
From the 1Roessingh Research and Development, 2Department of Biomechanical Engineering, TechMed Centre, University of Twente 3Department of Biomedical Signals and Systems, TechMed Centre, University of Twente, 4Medisch Spectrum Twente, Medical School Twente, 5Department of Research Methodology, Measurement and Data Analysis, University of Twente, and 6Roessingh Center for Rehabilitation, Enschede, The Netherlands
Objective: To determine: (i) whether the use of ankle-foot orthoses over a period of 26 weeks affects tibialis anterior muscle activity; (ii) whether the timing of provision of ankle-foot orthoses (early or delayed) affects the results; (iii) whether the provision of ankle-foot orthoses affects tibialis anterior muscle activity within a single measurement.
Design: Randomized controlled trial.
Subjects: Unilateral hemiparetic subjects, a maximum of 6 weeks post-stroke.
Methods: Subjects were assigned randomly to early (at inclusion; week 1) or delayed provision of ankle-foot orthoses (8 weeks later; week 9). Tibialis anterior electromyography was measured with and without ankle-foot orthoses, in study weeks 1, 9, 17 and 26.
Results: A total of 26 subjects were analysed. In a single measurement, use of an ankle-foot orthosis significantly reduced the activity levels of the tibialis anterior muscle during the swing phase (p = 0.041) compared with walking without an ankle-foot or-thosis. During the 26-week follow-up, no changes were found in tibialis anterior muscle activity in the swing phase without an ankle-foot orthosis, both within-groups (p = 0.420 early; p = 0.282 delayed), and between-groups (p = 0.987). After 26 weeks, no differences were found in tibialis anterior muscle activity between both groups in the swing phase, with (p = 0.207) or without ankle-foot orthoses (p = 0.310).
Conclusion: Use of ankle-foot orthoses post-stroke reduced tibialis anterior muscle activity in the swing phase within one measurement; however, long-term use of ankle-foot orthoses for 26 weeks did not affect such activity. Early or delayed provision of ankle-foot orthoses did not affect the findings. The results indicate that there is no need to fear negative consequences on tibialis anterior-activity because of long-term AFO-use (early) after stroke.
Key words: ankle-foot orthosis; stroke rehabilitation; muscle electromyography; tibialis anterior; long-term effects; timing of provision; randomized controlled trial.
Accepted Sep 22, 2018; Epub ahead of print Oct 26, 2018
J Rehabil Med 2019; 51: 00–00
Correspondence address: Corien Nikamp, Roessingh Research and Development, Roessinghsbleekweg 33b, NL-7522 AH Enschede, The Netherlands. E-mail: c.nikamp@rrd.nl
Ankle-foot orthoses (AFOs) are often used to improve walking after stroke. However, it is unknown whether early or later provision of AFOs affects muscle activity, and what are the effects of long-term AFO use after stroke. Some clinicians fear that early use of AFO after stroke has negative effects on muscles around the ankle. Therefore, we studied the effect of AFO use on the tibialis anterior muscle in 26 subjects after stroke. Subjects were prescribed an AFO in week 1 of the study, or 8 weeks later. Muscle activity was measured 4 times over a period of 26 weeks. We found that AFO use reduced muscle activity levels compared with walking without an AFO within 1 measurement. However, long-term use of an AFO for a period of 26 weeks did not affect muscle activity. These effects were the same for the subjects provided with the AFO in week 1 or 8 weeks later. This study did not find any negative effects on activity of the tibialis anterior muscle with long-term use of an AFO early after stroke.
Walking function is often impaired after stroke (1). Insufficient foot-clearance during the swing phase is an important alteration contributing to limited walking function post-stroke. Activity of the tibialis anterior (TA) muscle is important for foot-clearance. In healthy subjects, the TA becomes active just before foot-off in order to lift the foot during the swing phase, peaking during early swing (2). A second burst of activity controls pre-positioning before initial contact and controls plantarflexion during the loading response.
Ankle-foot orthoses (AFOs) are often provided post-stroke to improve foot-clearance in swing (3), although the optimal timing of provision after stroke is unclear (4). Some clinicians are reluctant to prescribe AFOs post-stroke as they fear AFOs may result in disuse of muscles, in particular the TA muscle (3, 5, 6). Several studies compared walking with and without AFOs (5–9). Within a single session a decrease in electromyography (EMG) of the TA muscle was found during walking with AFOs (5–8). Only one study included a follow-up period (8). Geboers et al. (8) found immediate reduced activity of the ankle dorsiflexors of 7% in patients with peripheral paresis, calculated over the whole step cycle. Six weeks of AFO use, however, did not change EMG activity levels. Therefore, they concluded that AFO use is safe, even for recently paretic patients. It is not known whether AFO use over a longer period of time after stroke has negative effects. Furthermore, it is not known whether early or late provision of AFOs post-stroke affects muscle activity.
The aim of this study was to determine the long-term effects of AFO use on muscle activity of the TA muscle. The primary aim was to determine whether AFO use affects TA muscle activity over a period of 26 weeks within subjects provided with AFOs early or delayed after stroke. Secondly, between-group differences in TA muscle activity were measured for early and delayed provision of AFOs. Thirdly, whether provision of AFOs affects TA muscle activity within a single measurement session was determined when walking with and without AFOs.
In agreement with previous literature, it was hypothesized that AFO use decreases TA muscle activity during the swing phase, comparing walking with and without AFOs within a measurement. However, it was also hypothesized that TA muscle activity over time would not be affected by AFO use, and it was not expected that timing of AFO provision would influence the results.
Study data were collected as part of a single-centre, randomized controlled, parallel group study, which aimed to study the effects of different timing of provision of AFOs. The study was approved by the medical ethics committee Twente, registered in the “Nederlands Trial Register”, number NTR1930, and followed the CONSORT guidelines (10). All subjects provided written informed consent.
Subjects were recruited by the main researcher between December 2009 and March 2014, follow-up continued until 2015. Stroke subjects were recruited from the Roessingh Centre for Rehabilitation in Enschede, the Netherlands. Inclusion criteria were: (i) unilateral ischaemic or haemorrhagic stroke leading to hemiparesis (single and first-ever stroke or history of previous stroke with full physical recovery); (ii) minimum 18 years; (iii) maximum 6 weeks post-stroke; (iv) receiving in-patient rehabilitation care at inclusion; (v) able to follow simple verbal instructions; (vi) indication for AFO use (i.e. abnormal initial floor contact and/or problems with foot-clearance in swing and/or impaired ability to take bodyweight through the paretic lower limb in stance) determined by the treating rehabilitation physician and physiotherapist. Exclusion criteria were: subjects with severe comprehensive aphasia, neglect or cardiac, pulmonary or orthopaedic disorders that could interfere with gait.
An independent person allocated participants to 1 of the 2 intervention groups using stratified block-randomization: (i) AFO provision at inclusion, in study week 1 (early group); or (ii) AFO provision 8 weeks later, in study week 9 (delayed group). Randomization was performed with sealed envelopes in blocks of 4 with a ratio of 1:1. Stratification was based on the Functional Ambulation Categories (FAC) (11). Walking with (FAC 0–2) and without (FAC 3–5) physical support of another person at inclusion were used as stratification categories before randomization.
Subjects were provided with 1 of 3 commonly used types of off-the-shelf, non-articulated, posterior leaf design, polyethylene or polypropylene AFOs; flexible, semi-rigid or rigid (Basko Healthcare, Zaandam, the Netherlands). The type of AFO was chosen in week 1 (early group) or week 9 (delayed group). AFO-fitting was performed by a licensed orthotist. AFO type was chosen according to a custom-developed protocol (12). Besides the AFO-intervention, all subjects received usual care from experienced physiotherapists according to the Dutch guidelines for physiotherapy after stroke (13, 14).
Measurements were performed 4 times in both groups and were planned in week 1 (T1), 9 (T2), 17 (T3) and 26 (T4) of the study. T1 and T2 correspond with the point in time at which the AFO was provided in both groups. The 8 weeks between T1 and T2 were also incorporated between T2 and T3, T4 was planned as follow-up measurement after 26 weeks. The measurements required that subjects were able to walk without physical support of another person (FAC ≥ 3) and had sufficient endurance to complete a measurement. If this was not the case, the measurement was postponed until these requirements were met. Measurements were performed with and without AFO in randomized order. Subjects in the delayed group did not use an AFO at T1 and were therefore measured at T1 without AFO only.
At inclusion, basic demographic data were recorded. Actual AFO use was assessed for every measurement. Measurements were performed in a gait laboratory. Muscle activation pattern of the TA muscle was assessed using surface EMG (sEMG), using a wireless 16-channel Biotel 99 EMG-amplifier (Glonner, Munich, Germany) with a cut-off frequency of 600 Hz/–3 dB and a first order 17-Hz high-pass filter. Arbo sg93 electrodes (Covidien, Mansfield, MA, USA) were used and electrode-placement and skin preparation were according to the SENIAM protocol (15). Subjects walked on a level walkway over a distance of 8 m at self-selected walking speed, wearing their own shoes. sEMG electrodes were not removed between measurements with and without AFO. Assistive devices (such as cane or quad stick) were allowed and subjects were allowed to rest between the trials if necessary.
Raw sEMG-signals were digitized at 1,000 Hz sampling rate with 16-bits resolution and stored on a VICON MX13+ motion-analysis system (Vicon, Oxford, UK). Simultaneously with the sEMG-recordings, 3D gait-analysis was recorded, using a 6-camera Vicon MX13+ motion-analysis system for capturing marker trajectories. Reflective 25-mm markers were placed directly on the skin and shoes, according to the modified Helen Hayes marker-set. Marker trajectories of the foot were used to manually determine initial contact (IC) and foot-off (FO). Marker trajectories of the left and right anterior superior iliac spine along the axis of progression were averaged and used to calculate walking speed.
Data-processing was performed using custom in-house software, developed in Matlab (MathWorks, Natick, MA, USA). sEMG data were first band-pass filtered with cut-off frequencies of 25 and 450 Hz. After processing, data were manually checked for artefacts. If artefacts were found, the specific gait cycle was removed from the analysis. Subsequently, sEMG data were rectified and smoothened using a low-pass filter with cut-off frequency of 10 Hz and split into 4 sub-phases of gait using foot-events (IC and FO) of both sides: (i) first double support (DS1), from IC to opposite FO; (ii) single support (SS), from opposite FO to opposite IC; (iii) second double support (DS2), from opposite IC to FO; (iv) swing (SW), from FO to IC. Once the data were segmented into the 4 sub-phases, each sub-phase was time-normalized to 100%. These time-normalized sub-phases were used to calculate the area under the curve (AUC) to express the activity level per sub-phase.
The primary outcome measure was TA activity during swing, as the swing phase is the main sub-phase of gait in which TA activity is shown during normal walking to evoke foot-clearance (2). The secondary outcome measure was TA activity during the other sub-phases. Outcomes were calculated for each of the 4 measurements T1–T4, with and without AFO. Walking speed without and with AFO was calculated, since walking speed is known to affect EMG (16).
SPSS version 19 (IBM SPSS Statistics, Chicago, IL, USA) was used for data analysis. The level of significance for all analyses was set at p < 0.05. No power calculation was performed, since relevant data regarding timing of AFO provision were not available. Because TA activity per sub-phase did not show a normal distribution, logarithmic transformations were performed prior to statistical testing.
Baseline data, including TA activity of both groups at T1 without AFO, were compared using independent samples t-test/Mann–Whitney U test for continuous variables and χ2 test/Fisher’s exact test for categorical variables, as appropriate.
Mixed-model repeated measures analyses were performed, both within-groups to study whether AFO use affected TA muscle activity over a period of 26 weeks, and between-groups over time, in order to assess a group-by-time interaction. Both analyses included walking speed as a confounder. The analyses included data of all 4 measurements (T1, T2, T3, T4). Since data of 4 measurements was available only without AFO (the delayed group did not yet use an AFO at T1), the mixed-model analyses were performed for data without AFOs only.
Between-group effects after 26 weeks were studied comparing the data of both groups using the independent samples t-test, both for the without and with AFO condition.
The third objective was to determine whether AFO provision decreased TA muscle activity when walking with and without the AFO was compared within a single measurement session. In order to be able to compare these results with those of previous studies (mainly including subjects with chronic stroke), data of the total (early and delayed) group at T4 were included in this analysis. A paired-samples t-test was used to compare data with and without AFO.
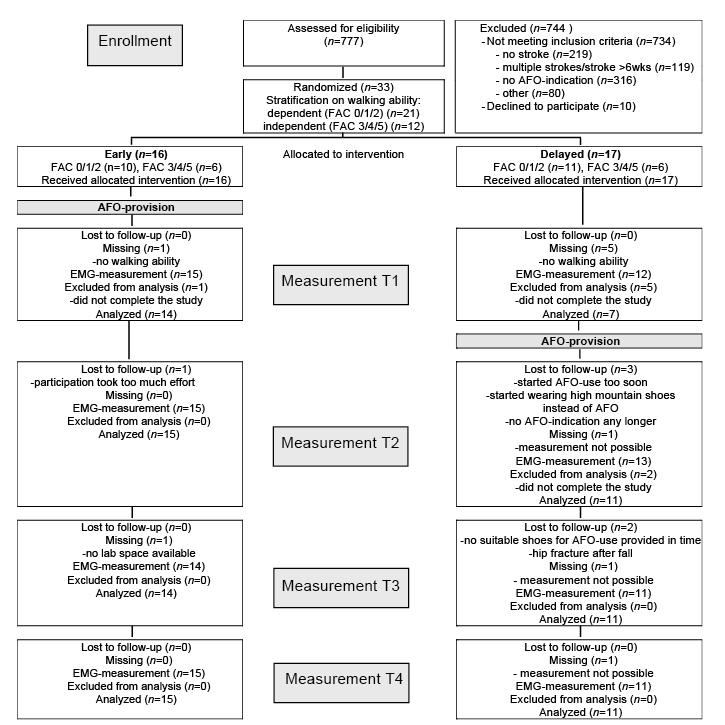
Fig. 1 details the participant flow through the study. Thirty-three subjects (16 early, 17 delayed) were included in the study. Of these, 26 subjects (15 early, 11 delayed) were included in the analysis. Six subjects (1 early, 5 delayed) did not complete the study (drop-out after T1 or T2). They were not included in the analysis since their data was insufficient to answer the research questions (missing T4). One additional subject (delayed) was excluded, since it was not possible to perform the measurements (measurements were too tiring). Of the included 26 subjects, 5 (1 early, 4 delayed) were not able to perform T1, as they were not able to walk without physical support from another person and/or had insufficient endurance to complete T1. In 19 of the 21 subjects who were able to perform T1, measurements had to be postponed with 1–5 weeks, resulting in T1 being performed approximately 51 days after stroke (see Table I). In general, measurements T2, T3 and T4 could be performed as planned. Data for 1 subject (early) is missing at T3 because no laboratory space was available.
Fig. 1. CONSORT flowchart. The figure shows the participant flow through the study. AFO: ankle-foot orthosis; FAC: Functional Ambulation Categories.
Table I. Subject characteristics
Table I shows the subject characteristics. No statistically significant differences were found between the groups at inclusion. The type of AFO provided, and whether subjects use their AFO in daily life was registered. Most subjects were provided with a flexible type of AFO (Table I). One subject (early) changed from a flexible to a semi-rigid AFO between T1 and T2, as the rehabilitation physicians judged that the flexible AFO did not provide enough support any longer. All subjects used their AFO daily at the time of the measurements at T1, T2, T3 and T4, except for 3 subjects (2 early, 1 delayed) at T4. These 3 subjects used their AFO during some days of the week at T4, mainly during walking outdoors for longer distances. These subjects were measured both with and without AFO at T4.
The median number of gait cycles used to calculate the average AUC per sub-phase was ≥ 9 for each measurement and group. Baseline comparison at T1 did not reveal significant differences in TA muscle activity without AFO (n = 14 early; n = 7 delayed), except for TA muscle activity during the second double support phase (p = 0.016). No differences in walking speed without an AFO were found at baseline (0.37 vs 0.39 m/s for the early and delayed group, respectively, p = 0.804).
Table II and Fig. 2 show the median AUC for TA activity of the early and delayed group at T1, 2, 3 and 4 for the different phases in gait. The original data without logarithmic transformation are shown.
Table II. Area under the curve (AUC) of the tibialis anterior muscle and walking speed for the early and delayed group (T1–T4); the mixed model repeated measures analysis within and between groups; and the independent samples t-test between the early and delayed group at T4
Fig. 2. Boxplots of tibialis anterior area under the curve (AUC) without ankle-foot orthoses (AFO). AUC is presented per sub-phase, for the early (left) and delayed (right) group separately. Circles and asterisks represent outliers and extreme outliers, respectively
No changes in TA muscle activity were found during the 26-week period in SW without AFO in both groups (mixed-model repeated measures analysis within-groups p = 0.420 and p = 0.282 for the early and delayed group, respectively). During the other sub-phases of gait, significant changes were found only for DS1 and SS in the delayed group (p = 0.013 and p = 0.007, respectively).
After 26 weeks (T4), no differences in TA muscle activity between both groups were found in SW (independent samples t-test p = 0.310 and p = 0.207 for without and with AFO, respectively) or any of the other sub-phases of gait (p ≥ 0.192 in all cases). Furthermore, mixed-model repeated measures analysis between-groups shows that changes in TA activity during the 26-week follow-up period were not different between the early and delayed group in SW (p = 0.987) or any of the other sub-phases of gait (see Table II).
TA activity without and with AFO were compared at T4 for the total group (n = 26) to study the effects of AFO use within a measurement. AFO use significantly lowered TA activity in SW (p = 0.041) compared with walking without an AFO. No effects are found in the other sub-phases of gait (p = 0.398, 0.696 and 0.407 for DS1, SS and DS2, respectively).
This study shows that AFO use after stroke decreases TA muscle activity during swing within a single measurement session, without negatively affecting TA muscle activity over 26 weeks.
The results comparing TA muscle activity with and without AFO are in accordance with our hypothesis and in agreement with previous studies comparing the effects of AFOs in the swing-phase during a single measurement session (5–7).
Based on the results of previous studies assessing the effects of AFO use only at a certain point in time, AFO use was suggested to decrease the activation of muscles around the ankle, thereby encouraging disuse of these muscles (3, 5, 6). Consequently, AFO use was thought to worsen the existing loss of strength and possibly delay recovery (8), resulting in permanent gait impairments and AFO dependence (6). To our best knowledge, the present study is the first to assess the long-term effects of AFO use after stroke. No changes were found in AUC of the TA in swing during the follow-up period of 26 weeks while walking without AFO, for subjects either in the early or delayed group. Significant changes in AUC in SS were found for the delayed group. Post-hoc analysis revealed that AUC at T3 differed significantly from T1 and T2, showing higher levels at T3. We have no explanation for this increase at T3. Significant changes were also found in DS2, but post-hoc analysis did not reveal any significant differences between individual measurements. The results for the swing phase did not show any negative effects of long-term AFO use on TA muscle activity post-stroke. This is in accordance with a study by Geboers et al., which included patients with peripheral paresis (8). They found reduced activity of ankle-dorsiflexors with AFO within a single measurement session, but 6 weeks of AFO use did not lead to a general lower level of EMG activity. To explain our results, studies suggest that the possible negative effects of AFOs on muscle activity in a single gait cycle might be counteracted by the fact that AFOs improve walking in general (6, 8). An increase in amount of walking (steps taken) is suggested to offset a decrease in EMG during a single step (6).
Ideally, one would need a long-term longitudinal randomized controlled trial, including a control group with no AFO use to determine whether long-term use of AFOs affects TA muscle activity after stroke. How-ever, this is not feasible for ethical reasons. Instead, groups were provided with an AFO early or delayed after stroke, which was found not to influence results. We already reported positive effects of AFO provision on ankle kinematics early after stroke (17), while no effects of early vs delayed AFO provision on pelvis, hip and knee kinematics were found after 26 weeks (18). At the same time, beneficial effects of AFO provision were found on functional levels (12). After 26 weeks no differences with respect to balance and mobility were found between early and delayed provision, but early provision showed favourable outcomes in the first 11–13 weeks, possibly resulting in earlier independent and safe walking (19). For clinical practice, this means that clinicians, together with the patient, can decide when to start AFO treatment based on personal priorities and preferences. Early AFO provision is expected to provide beneficial effects on a functional level in the short-term, without negatively affecting muscle activity of the TA in the long-term.
An important strength of the study is that this is the first to measure the effects of AFOs on muscle activity of the TA in a longitudinal study-design post-stroke. Furthermore, subjects were included early (within 6 weeks) after stroke, both with independent and dependent walking ability at the start of the study. Thereby, our study conditions match with the situation in which clinicians often consider AFOs in daily clinical practice.
This study has some limitations. First, the sample size was relatively small, and this was limited further at T1, since not all subjects were able to perform this measurement at that time. Secondly, the longitudinal design included 4 separate EMG measurements during the 26-weeks follow-up period. Changes in electrode-position may arise and could affect results. This was limited, since a standard protocol was used to define electrode positioning (15). Changes in measurement conditions are inevitable in a longitudinal design including subjects early after stroke. This includes changes in the use of walking aids and shoes during the follow-up period. Although we tried to limit variation as much as possible, changes in walking aids and shoes between measurements could have affected our results (20). The results may also be affected by the use of different types of AFOs in our study. However, because of the small sample size, a sub-group analysis per type of AFO was not possible. Furthermore, walking speed increased during the study, which is known to affect EMG (16). Therefore, walking speed was included as confounder in the mixed-model analyses. Post-hoc analysis revealed that walking speed did not differ between both groups after 26 weeks. Finally, it was not possible to blind subjects and assessor for AFO use.
Within a single measurement session, AFO use lowers TA muscle activity in the swing phase when walking with AFO is compared with walking without AFO. However, long-term AFO use for a period of 26 weeks after stroke does not affect TA muscle activity. Furthermore, early or delayed provision of AFO does not affect the results. The results clearly indicate that there is no need to fear negative consequences on the level of muscle activity of the TA muscle because of long-term AFO use (early) after stroke.
The authors would like to thank the patients and staff from the Roessingh, Center for Rehabilitation, Enschede, the Netherlands, and staff from Roessingh Rehabilitation Technology, Enschede, the Netherlands for their participation and co-operation in the study. Furthermore, the authors would like to thank Basko Healthcare for providing the AFOs.
This work was supported by grants from the Ministry of Health, Welfare and Sport, the Netherlands; and “Stichting Hulpfonds Het Roessingh”.
Conflicts of interest: The AFO used in this study were provided by Basko Healthcare, Zaandam, the Netherlands. Basko Healthcare was not involved in designing the study, collecting data or the analysis and interpretation of data. In addition, they had no role in writing the article and the decision to submit the article for publication.


 Click to show fullsize
Click to show fullsize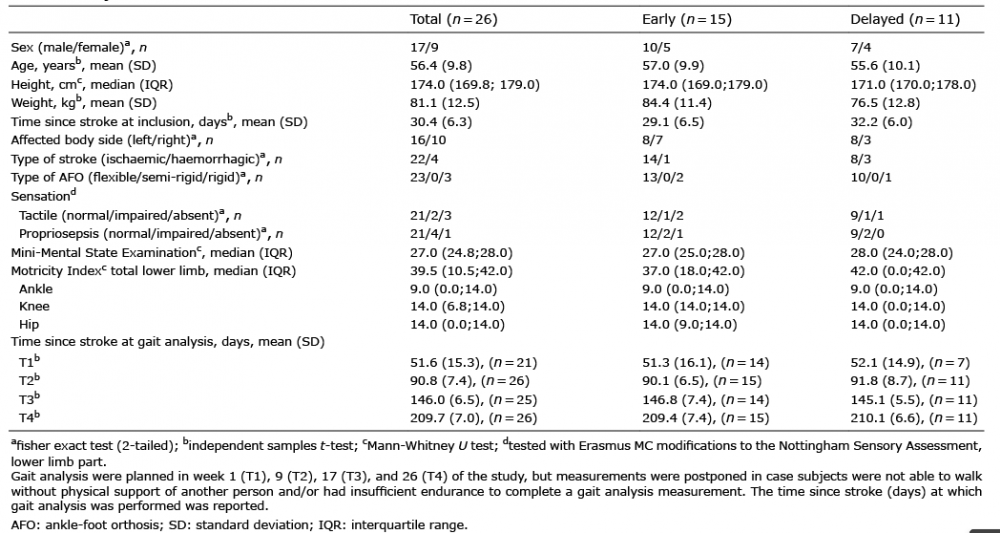 Click to show fullsize
Click to show fullsize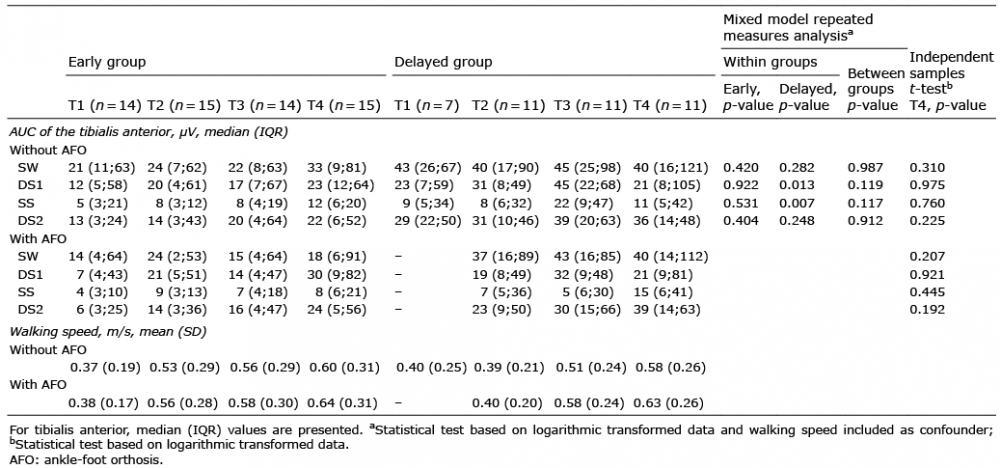 Click to show fullsize
Click to show fullsize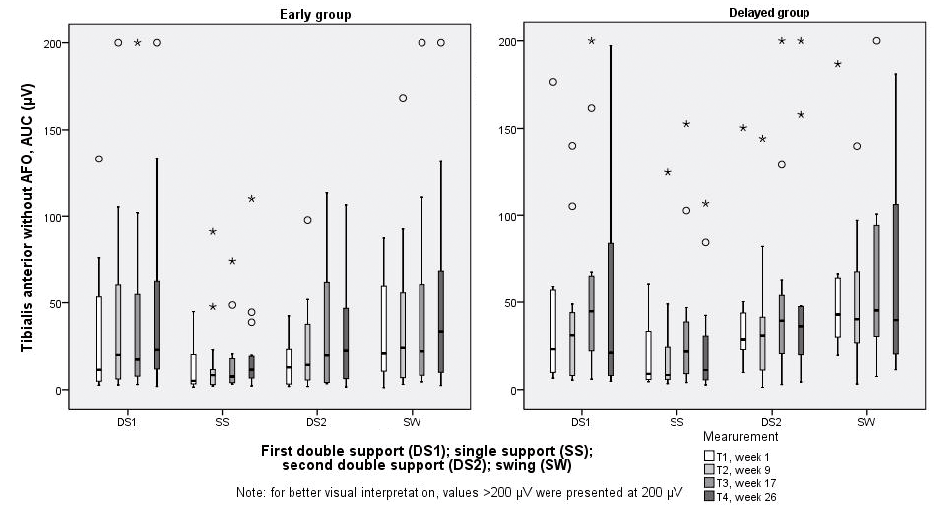 Click to show fullsize
Click to show fullsize