
From the 1Monash-Epworth Rehabilitation Research Centre, Epworth Healthcare, 2Monash Institute of Cognitive and Clinical Neuroscience, School of Psychological Sciences, Monash University, 3Department of Surgery, Central Clinical School, Monash University, 4National Trauma Research Institute, The Alfred & Monash University, 5School of Public Health and Preventive Medicine, Monash University, 6Centre for Health Economics, Monash Business School, Monash University, 7Department of Neurosurgery and 8Department of Trauma, The Alfred Hospital, Melbourne, Australia, 9Lee Kong Chian School of Medicine, Nanyang Technological University, Singapore, 10Melbourne Medical School, The University of Melbourne, 11Department of Emergency Medicine, Royal Melbourne Hospital, Melbourne, Australia and 12Faculty of Economics and Business, University of Groningen, the Netherlands
Objectives: Debate regarding factors associated with persistent symptoms following mild traumatic brain injury continues. Nested within a trial aiming to change practice in emergency department management of mild traumatic brain injury, this study investigated the nature of persistent symptoms, work/study outcomes, anxiety and quality of life and factors associated with persistent symptoms following injury, including the impact of receiving information about mild traumatic brain injuries in the emergency department.
Methods: A total of 343 individuals with mild traumatic brain injury completed the Rivermead Post-Concussion Symptom Questionnaire, Hospital Anxiety Depression Scale – Anxiety Scale, and Quality of Life – Short Form an average 7 months post-injury.
Results: Overall, 18.7% of participants reported 3 or more post-concussional symptoms, most commonly fatigue (17.2%) and forgetfulness (14.6%). Clinically significant anxiety was reported by 12.8%, and was significantly associated with symptom reporting, as were mental and physical quality of life scores. Significant predictors of post-concussional symptoms at follow-up were pre-injury psychological issues, experiencing loss of consciousness, and having no recall of receiving information about brain injury in the emergency department.
Conclusion: This study confirms that loss of consciousness and pre-injury psychological issues are associated with persistent symptom reporting. Not receiving injury information in the emergency department may also negatively influence symptom reporting.
Key words: mild traumatic brain injury; post-concussion symptoms; anxiety; quality of life.
Accepted Sep 4, 2018; Epub ahead of print Nov 14, 2018
J Rehabil Med 2019; 51: 00–00
Correspondence address: Jennie Ponsford, School of Psychological Sciences, Monash University, Clayton, Victoria, 3800, Australia. E-mail: jennie.ponsford@monash.edu
Loss of consciousness and pre-injury psychological issues are associated with persistent post-concussional symptom reporting. Not receiving information about mild traumatic brain injuries in the emergency department may also negatively influence symptom reporting.
Mild traumatic brain injury (mTBI) continues to present considerable controversy. mTBI commonly results in post-concussional symptoms (PCS) in the hours, days or weeks after injury. Whilst most patients have fully recovered within 1–3 months of injury, 15–25% of cases still experience symptoms 3 months post-injury, causing stress and disability (1, 2). Frequencies of persistent PCS vary with study recruitment criteria, setting and timing (3).
Most prospective studies have not followed up individuals with mTBI beyond 3 months post-injury. Of studies measuring PCS on the Rivermead Post-Concussion Symptom Checklist (RPQ) 6 or 12 months post-mTBI, rates of PCS have varied from 21% (4) to 49.8% (5) at 6 months, and from 27.3% (6) to 47.9% (5) at 12 months. Overall, there is limited agreement on when symptoms resolve (7).
Regarding predictors of persistent PCS, injury severity measures including GCS and PTA do not generally predict outcome following mTBI (1, 4, 8, 9), although recent studies (10, 11) show that higher GCS is associated with less symptom reporting. Loss of consciousness (LOC) has not reliably predicted outcome following mTBI. Intracranial abnormalities are associated with persistent PCS in some studies (12–15), but not others (10, 16). However, most mTBI patients do not show intracranial abnormalities and/or are not scanned. Of demographic predictors, female sex is associated with greater PCS (2, 5, 8–10, 17–20). Older age has been associated with persistent PCS in only 3 mTBI studies (20–22), whilst Van der Naalt et al. (10) found a non-linear relationship of age with PCS reporting. Of all pre-injury factors, presence of pre-injury mental health issues has been the strongest outcome predictor (2, 8–10, 22–24). Studies have also shown that concurrent anxiety and depression is associated with PCS reporting (4, 8, 10, 16, 25).
Limited evidence supports efficacy of interventions to reduce PCS following mTBI. Some evidence suggests provision of written information regarding expected symptoms and suggested coping strategies results in fewer reported PCS and lower anxiety 3 months post-injury (26–28).
The recently completed NET trial (29) examined the effectiveness of an implementation intervention to increase uptake of 3 recommendations for management of mTBI patients in emergency departments (ED): (i) prospective assessment of PTA using a validated tool; (ii) use of guideline-developed criteria to determine use and timing of computed tomography (CT) imaging; and (iii) provision of written patient information upon discharge from the ED. Control sites received access to an evidence-based clinical practice guideline without further implementation support. The present study utilized a cohort of patients participating in a follow-up component of this study (NET-Plus); first to describe long-term PCS symptoms, work/study outcomes, anxiety levels and quality of life in mTBI patients presenting to ED with GCS 14 or 15; and secondly, to identify factors associated with persistent PCS at follow-up, including the impact of receiving mTBI information in ED. It was hypothesized that persistent PCS would be reported in 20% of cases, and symptom reporting associated with age, sex, pre-injury mental health issues, concurrent anxiety, and recall of receipt of written information regarding the nature of expected symptoms.
The NET trial was a cluster randomised trial (CRT) involving 31 Australian EDs. The NET protocol has previously been published and this study only provides a brief overview of procedures relevant to the NET-Plus component of the trial (29).
The trial had 2 levels of hospital participation, designated NET and NET-Plus. EDs participating in NET measured clinical practice outcomes only, whereas EDs participating in NET-Plus assessed patient outcomes following discharge in a subgroup of individuals who agreed to be followed up from the larger cohort. This paper examines data from the NET-Plus cohort. Of the 31 EDs in the NET study, 24 agreed to participate in the NET-Plus trial and recruited participants. In this cohort, 10 EDs were allocated to the intervention and 14 to the control group. However, 7 control EDs reported receiving (limited) education regarding the management of mTBI as part of standard clinical education programmes or in-service training during the trial. One control site had an existing validated PTA assessment tool, administered by occupational therapists. For the current paper, the NET-Plus cohort was analysed as a single group. Trained chart auditors identified eligible candidates on the basis of 4 pre-defined inclusion criteria obtained from medical records: (i) aged 18 years or older; (ii) presented to the ED within 24 h of injury; (iii) sustained an acute blunt head trauma; and, (iv) documented a GCS score of 14 or 15 at presentation. Patients with penetrating injuries or non-traumatic brain injuries (e.g. stroke) were excluded. Eligible candidates were initially contacted by an ED staff member and invited to participate in a follow-up telephone interview. Exclusion criteria at this phase were: (i) non-English speaking background; (ii) limited hearing ability; (iii) cognitive impairment from intellectual disability and/or other neurological syndrome; and, (iv) severe substance use disorder and/or major psychiatric disorder requiring previous hospitalization. Interested candidates were posted an information sheet with a 2-week opt out option. After 2 weeks, consent was presumed and contact details were provided to researchers with clinical training and experience in conducting interviews with a brain trauma population. Researchers further screened for capacity to provide informed consent at interview commencement and calls were terminated if participants were intoxicated, distressed or impaired cognition was suspected. Overall, 343 participants were recruited into the study.
Ethical approval for the study protocol was granted by Alfred Health Human Research Ethics Committee (approval number 398/12). Local ethics was further obtained for each hospital site. Four attempts were made to contact consenting participants. Patient outcomes were collected through a structured telephone interview. The interview took approximately 15 min to complete and included questions on whether patient information was received in the hospital (see the following website for a copy of this information resource, which included information about expected symptoms and suggested coping strategies: https://www.monash.edu/medicine/psych/research-programs/merrc/resources), healthcare utilization since discharge (i.e. whether they visited healthcare facilities in the 4 weeks prior to the assessment for the head injury or another reason, and whether they had taken medication for headaches, anxiety, sleep issues or nausea), and return to work/study (i.e. status prior and post-injury). Pre-injury psychiatric history and substance use was documented by asking participants to answer yes or no to the following questions: “Have you ever had psychological/psychiatric problems?”, “Are you currently taking or have previously taken illicit drugs?”, and, “Has drinking alcohol ever disrupted your lifestyle?” The interview also included scales measuring PCS, anxiety and quality of life, discussed below. Participant responses were entered directly into the online database with real-time checks to minimize risk of error and missing data. Researchers conducting interviews received training and supervision in initial interviews to ensure standardized protocol delivery. Information regarding injuries (LOC, GCS, other injuries) and whether information had been given to patients was sought from medical records.
ussion Symptom Questionnaire (RPQ) (30) was used to assess symptom experience. Participants rated on a 5-point scale their experience of each of 16 symptoms at time of assessment (over the last 24 h), with 0 = symptom not present, 1 = symptom no more of a problem than pre-injury, and scores of 2, 3, and 4 reflecting mild, moderate and severe post-injury symptoms, respectively. Higher scores thus indicated greater severity of PCS. The overall score was computed by summing scores for all 16 items (range 0–64). A total score represented the sum of scores only if scores of 2, 3, or 4 were given, reflecting novel mild, moderate or severe post-injury symptoms respectively (range 2–64).
Secondary outcomes. The Anxiety scale of the Hospital Anxiety and Depression Scale (HADS) (31) was used to assess anxiety symptoms post-injury, since it has been shown to be sensitive in TBI populations (32, 33). HADS-Anxiety requires participants to rate on a 4-point scale (0–3) their experience of 7 symptoms over the past week, with total possible Anxiety score ranging from 0 to 21. A score >7 indicates clinically significant anxiety, with scores 8–10 indicating mild, 11–14 moderate and ≥15 severe anxiety.
The Quality of Life – Short Form (QoL SF-12) (34) questionnaire was used to assess quality of life post-injury. This includes 12 questions, 10 on a 5-point scale and 2 on a 3-point scale. Higher scores indicate better quality of life than lower scores. Physical functioning composite scores (PFCS) and Mental functioning composite scores (MCS) can be derived, with higher scores indicating greater functioning (mean 50 (standard deviation 10)).
Return to work/study outcomes were also documented. This included questions on whether participants were working/studying pre-injury (and for what hours) and at the time of the interview, and whether their duties or enrolment status had changed.
All analyses were conducted with SPSS v22 (SPSS Inc., Chicago, IL, USA) and Stata v12. For the RPQ, a total PCS score was computed for each participant, whereby scores of 0 and 1 were excluded based on the procedure adopted by King et al. (30) as 0 = symptom not present and 1 = symptom no more of a problem than pre-injury. An overall RPQ score was also computed including all scores. Overall RPQ scores were then dichotomized into no new post-injury symptoms vs. mild, moderate and severe symptoms for the prediction analysis. HADS anxiety scale scores were summed from response scores on HADS anxiety items. For the QoL questionnaire, separate physical functioning and mental functioning composite scores were generated and standardized according to Australian norms (35).
Descriptive statistics, including frequencies, were computed for all measures. χ2 analysis was conducted to determine whether there were differences in PCS reporting, based on recall of receipt of information at discharge from ED. Pearson’s correlation coefficient was calculated to estimate the linear correlation between PCS, HADS Anxiety and SF-12 QoL. A series of logistic regression models, accounting for the clustered nature of the sample arising from potential correlated responses of individuals within EDs, were conducted to identify factors associated with PCS reporting on the RPQ (i.e. mild, moderate or severe) vs. no new post-injury symptom reporting. Stata logistic regression with clustered/robust variance estimation is equivalent to performing a generalized estimated equations (GEE) analysis assuming an independence correlation structure (36). Predictive variables were selected based on previous research and available data, and included demographic variables (age and sex) in Model 1, premorbid psychological history/substance abuse variables in Model 2, injury-related variables (GCS, presence of LOC, time post-injury and other injury) in Model 3, and whether participants recalled having received information on discharge from ED in Model 4. Statistically significant predictors in each of these models, defined using a cut-point of p < 0.05, were then entered together into a final model (Model 5). Each of these models also controlled for which intervention the ED was allocated in the NET trial.
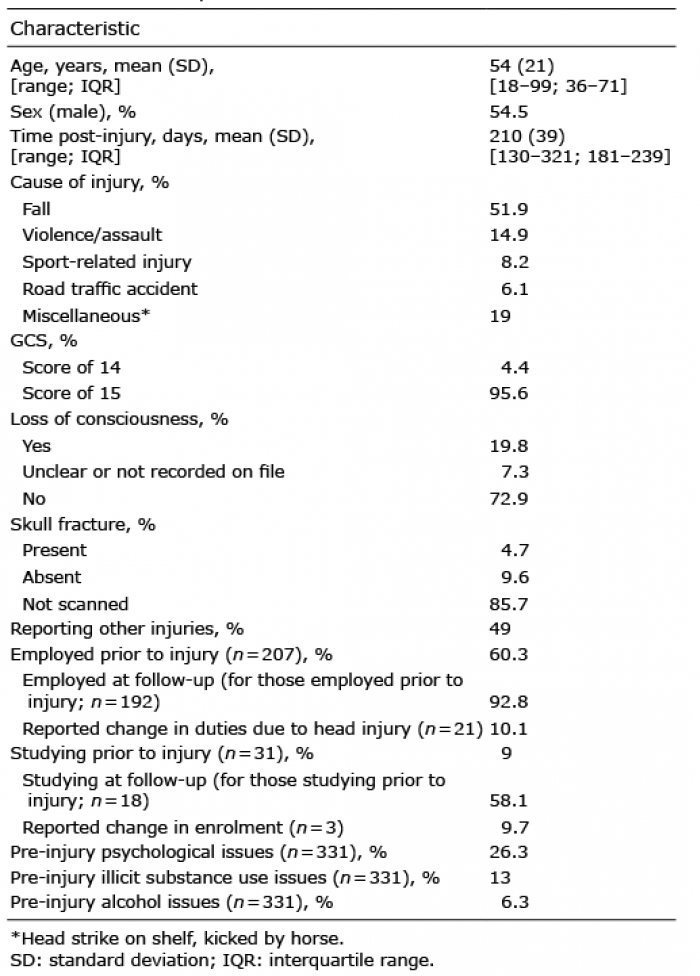
Of the 1,943 participants completing the NET trial, 536 consented to be contacted for the NET-Plus arm. Of these, 35 declined to proceed with interview, 16 were deemed not competent, and 119 were lost to follow-up (no response after 4 attempts). Interviews were completed by 366 participants, but data from 23 participants were excluded due to co-morbid neurological conditions. The subsequent NET-Plus sample included 343 participants. Details of this sample are shown in Table I. The demographic profile did not differ from the broader NET trial, where the mean age of participants was 51 years (for control group) and 54 years (for intervention group), and 45% were male. The predominant cause of injury for these 343 participants was incidental falls. In comparison with the rest of the NET trial sample, the NET-Plus sample were more likely to have a GCS of 15/15 (95.6% vs 87.6%; p = 0.000), but also more likely to have LOC (19.8% vs 17.1%; p = 0.001). Other injuries were documented in 49% of NET-Plus participants. The vast majority (92.8%) had returned to employment, with 10.1% indicating a change in duties due to the head injury, and 58.1% of those studying had returned to study, with 9.7% indicating a change in enrolment. Ninety-one percent of participants were discharged home after presentation to the ED, 5.5% were admitted to the ward, 2.9% were transferred to another hospital for treatment, and 0.6% went into police custody. There were 26.28% who reported pre-injury psychological issues, 12.99% illicit drug use and 6.34% alcohol problems pre-injury.
Table I. Participant characteristics of the NET Plus study. n = 343 unless otherwise specified
Of the 343 participants, 63.6% were in the NET trial control group and 36.4% in the intervention group. Of the 343, 28% said they could recall receiving information about mTBI at discharge, 12.8% were unsure or could not remember, and 59.2% indicated they did not receive information at discharge. In the CHART (i.e. medical) file, 39.9% of participants were documented as having had information provided at discharge, 1.7% having no information provided, 5.5% where it was deemed not applicable to provide information at discharge from ED (e.g. in case of admission to the ward), and in 52.8% of cases it was not recorded.
Table II shows mean scores on the RPQ, HADS and SF-12. The percentage of participants reporting novel post-injury PCS on the RPQ (mild, moderate or severe) is shown in Fig. 1. Three or more symptoms were reported by 18.7% of participants and 12.8% met International Classification of Diseases 10th (ICD-10) symptom criteria for PCS.
Table II. Summary statistics for each outcome measure
Fig. 1. Percentage of patients reporting novel post-injury symptoms at a mean of 7 months post-injury.
Participants reporting novel mild-severe symptoms were compared with those reporting no novel symptoms across 3 age groups. For the symptomatic group, 39.4% were < 40, 44.4% 40–64, and 26.7% > 65 years. χ2 analysis was significant, χ2 (2, n = 343) = 8.6, p = 0.014, with participants older than 65 years reporting fewer novel PCS.
There were 14.9% of participants who scored >7 on the HADS Anxiety scale, indicating clinically significant anxiety symptoms at follow-up, where 7.2% scored as mild, 5.6% moderate and 2.1% were severe. Anxiety was statistically significantly correlated with PCS after adjusting for cluster, whereby higher anxiety was associated with greater reporting of persistent novel post-injury PCS at follow-up (r = 0.52, p < 0.001, n = 343).
Quality of life on SF-12 was also significantly correlated with PCS, with lower mental health scores and to a lesser extent physical health scores associated with reporting of persistent PCS at follow-up (r = –0.49, p < 0.001 and r = –0.24, p < 0.001, respectively, n = 331).
Table III shows the percentages of participants who did and did not report novel mild–severe PCS at follow-up according to whether they did or did not report receiving information about mTBI and PCS at discharge from ED. χ2 analysis indicated that there was a significant difference, χ2 (2, n = 343) = 6.18, p = 0.046, with a higher percentage of participants who reported novel PCS post-injury indicating that they had not received information about mTBI and PCS at discharge from ED. Of participants unsure about whether they received information, a higher proportion did not report novel PCS.
Table III. Percentage of participants reporting symptoms following receipt of information at discharge from emergency departments
Results of each of the models are presented in Table IV. In Model 1 where demographic variables were entered, age was a statistically significant predictor, with younger age being associated with greater symptom reporting at follow-up. In Model 2 where premorbid psychological history/substance abuse variables were entered, the presence of premorbid psychological issues was a significant predictor of symptom reporting, whereby the odds of reporting novel PCS at follow-up in participants with these issues pre-morbidly were 2.75 times than those of participants without these issues. In Model 3 where injury-related information was entered, LOC was a statistically significant predictor, whereby the odds of reporting PCS at follow-up in those who had LOC recorded were 1.94 times than those for participants who did not have LOC. Furthermore, those with unclear or not recorded LOC reported novel PCS 2.52 times more than those with no LOC. In Model 4 where recollection of receiving discharge information was entered, it was found to be a statistically significant predictor. Those who did not recall receiving information at discharge reported PCS 2.65 times more than those who were unsure. However, those who recalled receiving information at discharge reported PCS 2.35 times more than those who were unsure of receiving information.
Table IV. Results from logistic regression models investigating predictors of novel post-injury symptom reporting, controlling for initial intervention study group and accounting for clustering of responses within emergency departments
In the final Model (i.e. Model 5), the presence of pre-morbid psychological issues, LOC and receipt of information were statistically significant predictors. Participants reported PCS 2.99 times more if they had pre-morbid psychological issues. If they had experienced a LOC, they reported PCS 2 times more than those who had not experienced a LOC; if LOC was questionable, participants reported PCS 2.47 times more than those who had not experienced a LOC. Participants who reported they did not receive information reported PCS 2.34 times more than those who were unsure. While participants who did recall receiving information at discharge reported PCS 2 times more than those who were unsure, this did not reach statistical significance in the final model.
The aims of this study were to document outcome in terms of reported PCS, return to employment/study, anxiety symptoms and health-related quality of life and identify factors associated with persistent PCS in a series of uncomplicated mTBI cases presenting to the ED and agreeing to follow-up. Whilst 63% of participants reported no persistent PCS at follow-up, 18.7% reported 3 or more symptoms at follow-up, an average of 7 months post-injury, and 12.8% met criteria for an ICD-10 diagnosis of PCS. The most common symptoms were fatigue, forgetfulness, slowed thinking and sleep disturbance, followed by lowered frustration tolerance, irritability, depression, headaches and dizziness. These patterns of persisting symptoms are consistent with those found in previous longitudinal studies (4–6, 22, 37). Overall, however, the rates of PCS were low compared with many previous studies and the severity of reported symptoms was generally in the mild to moderate range. Rates of return to employment or study were high, with 92.8% of those employed pre-injury still working at follow-up, but only 60% of pre-injury students studying at follow-up. This may be partly explained by some students having completed studies. Rates of anxiety symptoms were low. Consistent with previous studies (8, 10), there was a statistically significant association between presence of persisting novel PCS and anxiety symptoms, as well as with mental and to a lesser extent physical quality of life on the SF-12. That is, individuals who reported lower QoL also reported persisting novel or worsening PCS.
Of the predictive factors examined, 3 were significantly associated with persistent PCS: premorbid psychological issues, LOC, and having no recall of receiving information at discharge from ED. Older age was associated with less PCS reporting than in the middle or younger age-groups, but this was not a significant predictor in the final model. The strongest predictor, namely premorbid mental health issues, has been associated with persistent PCS in numerous studies to date (2, 8–10, 23, 24, 38). It has been speculated previously that individuals with a pre-injury psychiatric history may respond to the experience of mTBI and PCS with greater anxiety, which may, in turn, exacerbate their PCS (37). The association of anxiety with PCS reporting supports this premise and is consistent with recent findings by van der Naalt et al. (10).
Nevertheless, the presence of LOC was also associated with persistent PCS, suggesting that the severity of the injury did also contribute to persistent symptoms in this study. The study sample had relatively mild injuries, with only 19.8% having any reported LOC. Previous studies have shown mixed findings, but many have not examined LOC as a predictor, or not found it to be a significant predictor (9). Some previous studies of mTBI outcomes have only included cases with some LOC (2, 8, 37), whereas others have also included a substantial majority without documented LOC (4, 24). From the results of the present study, it would appear that the occurrence of LOC may be an important injury severity marker. The duration of LOC has possibly proven less useful in previous studies, due to variability in methods of its measurement (7, 9).
Finally, it was apparent that a higher percentage of participants who reported novel PCS post-injury reported not receiving information about mTBI and PCS at discharge from ED than those who were unsure. Of participants unsure about whether they received information, a higher proportion did not report novel PCS than did. This lends some support to the use of such information. Although an inexpensive and relatively simple form of intervention, the results of our recently completed implementation trial suggested that achieving reliable distribution of such information is extremely difficult1. However, it also needs to be pointed out that those who did recall receiving the information did not report significantly fewer symptoms that those who did not recall it at this long time after injury.
1Bosch M, McKenzie JE, Ponsford J, Turner S, Chau M, Tavender EJ, et al. Evaluation of a targeted, theory-informed implementation intervention designed to increase uptake of emergency management recommendations regarding adult patients with mild traumatic brain injury: Results of the NET cluster randomised trial. PLoS Med (in submission).
This study had limitations and results need to be viewed in light of several factors. All predictive models accounted for only a small proportion of the variance, suggesting that there are other factors accounting for reporting of PCS at follow-up that were not measured in the current study (e.g. maladaptive coping (10), post-injury neuropsychological functioning (9), and presence of neck pain in the ED, PCS and post-traumatic stress at 2 weeks post-injury (39)). The participants in this study had very mild injuries, with more than 80% having no LOC and 95.6% having a GCS of 15/15 on presentation to the ED. In part this reflected the fact that only patients with GCS of 14 or 15 were included in the study. However, 85.7% were not scanned, making it possible that some complicated mTBI participants were included in the study, which could have confounded the results. The mean age of participants of 54 years was older than that seen in most mTBI samples, with a higher than usual proportion of women and of injuries due to falls. This may reflect that the participating EDs in this study were predominantly short stay units rather than trauma centres, where many large mTBI studies have historically been conducted and more complex trauma cases are likely to be included, with more associated injuries other than mTBI and potential for post-traumatic stress. This highlights the importance of considering sampling methods in relation to findings from mTBI studies. Only a small proportion of EDs approached agreed to participate in the NET trial and these were predominantly short-stay units rather than trauma centres. This may have influenced the rates of symptom reporting for the above-mentioned reasons. Furthermore, follow-up took place at a wide-ranging interval of 130–321 days post-injury. Whilst time post-injury was not associated with symptom reporting, this relatively long delay after injury may have influenced reliability of recall of information provided. Although all intervention centres were instructed to use the designated information booklets, we cannot be sure that they provided this information rather than some other form of information. Finally, there are limitations related to data collection via the telephone; namely, the inability to control the participant’s environment or see their body language.
Overall, this study has identified that the majority of individuals presenting to EDs with uncomplicated mTBI (GCS 14–15) make a good recovery. A relatively small, but significant, proportion (18.7%) have significant persisting problems. They are more likely to have had a history of psychological disturbance and/or lost consciousness. Not being able to recall receiving information about expected symptoms and how best to deal with them may result in greater long-term reporting of PCS. The study has implications for clinical practice. Screening for history of psychological disturbance and careful documentation of LOC in the ED are important indicators of risk of potential persistent symptoms that could be implemented. Provision of information about potential PCS with suggested coping strategies is an inexpensive intervention that may minimize PCS.
The authors would like to thank all the hospital emergency departments (ED) involved in this study, in particular the ED staff who recruited patients for this study. We would like to also thank all MERRC staff who conducted the follow-up interviews. This study is part of a 5-year grant (the Neurotrauma Evidence Translation (NET) Program), funded by the Victorian Transport Accident Commission (TAC), Australia. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize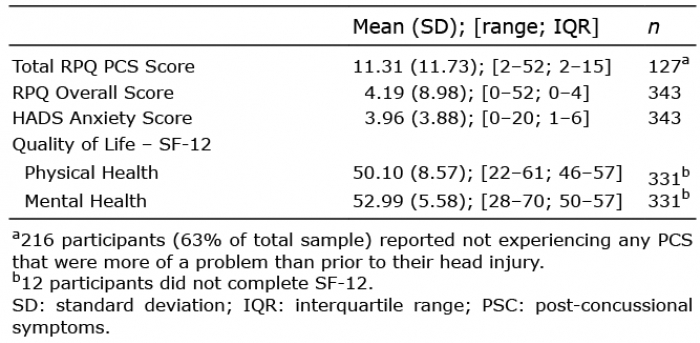 Click to show fullsize
Click to show fullsize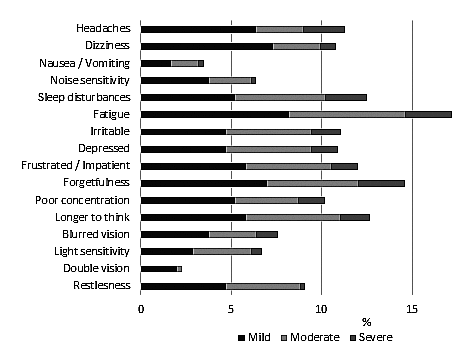 Click to show fullsize
Click to show fullsize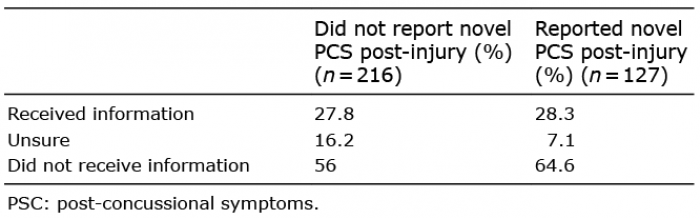 Click to show fullsize
Click to show fullsize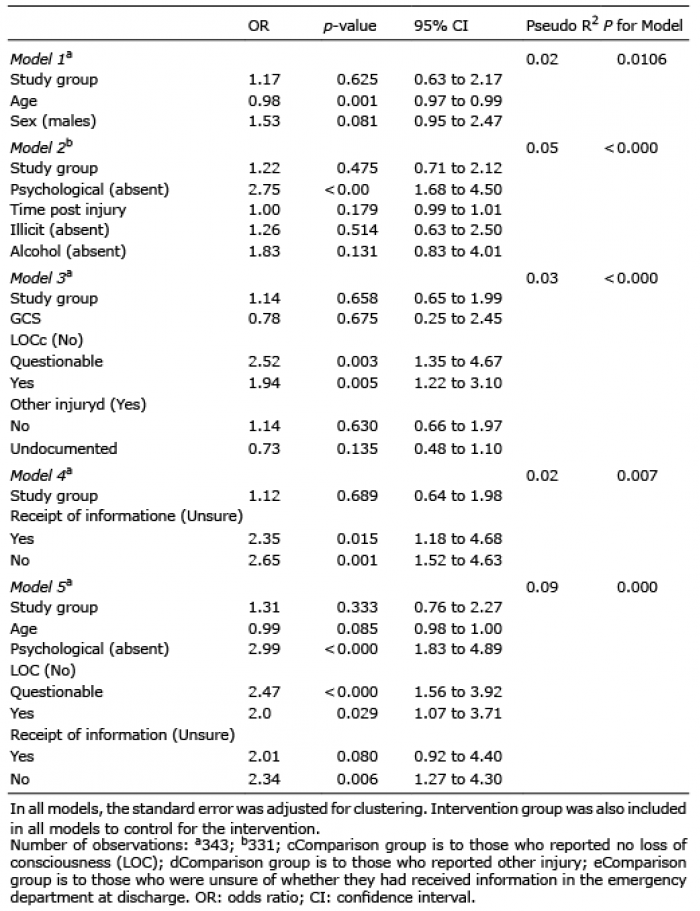 Click to show fullsize
Click to show fullsize