severity Scale median (interquartile range): 5.4 (4.8–5.9) and were minimally to moderately neurologically impaired, based on the Expanded Disability Status Scale: 2.5 (2.0–3.5), 73% had relapsing-remitting multiple sclerosis. Fatigue was measured by questionnaires (i.e. Checklist Individual Strength, Modified Fatigue Impact Scale), and the dimensions subjective, physical, cognitive and psychological fatigue were distinguished. Physical behaviour was measured using an Actigraph GT3X+, and outcomes were categorized into the dimensions of activity amount, activity intensity, day pattern, and distribution of activities.
Results: The physical behaviour dimensions were significantly associated with only the physical fatigue dimension (omnibus F-test: 3.96; df1 = 4, df2 = 207; p = 0.004). Additional analysis showed that the amount of activity (unstandardized beta coefficient (β) = –0.16; 95% confidence interval (CI) –0.27 to –0.04; p = 0.007), activity intensity (β = –0.18; 95% CI –0.31 to –0.06; p = 0.004) and day pattern of activity (β = –0.17; 95% CI, –0.28 to –0.06; p = 0.002) were the physical behaviour dimensions that were significantly associated with physical fatigue.
Conclusion: Physical behaviour is weakly associated with physical fatigue and is not associated with
other dimensions of fatigue.
Key words: fatigue; physical behaviour; multiple sclerosis; rehabilitation.
Accepted Jun 4, 2018, Epub ahead of print Sep 5, 2018
J Rehabil Med 2018; 50: 821–827
Correspondence address: Johannes B. J. Bussmann, Department of Rehabilitation Medicine and Physical Therapy, Erasmus MC – University Medical Center Rotterdam, PO Box 2040, NL-3000 CA Rotterdam, The Netherlands. E-mail: j.b.j.bussmann@erasmusmc.nl
*This article has been handled and decided upon by Editor-in-Chief Kristian Borg
Fatigue affects many people with multiple sclerosis and is associated with daily functioning. There are several subtypes of fatigue and physical behaviour, although this is often not recognized in the literature. Therefore, we studied the associations between subtypes of fatigue and physical behaviour in a large group of fatigued persons with multiple sclerosis. Fatigue was divided into subjective, physical, cognitive and psychological dimensions, and physical behaviour was divided into the dimensions amount of activity, intensity of activity, day pattern, and distribution of activities. The results showed that physical behaviour dimensions, the distribution dimension excepted, were associated only with the physical dimension of fatigue, and not with other fatigue dimensions or total fatigue scores. The results of this exploratory study highlight the importance of more detailed assessment of both fatigue and physical behaviour in multiple sclerosis.
Fatigue affects 80% of persons with multiple sclerosis (MS) (1, 2) and occurs among all MS subtypes and disability levels (3). MS-related fatigue is defined by the Multiple Sclerosis Council for Clinical Practice Guidelines (4) as “a subjective lack of physical and/or mental energy that is perceived by the individual (or caregiver) to interfere with usual and desired activities”. From this definition, it seems plausible that MS-related fatigue is associated with daily physical functioning (1, 3) or, more precisely, with an individual’s physical behaviour (PB) (5, 6) (i.e. the body postures, movements and activities performed in daily life (7)). However, the definition of MS-related fatigue is rather general, and lacks specificity regarding different dimensions of fatigue and its consequences. Fatigue questionnaires also have this lack of specificity, as exemplified by questions such as “fatigue interferes with my daily functioning” (Fatigue Severity Scale (8)).
The complexity of the relationship between fatigue and PB is also evident from the literature. Several studies (9–18) have focused on describing the relationship between fatigue and different aspects of PB. However, overall, the evidence for the relationship between fatigue and PB, with fatigue affecting PB and/or vice versa, is weak. Furthermore, the results are conflicting, as some studies support an association, i.e. when there is more fatigue the person is less physically active (9–11), while other studies report either a weak association or none at all (12–18). Thus, there is currently no consensus about associations between fatigue and PB.
This lack of consensus may be explained by the limited attention paid to the multi-dimensionality of fatigue (1) and that of PB (7). Both fatigue and PB can be regarded as umbrella constructs that consist of several dimensions. For example, perceived fatigue consists of subjective, physical, cognitive and psychological dimensions (19). Relying on a sum score of all of these dimensions, or considering a single dimension alone, may mask the existence of any association with PB.
Similarly, PB is composed of different dimensions. Most literature has focused primarily on 1 dimension of PB, namely the “amount of physical activity” (20–23). However, it is recognized that measurement of PB should include a wide range of multidimensional measures, such as intensity, type, duration, and frequency (24, 25), as well as temporal features (26). In a previous paper from our group (5), a detailed analysis of physical behaviour showed that fatigued people with MS not only differed from healthy controls in levels of physical activity, but also in some other dimensions of physical behaviour, such as day patterns, intensity and distribution. Treatment strategies also recognize the relevance of other dimensions of PB. For example, energy conservation management (27) does not focus on total amount of activity, but aims at balancing an individual’s activities and rest so as to relieve fatigue. In this case, PB outcomes that only represent amount will not be most valid and responsive. Also, in other populations, there has been increasing interest in evaluating day patterns (morning, afternoon, evening), intensity of activity, as well as the distribution of activity and sedentary behaviour (5, 6, 28). Not recognizing the multi-dimensionality of PB may mask any potential effects or associations.
To date, only one study has investigated the relationship between fatigue and PB considering the multi-dimensional components of fatigue (17). In this study, by Rietberg et al. (17), there were no associations detected when considering the total fatigue scores; however, the physical dimension of fatigue (measured with the Modified Fatigue Impact Scale) was significantly associated with the total amount of physical activity. A β of –0.044 indicated that a 1-point increase in physical fatigue was associated with a mean decline of 5.5 min in physical activity over 24 h. However, the study did not consider the multi-dimensionality of PB.
More detailed knowledge about the relationship between MS-related fatigue and PB will provide a better understanding of the consequences of MS on daily functioning, which can be useful in designing treatment modalities. This might lead to the development of more effective interventions that are tailored to individual needs and therefore to improved rehabilitation. The aim of the present study was to explore associations between different dimensions of fatigue and PB in ambulatory persons with MS-related fatigue.
The study population consisted of people with MS who were included (until March 2014) as participants in the Treating Fatigue in MS with Aerobic Training, Cognitive Behavioral Therapy and Energy Conservation Management (TREFAMS-ACE) research programme (29). This research programme consisted of 3 multi-centre randomized controlled trials (RCTs), which evaluated the effectiveness of rehabilitation interventions on fatigue and participation in patients with MS. The inclusion criteria in this research programme were as follows: definite diagnosis of MS; severe fatigue, as indicated by a score of ≥35 on the fatigue domain of the Checklist Individual Strength (CIS20r); ambulatory status (i.e. Expanded Disability Status Scale (EDSS) ≤ 6.0; no diagnosis of depression (i.e. Hospital Anxiety and Depression Scale (HADS) < 11); no initiation or change to pharmacological treatment for fatigue during the previous 3 months; and age 18–70 years. The protocol for this study was approved (NL number 33451.029.10; METc VUmc.nr 2010/289) by the Medical Ethics Committee of VU University Medical Center, Amsterdam, The Netherlands. Details of the TREFAMS-ACE study have been described elsewhere (29). All participants provided written informed consent. An additional inclusion criterion for the present study was the availability of baseline accelerometer data.
Fatigue was measured with 2 self-reported fatigue questionnaires that cover different dimensions of fatigue (30). The Checklist Individual Strength (CIS20r) (31) is a multi-dimensional questionnaire that consists of 20 items, rated on a 7-point scale. The CIS20r is divided into 4 dimensions of fatigue and related behavioural aspects: the subjective experience of fatigue (8 items); reduction in motivation (4 items); reduction in physical activity (3 items); and reduction in concentration (5 items). The CIS20r focuses on fatigue experienced in the previous 2 weeks. The CIS20r has several reliable psychometric properties, such as good internal consistency and test-retest reliability for total scores and dimensions scores, as well as good construct and concurrent validity. Furthermore, the multi-dimensional construct is supported by factor analysis (19, 32). The Modified Fatigue Impact Scale (MFIS) (33) is a multi-dimensional questionnaire that consists of 21 items, rated on a 5-point Likert scale. MFIS assesses the perceived impact of fatigue on 3 dimensions: physical (9 items), cognitive (10 items) and psychosocial (2 items) functioning during the previous 4 weeks. The MFIS is frequently used in MS research and has been shown to have good test retest reliability on the total and domain scores, as well as good construct and concurrent validity. The multi-dimensional structure has also been confirmed (19, 33). For both questionnaires, higher scores reflect more fatigue.
The assessment of PB was conducted in the participants’ daily environment using 3-dimensional accelerometry (ActiGraph GT3X+ modela; 4.6 × 3.3 × 1.5 cm; 19 g). This device is valid and reliable in measuring PB in persons with MS (34). Participants wore the accelerometer on an elastic belt around their waist during waking hours for 7 days and were requested to remove it only during water-based activities, such as showering or swimming. Accelerometer signals were sampled with 30 Hz and downloaded using an epoch length of 10 s and the low-frequency extension (LFE) option in Actilife software (v. 6.6.2). Activity counts from all 3 axes, i.e. the vector summed value known as “vector magnitude” (VM), were calculated. For every ActiGraph, a compliance and control quality check was performed once data were downloaded. Non-wear periods were defined as a 180-min (or longer) period of continuous zero counts without allowing for interruption and were filtered from the raw data using a semi-automated algorithm and excluded from further analyses. Days with at least 660 min of wear time were considered valid. For data to be included in the analysis, at least 5 valid measurement days were required (35). From Actilife the data were imported into Microsoft Excel for each person separately; additional calculations on bouts and cut-points were performed using Microsoft Excel and MATLAB.
Four dimensions of fatigue were derived from 7 subscales of the 2 fatigue questionnaires (CIS20r and MFIS) (see Table II). The 4 dimensions were categorized by maintaining the original subscales and combining the subscales of the 2 fatigue questionnaires of items that were conceptually similar. This was tested by examining the relationships such that the subscales were moderately (r > 0.3) (physical and psychological) or highly (r ≥ 0.8) (cognitive) correlated. The 4 dimensions are as follows: (i) Subjective fatigue: CIS subjective fatigue score; (ii) Physical fatigue: CIS physical activity scores and MFIS physical scores; (iii) Cognitive fatigue: CIS concentration scores and MFIS cognitive scores; (iv) Psychological fatigue: CIS motivation scores and MFIS psychosocial scores.
PB variables were selected based on the results of a previous study by Blikman et al. (5). In the present study, 10 PB variables (see Table II) were categorized into 4 PB dimensions: (i) Amount of activity: the amount of daily activity of a person based on the activity expressed in total counts per day and counts per minute. Higher amounts of activity are assumed to be beneficial. (ii) Intensity categories: the time spent in different intensity categories as a percentage of the total wear time per day. Percentages were calculated for the time spent in sedentary activities (0–150 counts), light physical activity (151–2,690) and moderate-to-vigorous physical activity (MVPA) (> 2,691) (36). More time spent in higher intensity categories is assumed to be beneficial from the perspective of functioning and health (i.e. less sedentary, more light and more MVPA). (iii) Day patterns (5): how the amount of activity is spread over the day (morning, afternoon and evening period). Based on previous research (5), we reported the outcome as a “day pattern ratio”, which was calculated by counts per minute in the evening (06.00 to 12.00 h) divided by counts per minute in the morning (05.00 to 12.00 h). We assume, that a higher (or equal) ratio express a higher amount of remaining capacity to be active during the evening, which can be considered to be beneficial. (iv) Distribution: distribution outcomes are based on the analysis of bouts: a consecutive time period of a defined activity. For this paper, the defined activities were sedentary behaviour and MVPA; thus we studied the distribution of both sedentary behaviour bouts and MVPA bouts. The distribution outcomes that were calculated were the “Fragmentation index”(37) and the “Gini index”(38). The Fragmentation index is calculated as the number of bouts divided by the summed duration of all bouts. A higher Fragmentation index indicates that time spent in an activity is more fragmented with shorter bouts. The Gini index reflects the pattern of accumulation of these bouts. The Gini index ranges from 0 to 1, where a Gini index score near 1 indicates that the summed time is composed of longer periods rather than short periods. A lower Gini index reflects a situation in which there are a larger number of periods of different lengths, with a dominance of short periods. The clinical interpretation differs between sedentary behaviour and MVPA. For sedentary behaviour a higher sedentary Fragmentation index (i.e. sedentary behaviour is alternated more frequently) and a lower sedentary Gini index (i.e. the amount of sedentary behaviour dominantly results from short sedentary bouts) is assumed to reflect better functioning. While the opposite (i.e. a lower Fragmentation index and a higher Gini index representing better functioning) applies to MVPA behaviour.
Prior to statistical analysis, the standardized values (z-scores) of the baseline fatigue and PB variables were calculated by SPSS, resulting in a distribution with a mean of zero and a variance of one. After standardization, a lower z-value related to fatigue implied less fatigue, and a higher z-score for PB indicated a more beneficial type of PB. The standardized values of the variables within 1 dimension were averaged for each individual. Standard linear regression analysis was used to assess the association between the standardized dimensions of PB as the independent variables in the model and the standardized dimensions of fatigue as the dependent variables. A negative β regression coefficient indicated that, per unit increase in the standardized PB dimension, the standardized fatigue dimension was reduced by the amount of β, and vice versa for a positive β. Assumptions of normality, heteroscedasticity and multicollinearity were graphically checked using residual plots. First, 4 regression models were used, each focusing on 1 of the fatigue dimensions, while including the whole set of PB dimensions simultaneously. When evaluating the results of the linear regression analyses, we used the omnibus F-tests to investigate whether at least one of the 4 PB dimensions was significantly associated with a specific fatigue dimension. If this test was significant, additional analyses were conducted to determine which of the specific PB dimensions were significantly associated with the fatigue dimension under study. Subsequently, we also performed the same analyses after adjusting for age and sex. In addition to the fatigue dimensions, we studied the association between the PB dimensions and fatigue total scores (i.e. CIS total, MFIS total) to compare the findings resulting from the fatigue total scores and fatigue dimensions. SPSS version 21 was used for data analysis. Descriptive data are presented as the median (interquartile range; IQR) or as otherwise indicated. The significance level was set at p < 0.05. Additional analysis adjustments were made for multiple comparisons.
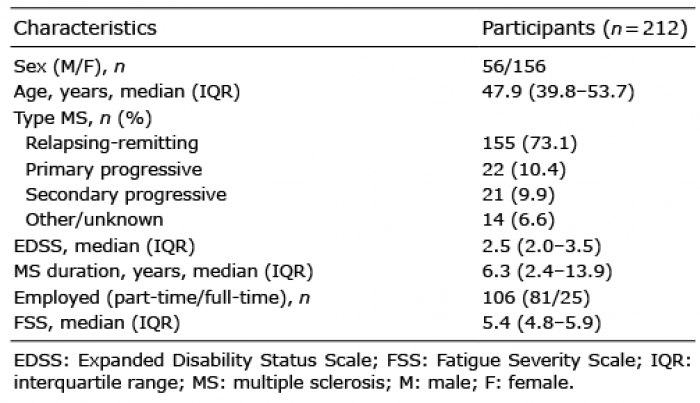
Initially, 222 baseline accelerometer data files of participants were available. Ten data files were excluded because they did not meet the inclusion criteria for valid measurements (i.e. over 5 valid measurement days). Ultimately, baseline accelerometer data from 212 persons with MS were available for analysis. The mean number of valid days was 6.7, and the mean wear time per day was 904 min. The participant characteristics are shown in Table I.
Table I. Participant characteristics
The participants with MS were severely fatigued, as defined by the fatigue domain of the CIS20r (inclusion criteria) and the Fatigue Severity Scale (39), and their EDSS scores showed minimal to moderate neurological impairments. In addition, 73.1% of participants had relapsing remitting MS. The mean and range of the original non-standardized PB variables and fatigue variables are shown in Table II.
Table II. Characteristics of the physical behaviour and fatigue variables
The omnibus F-test of the standard linear regression analysis showed that at least 1 PB dimension was significantly associated with the physical fatigue dimension (omnibus F-test: 3.96; df1 = 4, df2 = 207; p = 0.004), while no associations were found with subjective fatigue (omnibus F-test: 1.48; df1 = 4, df2 = 207; p = 0.210), cognitive fatigue (omnibus F-test: 1.06; df1 = 4, df2 = 207; p = 0.379) and psychological fatigue (omnibus F-test: 1.00; df1 = 4, df2 = 207; p = 0.409). In addition, no associations were found with the total scores of fatigue (CIS20r total p = 0.165; MFIS total p = 0.398).
Additional analyses focusing on which PB dimensions were significantly associated with physical fatigue revealed that the PB dimensions amount of activity, categories of intensity and day pattern were negatively associated with physical fatigue (Table III), while this was not the case for the distribution dimension. This means that persons with lower scores of physical fatigue have higher amounts of physical activity, spent more time in MVPA and less time in sedentary behaviour, and spread their activities more equally over morning and evening, or are more active in the evening. Comparable associations were found after adjustments for age and sex (Table III).
Table III. Four unadjusted and adjusted linear regression models with physical fatigue as the dependent variable and with each physical behaviour dimension separately as the independent variable
This study examined associations between dimensions of fatigue and dimensions of physical behaviour in a sample of 212 persons with severe MS-related fatigue. To our knowledge, no study has examined this relationship while taking into account the multi-dimensionality of both constructs. The results of our study show that physical behaviour dimensions are only associated with physical fatigue, and not with other fatigue dimensions and total fatigue scores. This conclusion can be drawn for 3 out of 4 dimensions of physical behaviour, i.e. the total amount, the intensity, and the day pattern of activities, while the distribution dimension was not related to physical fatigue. It has to be noted, however, that only a small proportion of the variance in physical fatigue was explained by the variance in physical behaviour.
The specific associations between physical behaviour and fatigue found in our study may lead to new perspectives on the treatment of fatigue in people with MS. The results of our study do not allow any causal statements, but do support the further exploration of treating physical fatigue by changing physical behaviour, e.g. by increasing the activity amount, making changes in the time spent in intensity categories (i.e. less sedentary and more light or MVPA intensity activities) or by balancing the day pattern of activities (i.e. equally spreading activities over morning and evening or increasing the level of activity in the evening). However, as indicated by the small explained variance, the clinical impact of changing physical behaviour to decrease physical fatigue may be small.
In a previous study we compared physical behaviour outcomes and dimensions between fatigued patients with MS and healthy comparison subjects (5). Although there were some differences between outcomes, the overall conclusion of that study was that these groups differed in physical activity level, and in other physical behaviour dimensions, such as day patterns, intensity, and distribution. The results of the current study are different with respect to the absence of a relationship between the distribution dimension of physical behaviour and the physical dimension of fatigue. Together with the previous findings this indicates that distribution, as expressed by the Gini and Fragmentation index, is affected in fatigued patients with MS, but not related to fatigue. In general terms: compared with healthy controls fatigued people with MS tend to have longer bouts of sedentary behaviour and shorter bouts of MVPA, but persons with MS with more fatigue do not have longer bouts of sedentary behaviour and shorter bouts of MVPA than persons with MS with lower levels of fatigue. This suggests that fatigued people with MS do distribute their periods of activity and rest differently from healthy controls, but also that changing distribution is not a primary adaptation strategy to fatigue.
None of the physical behaviour dimensions was associated with the total scores of the fatigue questionnaires. Similar results were reported by Rietberg (17), who showed that an analysis of the total scores of fatigue measures yielded no associations, whereas the physical dimension of fatigue was associated with the total amount of physical activity, one of our components of physical behaviour. Both our study and the study of Rietberg (17) suggest that the fatigue dimensions are distinct from each other and different from the total fatigue scores, which has also been concluded by other studies investigating measurements of fatigue (19, 40). This finding suggests that fatigue dimensions should be used separately in both research and clinical practice, and that the sum scores should not solely be relied on. In addition, our results also support the importance of studying physical behaviour in more detail (5), e.g. when treating patients with MS or studying the effectiveness of rehabilitation, otherwise important effects may be missed.
Although there was a significant negative association between the dimensions of physical fatigue and physical behaviour (i.e. more fatigued persons have a less active physical behaviour), these associations were nonetheless weak. A possible explanation may be that most of the participants included in this study were severely fatigued, with a relatively small range in fatigue scores. In studies that focus on relationships between outcomes, a large between-subject range in outcomes will more easily result in significant results. The weak relationships must therefore be considered in this perspective, and we propose future studies with a more heterogeneous population with respect to fatigue. Such studies may provide further insights into relationships between fatigue and physical behaviour.
Rietberg et al. (17) showed that stronger associations between fatigue and physical behaviour became evident after adjusting for patient characteristics, such as age, MS type, anxiety and depression. In our population, fatigue was present in all types of MS and independent of MS duration. We therefore had not selected these as possible confounders. Furthermore, adjusting for depression was unnecessary because a diagnosis of depression was an exclusion criterion in the present study. In our study, age and sex did not bias the association between physical behaviour dimensions and physical fatigue, and minimally altered the adjusted β values.
The present study has some limitations. Firstly, we have already discussed the relatively small range in fatigue scores of the subjects, which is the result of the inclusion criteria of the RCTs from which the data of the current study were used. Secondly, causal relationship cannot be determined using a cross-sectional study design. Specifically, while changes in physical behaviour may influence fatigue, the converse may also be true. For example, Rietberg et al. (17) studied the association between physical behaviour and fatigue and defined fatigue as the independent variable. Thirdly, our sample consisted of fatigued and ambulatory persons who were enrolled in a RCT study, most of whom had relapsing-remitting MS with minimal to moderate neurological impairment and no evidence of depression. These criteria limit the generalizability of our findings to all persons with MS. Fourthly, accelerometers have limitations, for example difficulty with measuring low activity patterns, which in our GT3X model was improved with the low-frequency extension filter; however, the validity of this filter is still insufficiently shown. Also different processing techniques (e.g. wear-time, cut-points) for accelerometers can influence the outcomes (41). We therefore clearly described our data-processing settings, which were appropriate at the time of our analysis. However, as activity monitor technology and protocols are rapidly changing, other data processing settings could become more suitable. Finally, the fatigue and physical behaviour measurements were not assessed across exactly the same period of time. Fatigue questionnaires were most often completed one week before the activity monitor measurement. However, the fatigue questionnaires measured fatigue over the previous 2 (CIS20r) or 4 weeks (MFIS) and gave a good indication of the level of chronic fatigue generally experienced by persons with MS. Although fatigue fluctuates between days, participant scores on these questionnaires are likely to remain stable. Therefore, we would not expect associations to be different if the measurements had been conducted in the same week.
In conclusion, in ambulatory persons with MS-related fatigue, a weak association was found between physical fatigue and several physical behaviour dimensions. The results indicate that more fatigued persons have a less optimal physical behaviour. The results subscribe the importance of considering specific fatigue and physical behaviour dimensions in addition to the total scores when treating patients with MS or studying the effectiveness of rehabilitation interventions. However, our study was explorative and the associations found were weak. Overall, we conclude that the clinical impact of changing physical behaviour to decrease physical fatigue may be small.
The authors would like to thank Martin Heine and Lizanne van den Akker for their contribution to this article by sharing their baseline TREFAMS RCT data. Trial registrations: ISRCTN69520623, ISRCTN58583714, and ISRCTN 82353628.
The study was performed on behalf of the Treating Fatigue in Multiple Sclerosis: Aerobic Training, Cognitive Behavioural Therapy, Energy Conservation management (TREFAMS-ACE) Study Group. The TREFAMS-ACE Study Group: V. de Groot and H. Beckerman (programme coordination), A. Malekzadeh, L. E. van den Akker, M. Looijmans (until September 2013), S. A. Sanches (until February 2012), J. Dekker, E. H. Collette, B. W. van Oosten, C. E. Teunissen, M. A. Blankenstein, I. C. J. M. Eijssen, M. Rietberg. V. U. University Medical Center, Amsterdam; M. Heine, O. Verschuren, G. Kwakkel, J. M. A. Visser-Meily, I. G. L. van de Port (until February 2012), E. Lindeman (until September 2012), Center of Excellence for Rehabilitation Medicine, University Medical Centre Utrecht and Rehabilitation Centre, De Hoogstraat, Utrecht; L. J. M. Blikman, J. van Meeteren, J. B. J. Bussmann, H. J. Stam, R. Q. Hintzen. Erasmus MC, University Medical Center, Rotterdam; H. G. A. Hacking, E. L. Hoogervorst, S. T. F. M. Frequin. St Antonius Hospital, Nieuwegein; H. Knoop, B. A. de Jong (until January 2014), G. Bleijenberg (until April 2012). University Medical Center St Radboud, Nijmegen; F. A. J. de Laat, Libra Rehabilitation Medicine & Audiology, Tilburg; MC Verhulsdonck, Rehabilitation Center, Sint Maartenskliniek, Nijmegen; EThL van Munster, Jeroen Bosch Hospital, Den Bosch; C. J. Oosterwijk, G. J. Aarts (until March 2013). Dutch patient organization, Multiple Sclerosis Vereniging Nederland (MSVN), The Hague.
Information on author access to data. Lyan J. M. Blikman had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. For access to the data used in this paper, please contact J. B. J. Bussmann.
Role of funding source. This study was part of the Dutch TREFAMS-ACE research programme and was financially supported by Fonds NutsOhra grant number (ZonMw 89000005). The funder of the study had no role in design and conduct of the study, data collection, data management, data analysis, data interpretation, preparation and writing of the manuscript, nor in the approval of the manuscript and the decision to submit the manuscript for publication.
Suppliers. a. ActiGraph, 48 E. Chase Street, Pensacola, FL 32502, USA. http://www.actigraphcorp.com/products/.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize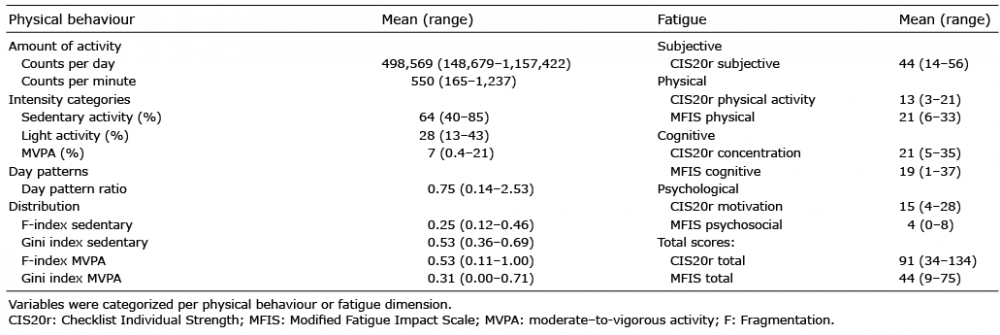 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize