
From the 1Department of Rehabilitation and Brain Trauma, Division of Clinical Neurosciences and 3Department of Physical and Rehabilitation Medicine, Turku University Hospital and University of Turku, and 2Department of Biostatistics, University of Turku, Turku, Finland
Objective: To compare easy-to-use International Classification of Functioning, Disability and Health (ICF)-based measures of functioning with the level and severity of spinal cord injury.
Methods: Cross-sectional study. Patients (n = 142) and their significant others completed the 12-item World Health Organization Disability Assessment Schedule (WHODAS 2.0) questionnaire. A physician at the university hospital outpatient clinic assessed functioning with the 7-item World Health Organization (WHO) minimal generic set.
Results: The patient and proxy WHODAS sum score was rated severe with decreasing severity in groups with complete and partial tetraplegia and paraplegia, respectively. Working ability was rated most severely impaired in the tetraplegic groups. Between-group differences were also found in mobility, household tasks, and self-care. Mobility was found to be associated with lesion severity; life activities, participation and friendships with lesion level; and self-care and WHODAS sum score with both lesion severity and level. Depending on the level and severity of spinal cord injury, a moderate to strong correlation was found between the sum scores of the 2 tools, and mostly very strong correlations between patient and proxy assessments of functioning.
Conclusion: Both generic ICF-based tools, despite their briefness, seemed to be useful as they were able to differentiate various levels and severities of spinal cord injury. We recommend using the 12-item WHODAS 2.0 when planning individualized services for patients with spinal cord injury.
Key words: disability; ICF; severity; spinal cord injury; WHO minimal generic set of domains of functioning and health; WHODAS.
Accepted Oct 3, 2018; Epub ahead of print Nov 8, 2018
J Rehabil Med 2019; 51: 00–00
Correspondence address: Sinikka Tarvonen-Schröder, Division of Clinical Neurosciences, Turku University Hospital, PO Box 52, FIN-20521 Turku, Finland. E-mail: sinikka.tarvonen-schroder@tyks.fi
Two easy-to-use validated International Classification of Functioning, Disability and Health (ICF)-based tools, the 12-item patient and proxy World Health Organization Disability Assessment Schedule (WHODAS 2.0) and the 7-item World Health Organization minimal generic set used by a physician, were found to be reliable and useful in assessing functioning in patients with spinal cord injury. These tools can, with little effort, be used to detect activity limitations and participation restrictions, and differentiate various severities and levels of spinal cord injury. As the minimal generic set is brief and limited, we recommend using the 12-item WHODAS 2.0 when planning individualized services for patients with spinal cord injury.
Spinal cord injury (SCI) is a major cause of long-term disability (1–9), with increasing prevalence rates unless measures are taken to control incidence (2). It has been estimated that the prevalence of non-traumatic SCI may overtake traumatic SCI in the next decades (6). In the light of previous studies, patients with non-traumatic SCI seem to reach the same functional outcomes as those with traumatic SCI (1, 4). With improved acute care and greater life expectancies after SCI, the focus of management has shifted to interventions aiming to improve functioning, quality of life and involvement in life situations. The ultimate aim of rehabilitation is for patients to reach optimal participation despite their disabilities.
Different instruments have been used to evaluate the severity of SCI, patient’s needs and treatment effects (10–13). Some of these outcome measures do not address functional relevance (11). Priorities in developing appropriate functioning instruments for patients with SCI include understanding the dimensions of participation, and the importance of both objective and subjective measures (10). Only a few studies, however, have tested participation instruments, such as WHODAS 2.0, in individuals with SCI, and there is still a lack of studies comparing self-rated functioning with more objectively defined parameters (14–19). Other difficulties in measuring functioning lie in a redundancy of instruments for different health conditions and tools that are too time-consuming for clinical settings. Among ICF-based tools developed by the WHO (20), the 2 shortest validated generic assessment scales are the 7-item minimal generic set of domains of functioning and health (21) and the 12-item World Health Organization Disability Assessment Schedule (WHODAS 2.0) (22). These 7- and 12-item scales evaluate different items in the “activities and participation” section of the ICF. While participation is a crucial outcome of SCI rehabilitation (10, 23–25), brief validated measures to evaluate participation are needed.
As far as we know, there are no studies comparing these 2 tools, the WHODAS 2.0 and the WHO minimal generic set, in assessing functioning in patients with SCI of different severities and injury levels. The objective of this study was to compare the utility of these 2 brief scales in assessing functioning in SCI.
This observational cross-sectional study was conducted between November 2015 and November 2017. The 12-item WHODAS 2.0 and personal background information (age, sex, accommodation, marital status, educational level, and working status) questionnaires, along with informed consent and information regarding the study were posted to 240 consecutively referred patients with SCI (diagnosis according to the ICD-10 criteria) and their significant others 2 weeks before their visit at a specialist outpatient clinic of a university hospital. The outpatient clinic both evaluates patients with recent SCI and takes care of patients with past SCI with ongoing problems and rehabilitative needs. A total of 160 patients responded, of whom 18 were excluded because they did not fulfil the inclusion criteria (age under 18 years at the time of the SCI, a current major medical or psychotic condition or another neurological diagnosis, and inability to understand, co-operate, or complete the questionnaire or complete recovery without residual symptoms). Of the 142 participants, 85 had also responses from their significant others; of whom 61 (72.6%) were spouses, 3 (3.6%) parents, 6 (7.1%) children, 3 (3.6%) siblings, 1 (1.2%) other relative, 3 (3.6%) close friends, and 7 (8.3%) trained caregivers.
Clinical information (date of diagnosis and comorbidities) was gathered from the hospital records, and the total number of comorbidities was counted (26, 27). The level and severity (grade) of SCI was classified according to the American Spinal Cord Injury Association (ASIA) (28). In this article, the term tetraplegia is used to describe the change in motor and/or sensory function when the injury is at the level of the cervical segments. The term paraplegia is used when the lesion is more caudal. A specialist in physical and rehabilitation medicine at the outpatient clinic completed the 7-item WHO minimal generic set aiming at assessing the level of functioning in a simple and validated way (21).
The 12-item patient and proxy WHODAS 2.0 includes 12 items assessing 6 disability domains during the previous 30 days: cognition (learning and concentration), mobility (standing and walking), self-care (washing and dressing oneself), getting along (dealing with strangers and maintaining friendships), life activities (doing housework and working ability), and participation (emotional functions and engaging in community). Each of these 12 items is rated according to a 5-point Likert-type scale, which grades the difficulty experienced by a participant in performing a given activity. Each of the 12 items is scored from 0 to 4, where 0 means no (0–4%), 1 means mild (5–24%), 2 means moderate (25–49%), 3 means severe (50–95%), and 4 means extreme or complete (96–100%) difficulty in this specific activity. The total score of WHODAS is the sum of all these 12 sub-scores, ranging from 0 to 48, with lower scores indicating better functioning. Total scores of 1–4 indicate mild disability, 5–9 moderate disability, and 10–48 severe disability (14, 15, 22, 29, 30).
The WHO minimal generic set consists of 7 ICF domains: energy and drive functions, emotional functions, sensation of pain, carrying out daily routine, walking, moving around, and remunerative employment. Generic means that this assessment scale is applicable to all people despite their health conditions. Minimal means that the scale consists of the least number of domains of functioning that can be used to explain significant differences between people with health issues. The scoring system is similar to WHODAS, the sum score ranging from 0 to 28, with lower scores indicating better functioning (21).
The comparison between the 4 patient groups according to severity and level (tetraplegia AIS A–B and C–D and paraplegia AIS A–B and C–D) was carried out within categorical variables using χ2 test, or, in the case of small cell frequencies, Fisher’s exact test. In numerical variables the comparisons between the 4 patient groups was carried out either by 1-way analysis of variance (ANOVA), or by the non-parametric Kruskal–Wallis test if the distribution of an outcome variable was too skewed. The Spearman’s correlation coefficient was used to test the correlation between variables. Patient and proxy WHODAS responses were analysed pairwise; the patients with only 1 value were excluded. The correlations of 0–0.30 were considered weak, 0.31–0.50 moderate, 0.51–0.70 strong, and greater than 0.70 very strong. No adjustment for multiple comparisons was done, since in this exploratory study the search for patterns is more important than formal statistical significance. In order to reach enough statistical power we set a minimum target number of patients to 140. Statistical analyses were performed using SAS 9.4 for Windows. p-values below 0.05 (2-tailed) were considered statistically significant.
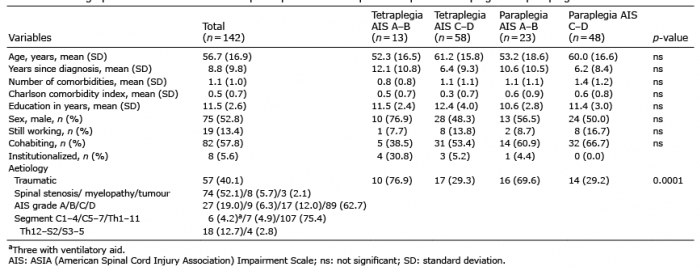
Demographic and clinical background data for all 142 participants are shown in Table I. To compare background data in different levels and severity groups of SCI, participants were divided into 4 groups: (i) complete tetraplegia AIS A–B (n = 13), (ii) partial tetraplegia AIS C–D (n = 58), (iii) complete paraplegia AIS A–B (n = 23), and (iv) partial paraplegia AIS C–D (n = 48).
Table I. Demographic and clinical data for the participants with complete and partial tetraplegia and paraplegia
When disability was rated by a physician (Table II), disabilities were severe in all patient groups, and patients with a complete tetraplegia were rated the most disabled. In all groups, energy and emotional functions were rated mildly impaired, pain moderately, daily activities at least moderately, and employment severely impaired. The total disability (sum score of the generic set) and 4 of the 7 separate functions were more impaired in those with a complete motor plegia (AIS A–B, n = 36) than in those with a partial plegia (AIS C–D, n = 106). When those with a cervical lesion (tetraplegia, n = 71) were compared with those with a more caudal lesion (paraplegia, n = 71), no between-group differences were found.
Table II. Physician-rated generic set scores by severity and level of spinal cord injury
When functioning was rated by patients and their significant others (WHODAS 2.0, Table III), the total disability score showed severe impairment in all patient groups. Difficulties reported in cognition, participation, and relationships remained mild, with the exception of moderate impairment in community life in those with a partial tetraplegia. All patient groups reported severe difficulties in standing, walking, and working ability, the restrictions being most severe in those with tetraplegia. When comparing tetraplegic and paraplegic groups, similar between-group differences were also found in household activities and self-care. When the ratings of those with a complete lesion (AIS A–B) were compared with those with a partial lesion (AIS C–D), a complete lesion was associated with more difficulties in getting around and self-care, and a partial lesion with participation difficulties.
Table III. Functioning assessed with patient and proxy WHODAS 2.0 by severity and level of injury
The Spearman correlations of the 6 patient-rated WHODAS domains with SCI severity (AIS grade), lesion level, walking ability, current working status, and physician-rated functioning (generic set sum score) are shown in Table IV. The correlation between the patient-rated WHODAS sum score and the physician-rated generic set sum score was moderate in all other patient groups, except for a strong correlation in the group with AIS D tetraplegia. The generic set sum score was correlated with all other WHODAS domains (0.26–0.56) except cognition.
Table IV. Spearman Correlations of patient-rated World Health Organization Disability Assessment Schedule (WHODAS) domains with spinal cord injury severity (AIS grade), level, walking ability, working status, and physician-rated functioning
The correlation coefficient between patient and proxy WHODAS sum scores was very strong (0.89) with strong to very strong correlations in single items except for the item “dealing with strangers” with only a moderate correlation. The significant others rated both the total disability (sum score) and the items learning, emotions and dressing as slightly more impaired than did the patients themselves. Cronbach’s alpha value for reliability of the WHODAS patient sum was 0.86, the WHODAS significant other 0.86 and the minimal generic set sum 0.75.
These results support the utility of both generic measures WHODAS 2.0 and the WHO minimal generic set in assessing functioning of patients with SCI. The degree of perceived impairment (WHODAS sum score) was found to increase from incomplete paraplegia through complete paraplegia and partial tetraplegia to complete tetraplegia, respectively.
In our study population, participants typically had hardly any problems in cognition, emotions or relationships. The most severe impairments were found in getting around and life activities, followed by self-care, these results being largely in line with previous studies in SCI (15–17, 31, 32). Participation, on the other hand, was rated less severely impaired among our participants, the restriction being only mild in all other groups except those with a partial tetraplegia. Obviously, the ratings do not strictly measure the level of functional capacity, but evaluate the level of actual performance in real-life situations and also reflect environmental factors, e.g. the amount of assistance and aids, support and services the patients receive in the community, as in previous studies (13). Unexpectedly, those with an incomplete SCI lesion were found to experience more difficulties in community life than those with a complete lesion. Our hypothesis is that, if people with a complete lesion and more severe symptoms get daily help from trained caregivers, those with a milder injury with no such aid may experience more restricted participation than those with a more severe or complete injury. The groups with a partial lesion were also 7–9 years older than the other 2 groups with a complete lesion, which could have some influence on the results even if the age difference was not statistically significant.
These results show that participants with a cervical lesion (partial or complete tetraplegia) experience more impairments in self-care and life activities, including the ability to work, than those with a lower lesion, which is in agreement with previous studies (18, 33–35). It is natural that, when those with a complete motor lesion were compared with those with an incomplete lesion, a complete lesion was associated with more difficulties in getting around and self-care. In our study, inability to walk was correlated with other impairments (getting around, self-care, participation and cognition) as in previous studies, which found wheelchair-dependency (36, 37) and mobility restrictions (17) to increase difficulties in other domains of participation (17, 37) and to decrease quality of life (36). Also, current employment was found to be associated with other domains (mobility, self-care, and life activities) in our study population. These findings are, in many aspects, in agreement with the only previous WHODAS study evaluating these associations between objective and subjective parameters in SCI (17).
The correlation between the assessments made by a physician (the WHO minimal generic set) and by the patients themselves (WHODAS) was moderate to strong. This study is in line with previous studies showing this kind of positive correlation between WHODAS 2.0 and other measures of activity limitations (30), in our study the WHO minimal generic set. As the correlations between the patient and proxy WHODAS scores on the whole and in single items were mostly very strong, it seems possible that, when assessing functioning in patients with SCI who do not have cognitive problems or concomitant neurological diseases, as in our study, the patient is able to make assessments reliably without reflecting his or her opinion with that of his or her significant others.
Although the physician who rated functioning using the generic set score was not blinded to background information, their ratings seemed reasonable, and might be even more reliable due to their good insight into the clinical history of the participants. Physician-rated functioning was correlated more clearly with lesion severity, walking ability and current employment status than when rated by the patients themselves. A physician rated the overall functioning severely impaired in tetraplegia and more moderately in the other 3 groups, showing between-group differences also in mobility and daily activities. The fact that working ability was rated more impaired by a physician than by the patients is interesting. Few of the patients were actually employed. Patients may have a more subjective view of employment possibilities and the functioning ability they still possess with diverse voluntary work possibilities, as a physician may think more of the real requirements in the open labour market reflected with the activity restrictions and participation limitations the patients may have.
In this study, both WHODAS and the WHO minimal generic set were found to differentiate varying severities and levels of SCI from each other. Previously, WHODAS has been shown to be useful in assessing disability in several health conditions, both in psychiatric and somatic conditions. While the burden of more time-consuming functioning tools is challenging for clinicians and patients, these simple tools appeared to be practical and useful in our clinical setting. In the wide field of rehabilitation of patients with SCI, developing cost-effective client-centred rehabilitative services is important. In this development, it is essential to assess perceived functioning, patients’ needs and participation restrictions using reliable tools. Although previous recommendations regarding evaluating functioning have suggested using the 7-item WHO minimal generic set together with other wider ICF-based tools, based on our results we would also recommend using the 12-item WHODAS 2.0 alone. It is, however, possible that the 12-item WHODAS is not adequate in finding between-group differences in mobility of patients with SCI, as the description of the mobility items in WHODAS includes “walking a long distance” and “standing a long time”, which are not usually possible for any patients with SCI (38). In contrast, the 7-item minimal generic set does not define the time or the distance of these activities thus allowing better clinical adjustment of moving difficulties than WHODAS. Even if WHODAS has many advantages, it does not substitute for other generic measures of both capacity and performance (capability without and with assistance) in real-life situations. In an outpatient clinic, as in our study, keeping the number of separate items minimal probably ensures the compliance of patients to complete the assessment scale. The 7-item WHO minimal generic set may, however, be too brief if used as the only functioning measure. When planning individual rehabilitative services for patients with SCI and their significant others, we primarily recommend using the 12-item WHODAS 2.0 as a screening tool.
Limitation
One limitation of the study is a cross-sectional design preventing confirming causal relationships of disability. Even if we included all consecutive 142 patients, the study population of a tertiary outpatient clinic is always selected. Even if the severity and level of the SCI was evaluated retrospectively, we had access to electronic patient records from the beginning of the medical history. As 2 different generic functioning scales (WHODAS and the WHO minimal generic set) were used, straight comparisons were not possible for all sub-items. Both measures are, however, ICF-based and have many identical items. Even if WHODAS and the WHO minimal generic set seemed to be adequate in the chronic phase as in our study, these results are not directly generalizable to the acute or subacute phase (39). Patients and their significant others were not blinded to each others’ evaluations; however, in the vast majority their responses differed from each other.
Both ICF-based tools were easy to use in assessing functioning in SCI. Of these 2 tools, we recommend using the 12-item patient-completed WHODAS 2.0, as this can, with little effort, be used to detect activity limitations and participation restrictions in SCI, and to differentiate between various severities and levels of SCI, when planning rehabilitative services.
The study was approved by the ethics committee of the University and University Hospital (19.5.2015, 73/2015). The ethical standards of the World Medical Association Helsinki Declaration of 1975, as revised in 1983, were followed.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize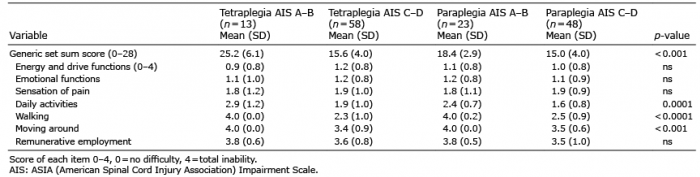 Click to show fullsize
Click to show fullsize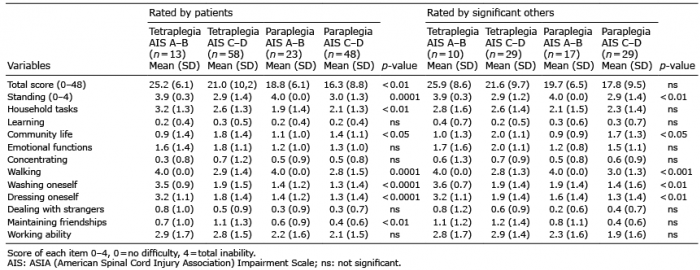 Click to show fullsize
Click to show fullsize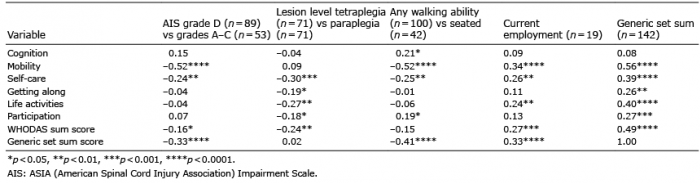 Click to show fullsize
Click to show fullsize