
From the 1Graduate School of Medical Technology and Health Welfare Sciences, Hiroshima International University, Hiroshima, and 2Obstetrics and Gynecology, Nakagawa Clinic, Hiroshima, Japan
Background: To determine the effects of a pelvic realignment device-aided exercise programme after childbirth. Postpartum low-back pain and pelvic girdle pain often occur due to pregnancy and childbirth. Pelvic stabilization exercises are considered effective for reducing these symptoms. However, such exercise might be more effective if the sacro-iliac joints were held in optimal conformity. There is no published evidence regarding the use of a pelvic realignment device during stabilization exercises.
Methods: This randomized controlled trial involved 2 interventions and a control group. Pregnant women were allocated randomly to: (i) exercises with a pelvic realignment device (group R, n = 25); (ii) stabilization exercise (group E, n = 25); or (3) a control group (group C, n = 25). Pain intensity (visual analogue scale) and limitations in activities of daily living (pelvic girdle questionnaire) were measured 11 times during the 3-month period after delivery. A Kruskal–Wallis test was used for statistical analyses.
Results: Seventy-five pregnant women (mean age 31.2 years) participated in the study. At 13 weeks after delivery the pelvic girdle questionnaire score in both groups and visual analogue scale score in group R had decreased significantly. However, group E did not present with pain reduction at 13 weeks (p = 0.058). No significant differences were found between groups R and E (p = 0.66). The immediate and short-term effects of exercise with a pelvic realignment device showed greater improvements compared with pelvic stabilization exercises alone.
Conclusion: Standing exercises with a pelvic realignment device had immediate and short-term effects on improvement in pain within 4 weeks after delivery. The realignment device may be useful for reducing mechanical stress during exercises for postpartum low-back and pelvic girdle pain.
Key words: pelvic girdle pain; low-back pain; postpartum women; pelvic realignment device.
Accepted Aug 2, 2018; Epub ahead of print Sep 28, 2018
J Rehabil Med 2018; 50: 00–00
Correspondence address: Kazuyoshi Gamada, Graduate School of Medical Technology and Health Welfare Sciences, Hiroshima International University, 739-2631 Hiroshima, Japan. E-mail: kazgamada@ortho-pt.com
After childbirth, more than 30% of women have pain in the back of the pelvis. Pelvic stabilization exercises are recommended to reduce pain and improve functioning. The aim of this study was to determine whether use of a pelvic realignment device (PRD) during standing exercises can further improve pelvic pain after childbirth. We hypothesized that the device would improve pain reduction within 4 weeks after delivery compared with exercise alone. This study measured 75 women from day 1 to 12 months after childbirth. The women were divided into 3 groups: (i) 25 performed pelvic stabilization exercises with the PRD; (ii) 25 performed pelvic stabilization exercises alone; and (iii) a control group of 25 performed no pelvic exercise. Exercises with the PRD had immediate and short-term effects on improvement in pain within 4 weeks. Therefore, a pelvic exercise programme with PRD is recommended for reducing pelvic girdle pain after childbirth.
Pain in the area of the sacroiliac (SI) joints and pubic symphysis is common after childbirth (1). Continuous low-back pain (LBP) and pelvic girdle pain (PGP) can affect quality of life, infant rearing, and family economics among women after childbirth. More than 30% of pregnant women experience pregnancy-related LBP/PGP (2). The pain may lead to depression and difficulties in infant rearing (3, 4). Over 60% of women have difficulty in working and healthcare sought (5). Risk factors for such pain may include a history of low-back and pelvic pain before pregnancy, age, parity, body mass index (BMI), education, and satisfaction with work (3, 6, 7). Weakness of the hip extensors (8), pelvic floor muscles and transverse abdominal muscles (6, 9, 10) are associated with PGP. Moreover, pelvic instability (8), asymmetry of the SI joints and ligament relaxation (11), and insufficient and asymmetrical compression of the SI joints (12) are associated with continuous PGP after delivery. Therefore, both muscle dysfunction and pelvic malalignment should be addressed in order to prevent sustained pain.
Treatments for PGP after childbirth include exercises, individual physical therapy, massage, the intra-articular block injection, acupuncture, information, and use of a pelvic belt (13). The European guideline for treating pregnancy-related pelvic pain recommends stabilization exercises that include dynamically controlling the lumbar segments and pelvic joints by activating the local and global muscles together (13). In particular, this guideline recommends improving the role of the pelvic anatomical structures responsible for stabilization, such as the ligaments, mono- and polyarticular muscles and fascia. The joint reaction force is determined by the position of the joint and the level of tension of the muscles and ligaments (14, 15). In addition, stability requires motion control of the pelvic joints, which allow loads to be transferred and movement to be smooth and effortless (13). Many studies have examined the effects of a stabilization exercise programme involving training of the pelvic floor and abdominal muscles to increase compressive forces in the SI joints (8, 10, 14, 16, 17). Some studies have shown positive results on pain reduction (17–19). However, there is room for improvement due to: (i) unsatisfactory results in more than 6–40% of women (20–22); (ii) the long time (4–12 weeks) required to achieve pain reduction (23); and (iii) lack of evidence of the effects of stabilization on the alignment and conformity of the SI joints (24). It is assumed that adequate conformity of the SI joints can play a role in reducing mechanical stress on the ligaments and muscles around the joints. This leads us to question whether realignment of the SI joints is effective in reducing PGP. However, the role of realignment of the SI joints has not been fully understood and the effects of pelvic realignment have not been studied (25). The aim of the current study was therefore to determine the effects of an exercise programme with device-aided pelvic realignment of the SI joints immediately after delivery.
The study protocol was approved by a local ethics review board in Japan (IRBN 14-140, 2015). All participants signed a consent form prior to enrollment. Inclusion criteria were: healthy pregnant women aged between 20 and 40 years, who were having unmedicated vaginal delivery; child and mother were sufficiently healthy that the mother could care for her newborn from the next day after childbirth. The subjects did not have PGP. Exclusion criteria were: women who had a caesarean section; health problems excepting PGP; difficulty in activities of daily living (ADL); communication disorders; mental and physical disabilities.
Participants were recruited at a single obstetrics and gynaecology clinic while they were pregnant. The total number of participants was 75. A power analysis using G*Power software required a sample size of 42 to detect the difference between 3 groups using 1-way analysis of variance (ANOVA) assuming 80% power at a significance level of 5%.
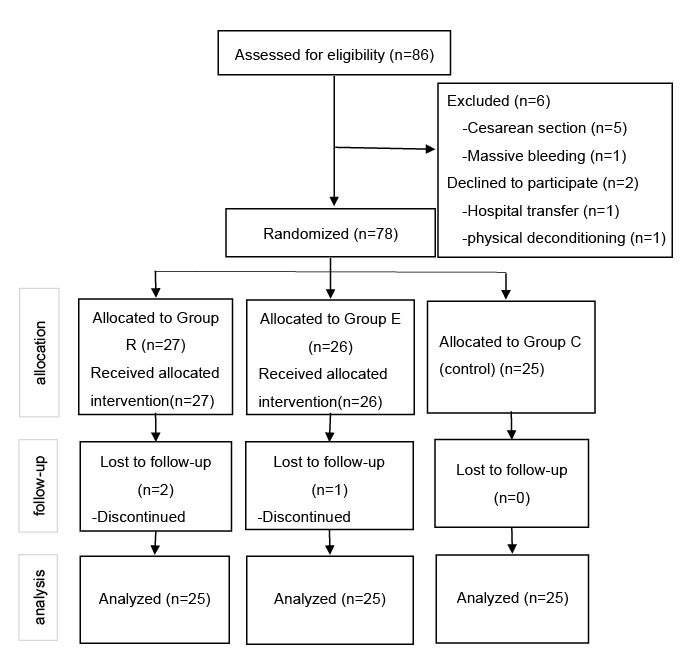
A total of 86 pregnant women were recruited during pregnancy at Nakagawa Clinic in Hiroshima, Japan. Seventy-eight subjects were allocated randomly to 3 groups: (i) group R (n = 27) performed exercises with a ReaLine® CORE (RLC) (GLAB Corp., Hiroshima, Japan) device; (ii) group E (n = 26) performed pelvic stabilization exercises; and (iii) group C (n = 25), with no intervention, served as a control group (Fig. 1). Participants’ characteristics are summarized in Table I.
Fig. 1. Flow diagram for the phases of a parallel randomized trial of 3 groups.
Table I. Characteristics of the study population
Group R performed an exercise programme using ReaLine® CORE, a belt-like device with a rigid front frame with 2 belts and 2 pairs of ratchets for attaining a more symmetrical pelvis. The device is designed to make the pelvis symmetrical and stable by applying focal forces on both anterior superior iliac spines (ASISs) and compressive forces on the SI joints while the subject is performing standing exercises for the hips and spine. The device was attached to the pelvis and shifted in the superior direction so that the top belt was located over the ASISs. The belts were tensioned using ratchets. The back frame is designed to be bent so that it compresses the SI joints. By increasing the tension of the belts, the ASISs were compressed by the rigid front frame and a greater force was applied to the ASIS of the innominate through anterior rotation. The asymmetry of the force on the ASISs becomes more equal after a few seconds of standing exercises, indicating that the innominates become more symmetrical. The RLC exercises consisted of: (i) stepping, (ii) pelvis shifting, (iii) pelvis rotation with knee extension, (iv) pelvis rotation with knee flexion, and (v) trunk flexion and extension, served as a control group (Fig. 2). These exercises took a maximum of 10 min per session and were performed twice a day for 4 weeks after delivery.
Fig. 2. Exercise protocol with ReaLine® CORE (RLC) (GLAB Corp.)
Group E performed an evidence-based stabilization programme proposed by European guidelines for postpartum PGP. The stabilization programme was divided into 3 parts, comprising: (i) isolated voluntary contraction of the pelvic floor muscles; (ii) a pelvic-tilt exercise with voluntary contraction of the pelvic floor muscles; and (iii) exercises involving hip extension, hip abduction, and abdominal crunches. Subjects performed (i) and (ii) during the first 2 weeks after delivery during the repair process of the uterus and perineum tissues, and (i)–(iii) for the remaining intervention period for 2 weeks. The stabilization exercises were repeated 10–20 times per session, and were performed twice a day for 4 weeks after delivery. According to the European guidelines for postpartum PGP, improvement in force closure, with co-ordination of the local and overall muscle system and control of a neutral position of the lumbo-pelvic region are recommended to develop strength and endurance of physical demands in order to prevent and ease pain after delivery (26). In addition, stabilization of the SI joints is essential for developing pelvic girdle control and stability (26). Thus, adequate information about pelvic control was provided.
The control group C did not receive any exercise programme. Their natural recovery was observed for comparison with the 2 exercise groups.
This study involves a 4-week intervention and 9-week follow-up period (Table II). Groups R and E were provided with different instructions during days 1–5. The intervention programmes started on the day following delivery (day 1) under the supervision of a trained instructor and a physical therapist (AS) with 15 years of experience. She instructed each subject in the exercises for the first 4 days, until discharge on day 5. After discharge, participants in groups R and E continued the exercises by themselves at home until week 4, followed by 9 weeks of follow-up. Subjects received exercise guidebooks and 10-min instruction videos on YouTube. The home exercises were the same as the ones given in the clinic. Recruitment to the study started on 1 April 2015 and the 3-month follow-up finished on 30 May 2017.
Outcomes were measured after delivery on days 1 to 5 and weeks 1, 2, 3, 4, 9 and 13 (Table II). All participants completed a baseline questionnaire about demographic data, including number of deliveries, history of low back and pelvic pain before and during pregnancy, and birthweight of the baby (Table II). They also answered questions on pain intensity and limitations in ADL, such as standing, sitting and walking during pregnancy, using a standard 100-mm visual analogue scale (VAS) and pelvic girdle questionnaire (PGQ), respectively (27). The PGQ was translated into Japanese using a cross-cultural adaptation study method (28). The reliability and validity of the PGQ Japanese (PGQ-J) version was high (Cronbach α 0.968, and interclass correlation coefficient 0.79) (personal communication).
Table II. Study protocol
An exercise journal was provided to help participants understand the protocol. Participants were contacted by telephone, text (SMS) or e-mail after discharge to remind them about the intervention and outcome measurements. They were provided with documents and pre-paid envelopes to return the forms by post on each measurement day.
Sample size was analysed with G*power software prior to starting the study. The number required for this study was a minimum of 42 participants (α = 0.05, β = 0.8). SPSS Statistics, version 24 (IBM Co.) software was used for data analysis. The demographic data for the 3 groups were compared for similarity of prognostic indicators and for initial values of outcome measures. All outcome measurements were analysed by Shapiro–Wilk test. Changes in the outcomes within each group were tested with the Friedman test. Kruskal–Wallis test was used to compare the effects of exercise between groups. α = 0.05 was used to detect a statistically significant difference.
Before delivery a total of 86 pregnant women, recruited of a single obstetrics and gynaecology clinic, agreed to participate in the study. After childbirth all participants were assessed for eligibility and 6 were excluded. Of the 6 excluded women, 5 had a caesarean section and 1 had massive bleeding during delivery. Following childbirth, 2 women declined to participate in the study: 1 was transferred to another hospital due to the emergency condition of her newborn and 1 had severe physical deconditioning. Thus, a final total of 78 subjects were divided randomly into 3 groups. A third party selected the number for each subject for random allocation. There were no significant differences between the characteristics of participants in the 3 groups. Three participants (2 in group R and 1 in group E) dropped out on week 1 after childbirth because they were too busy looking after their babies (Fig. 1). Thus, a final total of 75 subjects completed the study. There were no adverse events during intervention and follow-up.
The PGQ on week 13, after 4 weeks of intervention and 9 weeks of follow-up, showed a reduction in pain in all 3 groups (Table III). Although groups R and E demonstrated a significant reduction in pain, there were no significant differences in group C between day 1 and week 13 (p = 0.85). Between-group comparisons of PGQ demonstrated no differences between the 3 groups (p = 0.42).
Table III. Changes in pelvic girdle questionnaire (PGQ) score during the 4-week intervention and 9-week follow-up period
Results of the VAS at week 13, after a 4-week intervention and 9-week follow-up period, showed significant reductions in pain in all 3 groups (Table IV). The VAS score in group R decreased significantly at week 13 (p = 0.043). However, the VAS score in group E did not (p = 0.058). A between-group comparison of VAS using one-way ANOVA demonstrated no differences between the 3 groups (p = 0.328). The pain reduction in group R was greater than in group C (p = 0.030). There were no significant differences between groups E and C (p = 0.12) and between groups R and E (p = 0.66).
Table IV. Changes in visual analogue scale (VAS) score (mm) during the 4-week intervention and 9-week follow-up period
Immediate effects during the 4-week intervention period after delivery were in favour of group R. The immediate effect on VAS for groups R and E were 8.1 mm (95% confidence interval (95% CI) 5.4, 10.9) (p = 0.017) and 2.9 mm (95% CI 1.1, 4.7) (p = 0.19), respectively. However, there were no significant differences between groups (p = 0.21).
The aim of this study was to determine the effects of an exercise programme with RLC immediately after delivery. The main findings were that both the RLC exercise programme (group R) and stabilization exercises (group E) were effective in the short-term, resulting in reduction in pain in VAS and PGQ scores at week 13, with an intervention period of 4 weeks and a follow-up period of 9 weeks. In addition, RLC (group R) demonstrated a greater immediate effect on the reduction in VAS score than the stabilization exercise group (group E) during the 4-week period after delivery. There were no differences between the 2 exercise groups in the number of childbirth, while the median of parity in the control group was greater than those of the 2 exercise groups. Kovacs et al. (7) concluded that the number of previous pregnancies and number of children were not factors affecting LBP and PGP during pregnancy. Thus, the differences in the median of parity in this study would not have caused sampling bias. The current study targeted only healthy Japanese postpartum women who experienced unmedicated vaginal delivery, which may limit the generalizability of the results.
The short-term effects of stabilization exercises are controversial. Mens et al. (29) found no differences in peripartum pelvic pain between an exercise group performing diagonal trunk muscle exercises and a control group. On the other hand, Stuge et al. (18) found that specific stabilizing exercise for 20 weeks postpartum was more effective than general care including massage, relaxation, joint mobilization and strengthening exercises. Moreover, a longer-term intervention study with a 2-year follow-up showed that a specific stabilization exercise was more effective than a control group (30). A systematic review of 5 selected studies on the effects of an exercise programme for postpartum pain, involving an intervention period of between 4 and 20 weeks, concluded that the exercises were effective (31). Gutke et al. (32) found that stabilization exercises and a pelvic belt improved ADL ability and pain intensity, but it took more than 3 months of intervention to detect the differences. In the present study, the intervention period was only 4 weeks, which is shorter than in the previous studies, and both RLC and stabilization exercises significantly improved pain. Moreover, RLC was more effective on immediate reduction in pain after one session than the stabilization exercises, suggesting that realignment of the pelvis occurred using RLC and that mechanical stress on the ligaments and muscles around the SI joint was reduced. Thus, pelvic realignment with the device may have an additional effect over conventional stabilization exercises alone.
The immediate effects of stabilization exercises have not been discussed. The American College of Obstetricians and Gynecologists’ guidelines (34) recommends that an exercise programme involving walking, pelvic floor muscle exercise and stretching should be resumed gradually after delivery. However, there are no published studies to indicate the effects of exercises starting from day 1 or immediate effects on pain after 1 intervention session in the early period after delivery. The fact that the exercises with RLC reduced the pain immediately suggested that the mechanical stress on the ligaments and muscles around the SI joints was reduced. This will allow us to focus on future improvements, such as how the reduction in symptoms can be maintained more efficiently until the next session. Correction of asymmetrical motion of the SI joints to optimize the force closure mechanism is considered important (16, 34). RLC should improve pelvic alignment and may lead to further activation of local muscles to maintain the realigned pelvic position rather than letting the brain and muscles attain the optimal alignment. RLC may improve innominate sagittal rotation and stabilize the SI joints immediately, whereas it may be difficult to maintain the optimized position and stability of the SI joints if the tension of the fascia and the other structures, e.g. tension of the hip abductors pulling the iliac crest laterally, are separate from the SI joints. The primary outcome variables, decreased VAS score for pain and decreased PGQ score for difficulties in ADL, were not statistically different between the 3 groups.
PGQ and VAS were obtained using well-organized instructions explaining how to complete the form and answer each question so that the participants could understand the questions. All questionnaires and the manual booklet were completed as required. Pre-paid envelopes were provided to enable the participants to complete the questionnaires and post them to the investigators on time. Although a few participants posted the forms late, the response rate was over 90%. To decrease precision bias of the exercise intervention, an operation manual and instruction by an experienced physical therapist were provided, with the instructors teaching the exercises to the participants while they were in the clinic. In addition, an instruction video on YouTube was provided so that the participants could access it at any time. The exercise guidebook was provided to enhance understanding of the exercises. All participants considered it convenient to access the information. This study targeted only those women who had a natural birth. Caesarean birth was excluded because the pain of the incision may have confounded their perception of pain from the SI joints. The RLC device is a non-invasive intervention method to realign and stabilize the pelvis during a programme of standing exercises, which can be completed in 10 min.
A limitation of this study was the lack of detailed information on compliance at home after day 5. Although more than 80% of participants reported completion of the required intervention exercises, we did not obtain a record of how many times and how assiduously each participant performed the exercises. In order to optimize compliance, we contacted each participant every day in the clinic and once every 2 weeks by telephone or e-mail at home to encourage them to perform the required exercises for the 4-week period after delivery. Other limitations are that we did not use imaging data for the diagnosis, nor clinical physical examination to assess the pain and condition of the pelvis. Thus, the causes of the pain were unclear and the reasons for pain reduction were not identified.
An exercise programme with a pelvic realigning device (RLC: ReaLine CORE), designed to achieve a more symmetrical pelvis after delivery, resulted in immediate improvement and short-term improvement in postpartum PGP. Therefore, improvement in pelvic alignment after delivery may help decrease postpartum lumbar and pelvic pain. However, there were no significant differences between the exercises with the pelvic realignment device and pelvic stabilizing exercise. Further study is needed to determine the long-term effects of the exercises with the RLC on pain reduction and to improve the short-term effects. Furthermore, future research should include postpartum women in countries with different cultural backgrounds. Further research is also needed, using 3-dimensional magnetic resonance imaging (3D-MRI) or computed tomography (CT), to determine the effects of RLC on the alignment and conformity of the SI joints.
The authors would like to acknowledge nurses in the Nakagawa clinic, Ms Kyoko Hirokane, Ms Yasuko Masumune and Ms Otoe Tanaka, for their contribution to study recruitment and data collection. One of the authors (KG) is a founder and CEO of GLAB Corp. selling ReaLine CORE.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize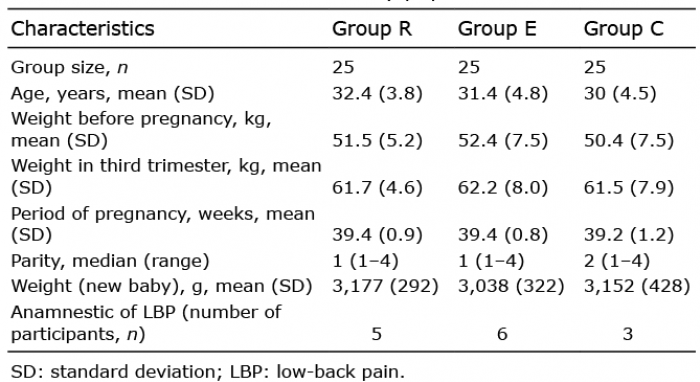 Click to show fullsize
Click to show fullsize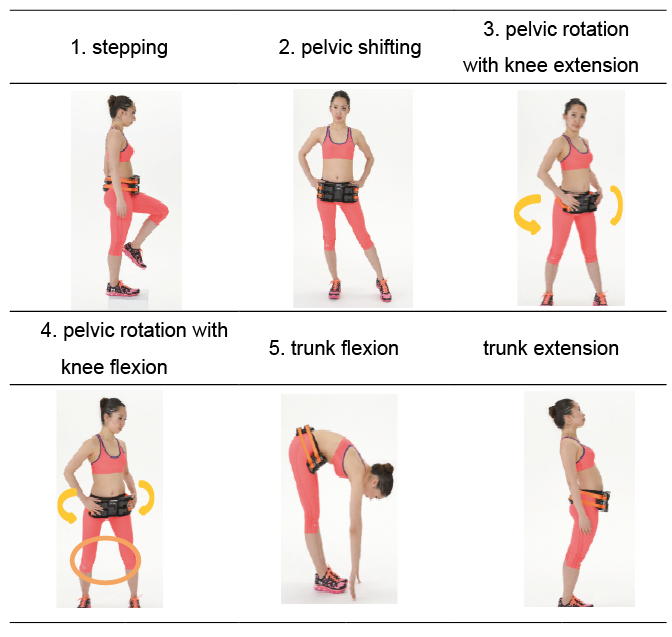 Click to show fullsize
Click to show fullsize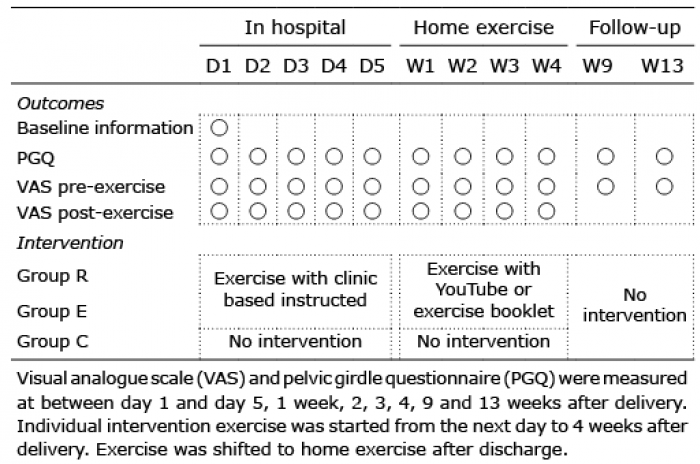 Click to show fullsize
Click to show fullsize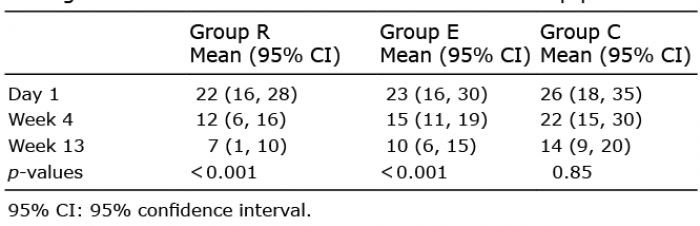 Click to show fullsize
Click to show fullsize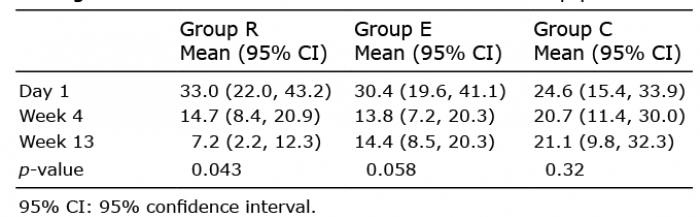 Click to show fullsize
Click to show fullsize